

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lateral ankle sprains are among the most common musculoskeletal injuries. The reported incidence rates range from 2.2 sprained ankles per 1000 person-years in the United States (1) to 5.3–7.0 sprained ankles per 1000 person-years in Europe (2). Ankle sprains mostly involve the young, active population and are more common in individuals under 35 years of age (3). Ankle sprains are more serious than commonly believed because in addition to the immediate onset of pain, swelling, and loss of joint motion, chronic lateral ankle instability (CLAI) with recurrent sprains and residual sensations of giving way has been reported in 15–40% of all lateral ankle sprain cases. This usually causes significant problems in gait and high-level physical activities, such as jogging, jumping, and skiing, and accelerates the possible development of osteoarthritis of the talocrural joint (456).
Therefore, patients with CLAI, in whom conservative treatment failed, require surgical treatment to restore mechanical stability (457). Additionally, young patients with CLAI with active lifestyles usually want good ankle stability for sports. The anterior talofibular ligament (ATFL), the main stabilizer of the ankle joint, is the most commonly affected ligament, followed by the calcaneofibular ligament (CFL) and the posterior talofibular ligament (89). To decide on the method of surgical treatment, it is essential to detect ankle ligament tears. Furthermore, it is imperative to assess the extent of the ligament tears and the quality of the residual ligamentous tissue. If the quality of the remnants of the ruptured ligaments is acceptable, anatomic repair is recommended; however, if the injured ligaments are attenuated, anatomical reconstruction should be performed (1011). However, besides clinical examination findings, only the talar tilt angle on stress radiographs is included as an indicator for selecting patients for ligament reconstruction (LAR) surgery (12). Although stress radiography, ultrasound, and MRI show clinical features for the diagnosis of lateral ankle ligament tears, few studies have conducted a comprehensive review of the imaging methods in terms of providing information on the residual ligamentous tissue required for selecting the appropriate surgical treatment methods (101314).
The purpose of our study was to perform a qualitative analysis of the MRI findings of ATFL and CFL injuries in patients with CLAI and to compare the MRI findings between surgical treatment groups. Consequently, we assessed the performance of MRI in providing useful information for selecting surgical methods in patients with CLAI.
MATERIALS AND METHODS
PATIENTS
Our Institutional Review Board approved this retrospective study, and the requirement to obtain an informed consent was waived (IRB No. KUH1140087). By performing a computerized search of medical and radiologic records from February 2012 to December 2016, 86 patients who had undergone surgical treatment for CLAI were found. These patients had undergone either the modified Broström procedure (MBP) or anatomical lateral ankle LAR and met the following criteria: 1) symptomatic CLAI and 2) history of preoperative ankle MRI and varus stress radiography within 6 months before surgery. All patients had failed non-operative treatment with a rehabilitation program for a minimum of 3 months and had recurrent episodes of giving way or sensations of lateral ankle instability. Thirty patients who underwent MRI at other institutions using varied MRI systems and pulse parameters were excluded. In addition, three patients were excluded because their ankle sprain occurred less than 2 weeks prior to undergoing preoperative MRI. One patient in the LAR group who had undergone a previous MBP and had a postoperative infection was excluded.
Finally, 52 ankle MRI studies from 52 patients were included in our retrospective study. The mean age at preoperative MRI and clinical assessment was 29 years (range, 15–56 years). There were 25 men patients (mean age, 35 years; age range, 19–58 years) and 27 women patients (mean age, 31 years; age range, 15–56 years). They were divided into two groups according to the surgical treatment: 31 patients (13 men, 18 women; mean age, 29 years; age range, 16–56 years) underwent MBP, and 21 patients (12 men, 9 women; mean age, 35 years; age range, 19–58 years) underwent LAR. All surgical procedures were performed by the same ankle surgeon with 20 years of experience in performing ankle surgeries. The surgeon's criteria used to select which patients should undergo LAR were based on the following overall considerations: significant ankle laxity on talar tilt inversion ankle stress radiographs and clinical findings, including generalized ligamentous laxity, high-demand heavy athletes, or previous failed MBP. MBP, which is the most widely used technique, involves direct repair and augmentation of the ATFL (15); conversely, LAR involves direct repair of the ATFL and anatomical reconstruction of the ATFL and CFL using a free semitendinosus tendon allograft and interference screws (16). All patients enrolled in this study showed good clinical results after the surgical treatments based on various clinical outcome score improvements, including the American Orthopedic Foot and Ankle Society ankle-hindfoot function scoring system, Karlsson-Peterson ankle score, and visual analogue scale pain score (1718).
MRI PROTOCOL
The patients underwent MRI using a 3.0-Tesla system apparatus (Magnetom Skyra, Siemens Healthcare, Erlangen, Germany) with a 16-channel ankle coil (Siemens Healthcare). All feet were placed in a neutral position during scanning. The following MRI sequences were employed: sagittal T2-weighted turbo-spin echo (TSE) sequence with fat saturation [repetition time/echo time (TR/TE), 3870/51; slice thickness, 3 mm; 0-mm spacing; matrix, 512 × 282; number of excitation, 1; echo train length (ETL), 9; field-of-view (FOV), 14 × 14 cm], axial T2-weighted TSE sequence (TR/TE, 4640/76; slice thickness, 3 mm; 0-mm spacing; matrix, 512 × 229; ETL, 10; FOV, 11 × 14 cm), and coronal T2-weighted TSE sequence (TR/TE, 5070/76; slice thickness, 3 mm; 0-mm spacing; matrix, 512 × 211; ETL, 11; FOV, 9 × 14 cm).
Preoperative and postoperative talar tilt inversion ankle stress radiographs were obtained in the neutral position at 150 N of stress force using a stress device (Telos SE 2000, ARD Medizinprodukte GmbH, Marburg, Germany). The talar tilt was measured up to 0.1° using a picture archiving and communication system workstation (Centricity RA 1000, GE Healthcare, Mt Prospect, IL, USA).
IMAGE ANALYSIS
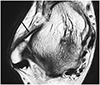
All MRIs were analyzed on the basis of the consensus of two musculoskeletal radiologists (N.R.K. and H.J., with 11 years and 1 year of experience in musculoskeletal radiology). These radiologists were blinded to the results of the physical examination and to the treatment groups of the patients. Qualitative analysis of the ATFL and CFL injuries, including caliber change, slope, and signal intensity on the T2-weighted MRIs, was performed. The caliber change in the ligaments was graded as thickened, thinned, and scarce. A thickened ligament was defined as a ligament with more than 2-mm thickness on axial T2-weighted images; a thinned ligament was defined as that with less than 2-mm thickness; and a scarce ligament was defined as that in which the remnant ligament fibers were ragged and nearly non-demonstrable (19). It was then determined whether the slope of the ligament showed normal tightness without laxity or wavy contour on the axial T2-weighted images. The signal intensity of the ligament was also analyzed. If the signal intensity of the ligament was the same as that of the tendon, it was described as a very low signal intensity; if the signal intensity was between that of the tendon and muscle, it was described as a low signal intensity; if the signal intensity was similar to that of the muscle, it was described as an intermediate signal intensity; and if the signal intensity was higher than that of the muscle, it was described as a high signal intensity (Fig. 1).
The thickness of the ligament was measured on the axial T2-weighted images. The reader magnified the image before measurement for optimal visualization of the ligament. The ATFL was measured at its middle portion between the origin and insertion, and the CFL was measured at its distal 1 cm, where its medial border could still be separated from the calcaneus (20). The talar tilt angle of all the patients was measured on the talar tilt inversion stress radiographs of the ankles preoperatively. The talar tilt angle refers to the angle between two lines drawn parallel to the tibial plafond and the talar dome.
STATISTICAL ANALYSIS
The Pearson's chi-square test was used to compare the categorical variables, including the caliber change and the signal intensity of the ATFL and CFL, between the two surgical treatment groups. The thickness of the ATFL and CFL and the talar tilt angle on the ankle inversion stress radiographs were also analyzed using the Mann Whitney U-test. The differences in the slope of the ATFL and CFL between the two groups were analyzed using the Fisher's exact test. Correlation between each thickness of the ATFL and CFL and the talar tilt angle in both surgical treatment groups was evaluated using Spearman's correlation coefficient. p < 0.05 was considered significant. Statistical analysis was performed using the SPSS software (SPSS for Windows, version 21.0; IBM Corp., Armonk, NY, USA).
RESULTS
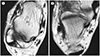
The comparison of the MRI features of the injured ATFL between the two surgical treatment groups is shown in Table 1. The injured ATFL on the T2-weighted MRIs showed a scarce or thin caliber change and was more common in the LAR group (18/21, 86%) than in the MBP group (16/31, 51%) (p = 0.002). The LAR group (17/21, 81%) also showed a decreased slope and a wavy appearance compared with the MBP group (10/31, 32%) (p = 0.001) (Figs. 2, 3). The ATFL often revealed a ragged appearance with a scanty amount of remnant ligament fibers due to chronic tear and ligament resorption in the LAR group (6/21, 29%) (Fig. 4). No significant difference was observed in the signal intensities of the injured ATFLs on the T2-weighted images between the groups (p = 0.154). A low signal intensity was commonly seen in both groups (20/31, 65% in the MBP group; 15/21, 71% in the LAR group). The mean thickness of the ATFL measured on the axial T2-weighted MRIs was significantly thinner in the LAR group (1.1 ± 0.9 mm) than in the MBP group (2.2 ± 1.3 mm) (p = 0.002).
The comparison of the MRI features of the injured CFL between the two surgical treatment groups is shown in Table 2. The CFL on the T2-weighted MRIs showed a thin caliber change and was more common in the LAR group (16/21, 76%) than in the MBP group (12/31, 39%) (p = 0.008). The LAR group also showed a decreased slope and a wavy appearance (11/21, 52%) compared with the MBP group (7/31, 23%) (p = 0.039). The mean thickness of the CFL measured on the axial T2-weighted MRIs was also significantly thinner in the LAR group (1.3 ± 0.8 mm) than in the MBP group (2.1 ± 0.9 mm) (p = 0.002).
The mean talar tilt angle on the ankle inversion stress radiographs was greater in the LAR group (13.4 ± 3.9°) than in the MBP group (9.5 ± 3.8°) (p = 0.001). Additionally, a significant correlation was observed between the talar tilt angle and the ATFL thickness in both groups, and a moderate negative correlation was present (r = -0.439, p = 0.001). However, no significant correlation was found between the talar tilt angle and CFL thickness (r = -0.142, p = 0.315).
DISCUSSION
Various surgical options for the treatment of CLAI exist. Broström described the first anatomical repair of the ATFL in 1966 (21). Several authors have modified the procedure since then. The MBP, proposed by Gould et al. (15), has become the gold standard for the primary surgical treatment of CLAI. The procedure involves augmenting the Broström repair by mobilizing the lateral portion of the inferior extensor retinaculum and attaching it to the fibula. However, certain factors have been reported to correlate with poor surgical outcomes after MBP, including previous failed ankle stabilization surgery, long-standing instability with poor ligamentous tissues, large athletes, and generalized ligamentous laxity (22). Therefore, the anatomical reconstruction of the ATFL and CFL using graft augmentation has recently gained popularity in treating these high-risk patients. Several studies have reported good-to-excellent outcomes after allograft reconstruction for CLAI in the last decade (11, 12, 16, 23).
The criteria for LAR in patients with CLAI include findings from several clinical examinations and imaging evaluations using stress radiographs (12). The indication based on stress radiographs is as follows: significant ankle laxity with more than a 10-degree difference in the talar tilt angle when compared to the opposite side or more than 15 degrees of an absolute talar tilt angle. However, the value of stress radiographs is controversial. The reliability of the stress test is determined by the extent of patient relaxation and cooperation, examiner, amount of force used, angle of ankle flexion, and amount of laxity in the uninvolved ankle (242526). The accuracy of the test increases with the use of local or general anesthesia in the operating room; however, this method could be significantly invasive for patients. Takao et al. (23) showed that patients with CLAI had morphologic ligamentous abnormalities on arthroscopic assessment despite having no demonstrable abnormal lateral laxity on stress radiographs. Nevertheless, several studies have reported that the grade of ATFL injury on MRI correlates well with the talar tilt angle (1427). In the present study, the mean talar tilt angle was greater in the LAR group than in the MBP group. Additionally, a significant correlation was found between the talar tilt angle and the ATFL thickness in both groups with a moderate negative correlation. Thus, talar tilt angle measurement and ankle MRI could be complementary methods for the preoperative assessment of patients with CLAI, although the talar tilt angle did not present a strong correlation with the quality of the ATFL remnants.
MRI is commonly used as a less invasive technique for diagnosing lateral ankle ligament injury. However, the accuracy of MRI in detecting chronic injuries of the lateral collateral ligaments has not yet been clearly established. The conventional MRI has demonstrated an accuracy of 59% in diagnosing chronic lateral ligament tears (28). Contrarily, MRI yielded a 93% accuracy in the diagnoses of 15 cases of chronic ATFL injury in the study by Oae et al. (29) and Park et al. (30) reported the accuracy of MRI for diagnosing ATFL injuries as follows: 77% for partial tears and 85% for complete tears. The discrepancy between the results of these studies may be because of the varying diagnostic criteria used for the diagnosis of chronic ankle ligament injury on MRI. Therefore, using MRI findings, such as thickening, thinning, elongation, and wavy or irregular contours of the injured ligament, in daily radiologic reports of ankle MRI would be more helpful than focusing on the discontinuity in the ligaments, as the quality of the residual ligamentous tissue is important for selecting the surgical treatment method (31). In the present study, the injured ATFLs in the LAR group showed ragged, scarce, or thin caliber changes with wavy appearances more frequently; conversely, the ATFLs in the MBP group showed thick caliber changes with maintained ligament slopes. Additionally, the CFL in the LAR group showed thin caliber changes and wavy appearances more frequently than that in the MBP group. The usual MRI signal intensity of the injured ATFL and CFL on the T2-weighted images in both groups was low, but which is higher than that of the tendon and lower than that of the muscle. This may be because the patients in the present study did not have acute injuries but chronic instability, as repetitive injury resulted in the partial restoration of the signal intensity of the ligaments while showing a higher signal intensity than the normal tendon. In the MBP group, the ATFL often revealed thickening with loss of elasticity during the intraoperative assessment.
Our study has some limitations. First, the detailed grading of the injured ATFL was not correlated with the surgical findings, as this study had a retrospective nature, although the ATFL injury itself was identified during surgery. Second, the CFL injury in the MBP group was not confirmed because the CFL could not be investigated using procedures, such as the MBP. Third, the present results may be biased because the study groups were divided according to the surgical methods.
In conclusion, qualitative analysis of lateral ankle ligament injuries using MRI for preoperative evaluation could provide information on the quality of the ligament remnants with chronic tear well; further, the findings may be included as imaging indications for selecting LAR surgery besides the talar tilt angle.




 XML Download
XML Download