

 PDF
PDF ePub
ePub Citation
Citation Print
Print



서론
척추는 골 전이 중 가장 흔한 부위이며, 전체 전이 중에서는 폐와 간에 이어 3번째로 흔한 부위이다(12). 암으로 사망하는 환자의 약 30~70%는 사후 검사에서 척추 전이가 있었으며, 약 14%의 환자는 이환 기간 동안 척추 전이로 인한 증상을 경험하게 된다(3). 척추 전이의 주요 임상 증상은 국소적인 통증 혹은 신경근 통증이며, 운동성 약화, 감각 상실 및 괄약근 통제 상실 등의 증상을 동반하거나 동반하지 않을 수도 있다. 암 환자가 통증이나 신경 증상을 호소하는 경우 가장 적절한 치료를 시작하기 위해 병변의 존재, 수 및 범위를 평가하기 위해 영상의학적 평가가 반드시 선행되어야 한다.
자기공명영상(이하 MRI)은 오랫동안 척추와 척수 전이 평가를 위한 유용한 방법으로 오랫동안 인식되어 왔으며(4), 특히 척추 전이의 조기 진단을 다른 검사들보다 용이하게 하는 것으로 입증되었다(567). 미국 영상의학과 의사협회(American College of Radiology; 이하 ACR)는 허리 통증이 있는 암 환자의 평가를 위해 조영 증강을 포함하지 않은 MRI를 통한 평가를 권고하였다. 그러나, 어떤 MRI 프로토콜이 척추 전이의 평가에 가장 적합한지에 대한 표준적 합의는 아직 부족한 상태이다(8910).
확산강조영상(diffusion weighted image; 이하 DWI)은 악성 종양의 평가에 있어서 여러 장기에서 유용성이 입증되었다(1112). 또한, 척추 압박 골절에 대한 평가에서 병적 골절(pathologic fracture)과 양성 골다공증성 골절(benign osteoporotic fracture) 사이의 감별에 DWI가 도움이 된다는 보고가 있었고(13), 전신의 골 전이 평가에 기존의 MRI에 DWI를 추가하였을 때 도움이 된다는 보고도 있었다(14). 또한, 척추 전이 병변에 대한 치료 반응의 평가에 DWI가 도움이 된다는 보고도 있었다(15).
본 연구에서는 척추 전이 여부의 평가에서 DWI의 유용성에 대해 평가하는 것을 목표로 하였다.
대상과 방법
본 연구는 본원 연구윤리위원회(Institutional Review Board)의 승인 하에 진행되었고, 후향적 연구로 정보 제공자 동의서는 면제되었다(IRB No. B-1806-472-107).
2017년 7월부터 8월 사이에 본원에서 전이암 진단 및 평가를 위하여 척추 MRI를 촬영한 환자들 중 DWI를 포함한 환자는 총 64명이었다. 이들 중 암 환자로 확진되지 않은 환자 5명을 제외하였고, 척추 혹은 척수의 원발 암으로 확진된 환자 7명을 제외하였고, 척추 전이 여부를 평가하기 위한 목적이 아닌 환자들 4명을 제외하였다(Fig. 1). 임상 소견은 전자의무기록을 참고하였으며 나이, 성별, 원발 종양에 대해 검토하였다.
최종적으로 31명의 남성(평균 연령: 62.2세, 연령 분포: 10~83세)과 17명의 여성(평균 연령: 60.5세, 연령 분포: 11~87세)의 총 48명의 자기공명영상이 포함되었다(평균 연령: 61.6세, 연령 분포: 10~87세).
원발 종양은 폐암(n = 10), 전립선암(n = 10), 유방암(n = 6), 위장관계 기원의 악성 종양(n = 4), 두개 내의 악성 종양(n = 4), 신장암(n = 2), 림프종(n = 2), 요관암(n = 2), 비인두암(n = 2), 간암(n = 1), 방광암(n = 1), 담낭암(n = 1), 담관암(n = 1), 난소암(n = 1), 후두암(n = 1) 이었다.
자기공명영상 프로토콜
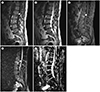
연구 대상 환자 48명의 영상은 3.0-Tesla 자기공명영상 촬영기(Ingenia, Philips Healthcare, Best, the Netherlands)로 획득하였다. 척추 전이 여부 평가를 위한 기존의 전 척추(whole spine) MRI 프로토콜(conventional MRI)은 다음과 같다: T1 강조 시상면 터보 스핀 에코[T1-weighted sagittal turbo-spin-echo (이하 TSE)] [repetition time (이하 TR)/echo time (이하 TE), 400~650/10 msec; slice thickness, 4 mm; slice gap, 0.4 mm; field of view, 25~40 cm; matrix, 440 × 429], T2 강조 축상면 터보 스핀 에코(T2-weighted sagittal TSE) (TR/TE, 3400~4400/120 msec; slice thickness, 8 mm; slice gap, 2 mm; field of view, 25~40 cm; matrix, 440 × 413), 그리고 T1 강조 축상면 터보 스핀 에코(T1-weighted axial TSE) (TR/TE, 400~650/10 msec; slice thickness, 8 mm; slice gap, 2 mm; field of view, 25~40 cm; matrix, 440 × 429).
조영 증강 영상은 지방억제 T1 강조 터보 스핀 에코(T1-weighted multiecho dixon TSE)영상을 얻었고, 시상면(TR/TE, 450~650/15 msec; slice thickness, 4 mm; slice gap, 0.4 mm; field of view, 25~40 cm; matrix, 352 × 391; mean acquisition time, 6 minutes 47 seconds) 및 축상면(TR/TE, 400~650/15 msec; slice thickness, 8 mm; slice gap, 2 mm; field of view, 15 cm; matrix, 304 × 260; mean acquisition time, 6 minutes 54 seconds)에 대해 얻었다. 조영제는 0.1 mmoL/kg Gd-DPTA (Magnevist; Schering, Berlin, Germany)로 정맥 주사하였다.
확산강조영상은 다발에코평면영상(multi-shot echo planar imaging)을 시상면에 대해 얻었다(TR/TE, 2255/62~84 msec; slice thickness, 4 mm; slice gap, 0.4 mm; field of view, 25~37 cm; matrix, 148 × 97; b = 1000 s/mm2; mean acquisition time, 4 minutes 1 seconds).
영상소견 분석
3명의 영상의학과 의사(reader 1, 척추 영상 분야에서 17년간의 경력을 가진 영상의학 전문의, reader 2, 척추 영상에서 7년간의 경험을 가진 영상의학 전문의, reader 3, 척추 영상에서 9개월의 경험을 가진 영상의학 전공의)가 MRI를 후향적으로 검토했다. 각각의 영상의학과 의사들은 MRI를 독립적으로 해석하였고, 척추 전이 평가를 위한 MRI라는 정보만 제공받았다.
각각의 영상의학과 의사는 각 환자의 척추 자기공명영상을 2회 판독하였다. 2회의 판독은 2개의 다른 MRI 프로토콜에 대한 평가를 반영하였다; 첫째, 기존의 MRI 프로토콜(conventional, T1 및 T2 강조 영상과 조영 증강 영상), 둘째, conventional에 DWI를 추가한 프로토콜. 동일한 환자에 대한 2회의 판독 세션은 2주 이상의 시간 간격을 두고 진행하여 리콜 편차(recall bias)를 줄였다. 두 번째 세션에서는 첫 번째 세션의 판독 보고서를 검토하거나 참고하지 않았다.
2회의 판독 세션에서 모두 척추 전이 여부에 대한 평가는 척추 분절(spinal segment)의 수로 기록되었고, 각각의 분절에 대해 신뢰등급(confidence rating)을 3개의 등급으로 나누어 점수화하여 기술하였다: 비교적 분명하게 전이가 의심되는 경우(probably metastasis: 2), 전이 여부가 애매한 경우(doubtful: 1), 비교적 분명히 전이가 없을 것으로 판단되는 경우(probably benign: 0). 하나의 척추 분절(spinal segment)은 전방에 위치한 척추뼈몸통(vertebral body)과 척추뒤고리(posterior element)로 나누어 평가하였다.
2회의 판독 세션에서의 영상 분석은 선행 연구에서 척추 전이를 시사하는 것으로 보았던 소견을 근거로, 척추 전이 여부의 판단에 있어 최대한 실제 판독에 가깝게 수행하였다. 첫 번째 판독 세션에서는 1) T1 강조 영상에서 병변이 디스크를 기준으로 그보다 낮은 신호 강도를 보일 경우, 2) 모든 영상에서 병변 내부의 해면뼈(trabecular bone)가 소실되었을 경우, 그리고 3) 조영 증강 영상에서 강한 조영 증강을 보일 경우의 세 가지 기준을 원칙으로 하여 비교적 분명하게 전이가 의심되는 경우(probably metastasis: 2)로 판독하였다(1617181920). 또한, T2 강조 영상에서 달무리 징후(halo sign)가 보이는 경우, 모든 영상에서 척추 주위 조직으로의 침윤이 보이는 경우에는 전이를 의심할 수 있는 소견으로 참고하였다.
앞서 언급한 소견들이 보이지 않거나, 반대되는 소견을 보일 경우 비교적 분명히 전이가 없을 것으로 판단되는 경우(probably benign: 0)로 판독하였으며, 이러한 소견들이 모호할 경우 전이 여부가 애매한 경우(doubtful: 1)로 판독하였다.
두 번째 판독 세션에서는 첫 번째 판독 세션에서의 기준을 동일하게 적용하였고, 이에 더하여 병변이 낮은 apparent diffusion coefficient 값을 보이며, 확산 제한(diffusion restriction)을 보일 경우 전이를 의심할 수 있는 소견으로 참고하였다(1315). 영상의학과 의사(reader 3)는 자기공명영상 촬영 시점으로부터 6개월 이내에 이루어진 척추의 단순촬영(plain radiograph)과 컴퓨터단층촬영 영상(이하 CT)에 기반하여 척추 전이의 유형을 평가했다. 척추 전이의 유형은 골용해성(osteolytic), 골형성성(osteoblastic), 복합성(mixed)으로 구분하였다(21).
영상의학과 의사(reader 3)는 DWI의 질을 평가하였는데, DWI에서 허상에 의해 가려지는 척추 분절의 수를 해부학적 높이[vertebral level: 경추(C), 흉추(T), 요추(L), 천추(S)]에 따라 나누어 분석하였다.
통계적 분석
데이터 분석과 관련하여 통계 학자(통계에서 15년간의 경력을 가진 의료 통계 교수)와 상담하였다. 모든 통계 분석은 R software package (version 2.14.2; R Foundation for Statistical Computing, Vienna, Austria) 및 Stata 14.0 (StataCorp, College Station, TX, USA)을 사용하여 수행하였다.
환자들을 첫 번째와 두 번째 판독 세션에서 척추 전이 의심 병변에 대한 신뢰등급의 변화를 기반으로 14개의 군(category)으로 분류하였다. 이에 대한 설명은 Table 1에 자세히 기술하였다. 예를 들어, 1군은 probably metastasis로 평가된 분절의 수가 감소하였고, doubtful은 변화가 없으며, probably benign으로 평가된 분절의 수는 증가한 경우에 해당한다; 8군은 probably metastasis로 평가된 분절의 수가 감소하였고, doubtful은 증가하였으며, probably benign으로 평가된 분절의 수는 변화가 없는 경우에 해당한다.
이러한 14개의 군을 유용한 정도(degree of usefulness)에 따라 4개의 그룹(group)으로 통합하였다.
1) 명확히 유용한 그룹(definitely useful group), 전이의 감별에 유용한 1, 2, 3, 4, 7군과 전이의 발견에 유용한 5군, 전이의 발견과 감별 모두에 유용한 6군
2) 유용성이 모호한 그룹(equivocal group), 8, 9, 10, 11, 12군
3) 유용하지 않은 그룹(not useful group), 13군
4) 척추 전이가 없는 것으로 평가된 그룹(presumed non-metastatic group), 14군
2회의 판독 세션에서 모두 척추의 모든 분절에 대해 비교적 분명히 전이가 없을 것으로 판단되는 경우(probably benign: 0)로 판독한 경우는 14군으로 분류하였고 신뢰등급의 변화를 평가하지 않았다. 이러한 경우에 수치상으로는 13군으로 분류되지만, 확산강조영상의 유용성을 반영하기 어렵다고 판단하였기 때문이다.
환자의 임상 정보(나이, 성별, 원발 종양, 척추 전이의 유형)를 Fisher's exact test로 분석하였고, 유용성을 반영한 3개의 그룹과 첫 번째 세션에서의 probably metastasis로 평가한 분절의 수의 상관관계를 kruskal wallis test로 평가하였다.
유용성을 반영한 3개의 그룹과 해부학적 위치(척추뼈몸통, 척추뒤고리)의 상관관계를 Fisher's exact test로 분석하였다.
모든 검사에서, 통계적으로 유의한 차이를 나타내는 지표로 p-value를 사용하였고, p < 0.05를 기준으로 하였다.
결과
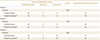
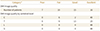
48명의 연구 대상 환자들 중 척추뼈몸통을 기준으로 하였을 때, reader 1의 판독상에서 definitely useful은 18명, equivocal은 5명, not useful은 8명이었고, presumed non-metastatic lesion은 17명이었다. Reader 2의 판독상에서는 definitely useful은 19명, equivocal은 5명, not useful은 8명이었고, presumed non-metastatic lesion은 16명이었다. Reader 3의 판독상에서는 definitely useful은 16명, equivocal은 5명, not useful은 10명이었고, presumed non-metastatic lesion은 17명이었다. Presumed non-metastatic lesion을 포함하지 않고 계산하였을 때, definitely useful 그룹은 reader 1에서 58%(18/31), reader 2에서 59%(19/32), reader 3에서 52%(16/31)였다.
48명의 연구 대상 환자들 중 척추뒤고리를 기준으로 하였을 때, reader 1의 판독상에서 definitely useful은 12명, equivocal은 1명, not useful은 5명이었고, presumed non-metastatic lesion은 30명이었다. Reader 2의 판독상에서는 definitely useful은 13명, equivocal은 1명, not useful은 9명이었고, presumed non-metastatic lesion은 25명이었다. Reader 3의 판독상에서는 definitely useful은 9명, equivocal은 4명, not useful은 10명이었고, presumed non-metastatic lesion은 25명이었다. Presumed non-metastatic lesion을 포함하지 않고 계산하였을 때, definitely useful 그룹은 reader 1에서 67%(12/18), reader 2에서 57%(13/23), reader 3에서 39%(9/23)였다.
Reader 3의 판독에 한하여, 첫 번째 세션에서 probably metastasis로 평가된 분절의 수는 척추뼈몸통과 척추뒤고리를 기준으로 하였을 때 모두 definitely useful, equivocal 그리고 not useful group 사이에 유의한 차이를 보였다[척추뼈몸통(p < 0.001), 척추뒤고리(p = 0.002)]. Reader 1의 경우, 척추뒤고리로 분석하였을 때, 유의한 차이를 보였다(p = 0.039). Reader 2에서는 모든 경우에서 유의한 차이가 없었다.
고찰
본 연구에서 확산강조 자기공명영상을 추가하였을 때 definitely useful로 평가된 경우는 척추뼈몸통 기준으로 52~59%였고, 척추뒤고리 기준으로 39~67%였다. 확산강조 자기공명영상이 척추 전이의 발견과 감별(characterization) 모두에 있어서 비교적 유용하다는 것을 보여준 결과이다. Definitely useful, equivocal, not useful 그룹 사이에서 3명의 reader에서 모두 유의한 차이를 보이는 임상적 요인 혹은 영상의학적 요인은 없었다.
우리는 척추뒤고리를 기준으로 하였을 때 척추뼈몸통을 기준으로 하였을 때보다 유용할 것으로 예상하였지만, 척추뼈몸통과 척추뒤고리를 기준으로 하였을 때, 유용한 정도에 유의한 차이가 없었다. 그러나, Fig. 4에 기술한 환자 1명은 첫 번째 판독 세션에서 세 명의 reader가 모두 T3 척추분절의 척추뒤고리에 위치한 작은 병변을 발견하지 못하였지만, 두 번째 판독 세션에서 확산 제한을 보이는 해당 병변을 발견하였다. 이 환자는 확산강조영상이 전이의 발견에 유용한 5군(useful in detection of metastasis), 그리고 명확히 유용한 그룹(definitely useful group)으로 분류되었다.
또한, Fig. 5에 기술한 환자 1명은 첫 번째 판독 세션에서 세 명의 reader가 모두 L2 척추 분절의 병변에 대해서 전이 여부가 애매한 경우(doubtful)로 판독하였으나, 두 번째 판독 세션에서 해당 병변이 확산 제한을 보이지 않아 비교적 분명히 전이가 없을 것으로 판단되는 경우 probably benign)로 판독하였다. 이 환자는 확산강조영상이 전이의 감별에 유용한 3군(useful in characterization of metastasis), 그리고 명확히 유용한 그룹(definitely useful group)으로 분류되었다.
요통은 척추 전이의 가장 흔한 증상이고 이로부터 수 주에서 수개월 후에는 신경학적 증상이 발현되는 경우가 많다(22). 척추 전이 환자에게 가장 중요한 치료 목적은 통증을 감소시키고, 기능을 회복시키는 것이다(23). 척추 전이 여부 및 전이된 분절 수의 평가는 암 환자에게서 앞서 언급한 증상이 있을 때 원인에 대한 평가에 있어 매우 중요하다(24).
ACR에 따르면, 척추 전이 여부 및 전이된 분절 수의 평가에 있어 MRI는 현재 가장 중요한 modality로 사용되고 있다(8). 병적 압박 골절의 감별에서 유용성이 확인된 DWI를 척추 전이 여부 및 전이된 분절 수의 평가에도 적용한다면, 더욱 정확한 평가가 가능할 것이다. 이는 결국, 척추 전이의 조기 발견 및 감별을 가능하게 할 것이고, 이를 토대로 한 수술적 혹은 방사선 치료 등의 척추 전이의 치료 계획 수립을 더욱 정교하게 하는 데 기여할 수 있을 것이다.
본 연구에는 몇 가지 제한점이 있다. 첫째로, 전이로 생각된 병변들이 병리학적으로 평가되지 않았고, 영상의학적으로 추적관찰하여 비교하지 않았다. 둘째, 2회의 세션 사이의 비교 시 전체 분절 수를 기준으로 신뢰등급의 변화를 평가하였기 때문에 각 분절의 신뢰등급 변화는 충분히 반영되지 않았을 가능성이 있다. 셋째, 연구 대상 환자의 수가 상대적으로 적었다. Definitely useful 그룹의 대상 환자 수는 파라 메트릭 분석(parametric analysis)에 사용 가능했지만 equivocal 과 not useful group에는 사용할 수 없었다.
14개의 군(category)으로 분류하여 분석하였을 때, 기존의 자기공명영상(conventional MRI)에 확산강조영상(DWI)을 추가한 경우가 척추 전이의 발견(detection) 및 감별(characterization)에 있어서 유용하였지만, 해부학적 위치에 따른 유용성에 차이는 없었다.






 XML Download
XML Download