

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
While not uncommon, intraabdominal infections (IAIs) can have potentially serious complications and poor outcomes, particularly if inappropriately managed.1234 IAIs are complex disease entities with a wide spectrum of pathological conditions ranging from uncomplicated appendicitis to generalized peritonitis. IAIs are caused by a diversity of microbes, most commonly enteric organisms.567 Appropriate antibiotic therapy and timely source control are essential to improve prognosis and minimize collateral damage caused by antimicrobial-resistant bacteria.8910
Recent epidemiologic studies have shown increasing interest in issues related to antimicrobial resistance in patients with IAIs.101112131415 Multidrug-resistant microorganisms are widespread worldwide, with significant geographical variations in pathogen diversity.121314 Extended-spectrum ß-lactamase (ESBL)-producing Enterobacteriaceae are problematic for both community-acquired and nosocomial infections. Hospitalized patients are often at a risk for IAIs caused by carbapenem-resistant Enterobacteriaceae and carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter species along with vancomycin-resistant enterococci (VRE).215 These problems of antimicrobial resistance complicate the decision-making process when choosing appropriate antibiotic therapy.816
The selection of empirical antibiotics based on accurate knowledge of potentially causative microorganisms increases the probability of making the right choice. Data on the distribution and antimicrobial susceptibility of pathogens isolated from patients with IAIs are of particular value for the implementation of an evidence-based antimicrobial stewardship program. However, no multicenter survey has determined the distribution and antimicrobial susceptibility of IAI-causative pathogens in Korea. Therefore, the current study investigated the microbiological profile and prevalence of antimicrobial-resistant organisms isolated from patients with IAIs in Korea, with a particular focus on Enterobacteriaceae resistant to third-generation cephalosporins, fluoroquinolones, and carbapenems, as well as non-fermentative gram-negative bacilli resistant to carbapenems, during the last 3 years to guide IAI antimicrobial therapy.
METHODS
Study design and patients
This multicenter, non-interventional cohort study was conducted at 6 university-affiliated hospitals located in 4 cities (Seoul, Guri, Busan, and Daegu) in Korea from January 2016 to December 2018. The primary aim of the study was to investigate the epidemiology and antibiotic susceptibility of microorganisms isolated from clinical specimens obtained from patients with IAIs.
Our study was based on a retrospective chart review of microorganisms isolated from consecutive adult patients (aged ≥ 18 years) with a clinical diagnosis of IAI in whom the causative pathogens had been elusive. First, data on all microorganisms isolated from patients in each participating hospital during the study period were listed. Then, the IAI-causative microorganisms were screened by the investigator in each participating hospital. IAI-causative microorganisms were defined as pathogens identified from intraabdominal fluid or tissue samples obtained from an aseptically placed drain in the intraabdominal space, such as closed suction drainage system, open drain, T-tube drain, computed tomography-guided drainage, or during invasive procedures for diagnosis or treatment.17 Specific microorganisms involved in spontaneous bacterial peritonitis or continuous ambulatory peritoneal dialysis peritonitis were excluded from our analysis. Isolates obtained from abdominal drains or drainage bottles, superficial wounds, blood, or perianal abscess were also excluded from our analysis. The organisms were considered clinically significant at the discretion of the investigators. Microbiological and clinical data for each isolate were recorded on a case report form based on the patients' medical records.
A single patient could harbor more than one microorganism during the study period. All microorganisms isolated from a patient were separately included in the analysis. In cases of multiple isolates of the same microorganism from a patient during the study period, only the first was included in the analysis.
Data collection and definitions
IAIs were clinically diagnosed in patients who presented with rapid-onset abdominal pain and signs of local and systemic inflammation (pain, tenderness, fever, tachycardia, and tachypnea).18 The diagnosis of postoperative IAIs was made based on the definitions stated in the guidelines from the National Nosocomial Infections Surveillance system.19 Electronic medical records were also reviewed to collect relevant demographic and clinical information such as demographic characteristics, IAI type (complicated or non-complicated), IAI extent, infection origin, and microbiological data.
Nosocomial IAIs were defined as infections that were absent on hospitalization but that occurred after 48 hours of admission in patients hospitalized for a reason other than IAI. The remaining IAIs were classified as community-onset IAIs. Uncomplicated IAIs were defined as infections contained within a single organ of origin, whereas complicated IAIs were defined as infections that extended beyond the source organ and into the peritoneal cavity through the anatomic disruption. Postoperative IAIs were considered nosocomial infections. The remaining IAIs were categorized as community-onset IAIs.20
Microbiological evaluation
Species identification and drug susceptibility testing of the isolates were performed in each participating hospital using VITEK II (BioMèrieux, Hazelwood, MO, USA) or MicroScan WalkAway 96 plus (Siemens Healthcare Diagnostics Inc., CA, USA) systems based on the standard criteria defined by the Clinical and Laboratory Standards Institute (CLSI).21 Escherichia coli and Klebsiella spp. were screened for an ESBL phenotype (ceftazidime or cefotaxime minimum inhibitory concentration >1 μg/mL) and confirmed as ESBL producers using combination clavulanate-based testing according to the method from the CLSI.22
Statistical analysis
Data are presented as frequencies (proportion) or means ± standard deviation, as appropriate. Categorical variables were compared using χ2 or Fisher's exact tests. IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Statistical significance was defined as P < 0.05.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Korea University Anam Hospital (IRB registration No. 2019AN0128). The investigators requested formal approval of the protocol by the regional ethics committee, if required. Because this research was a retrospective chart review study, informed consent was waived.
RESULTS
Patients and characteristics of IAIs
During the study period, 2,114 isolates from 1,571 patients (60.4% men, 67.0 ± 15.7 years) with microbiologically proven IAI were identified. Among 1,571 patients, community-onset IAIs and nosocomial IAIs were identified in 1,207 (76.8%) and 364 (23.2%) patients, respectively. Uncomplicated and complicated IAIs were observed in 966 (61.5%) and 605 (38.5%) patients, respectively. The most common primary focus of IAIs was the biliary tract, including the gallbladder (51.2%), followed by the liver (13.7%), colon or rectum (13.0%), gastroduodenum (6.3%), and appendix (4.9%). The distribution of lesion extent included localized inflammation (27.2%), localized abscess (47.5%), localized peritonitis (7.4%), diffuse suppurative peritonitis (12.2%), and combined complicated infection (5.7%). Among 2,114 isolates, 1,604 (75.9%) were collected from community-onset IAIs and 510 (24.1%) were collected from nosocomial IAIs. Among these isolates, 848 (40.1%) and 1,266 (59.9%) were associated with complicated and non-complicated IAIs, respectively. The lesion extent and sources of specimens in community-onset and nosocomial infections are summarized in Table 1. Diffuse suppurative peritonitis was more common in nosocomial IAIs than in community-onset IAIs. More than half of the IAI specimens were collected from biliary tracts, including the gallbladder (Table 1).
Table 1
Characteristics of IAIs according to community-acquired and nosocomial infections
Data are presented as number (%).
IAIs = intraabdominal infections.
aBiliary tract infections such as acute cholecystitis and acute cholangitis.
![]()
Distribution of the major pathogens isolated from IAIs
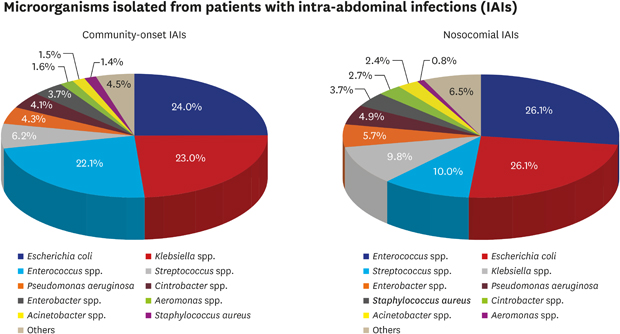
The distribution of the microorganisms was aerobic gram-negative (62.6%), aerobic gram-positive (33.7%), anaerobic (0.9%), and fungal (2.8%) pathogens. The most commonly identified pathogens were E. coli (23.8%), followed by Enterococcus spp. (23.1%), Klebsiella spp. (19.8%), and Streptococcus spp. other than S. pneumoniae (7.1%).
The distribution of microorganisms differed between community-onset and nosocomial IAIs (Table 2). Nosocomial IAIs had higher proportions of aerobic gram-positive bacteria (P < 0.001) and lower proportions of aerobic gram-negative bacteria (P < 0.001) than those in community-onset IAIs. There were significant differences in the isolation frequencies of Klebsiella spp. (P < 0.001) and Streptococcus spp. other than S. pneumoniae (P = 0.006) between the 2 groups, unlike E. coli (P = 0.689) and Enterococcus spp. (P = 0.065). The most commonly identified pathogens of nosocomial IAIs were Enterococcus spp. (26.1%), followed by E. coli (23.1%), Streptococcus spp. (10.0%), and Klebsiella spp. (9.8%), while those of community-onset IAIs were E. coli (24.0%), followed by Klebsiella spp. (23.0%), Enterococcus spp. (22.1%), and Streptococcus spp. (6.2%) (Table 2).
Table 2
Distributions of the most common microorganisms isolated from patients with IAIs

![]()
The most common causative isolates differed according to the IAI origin (Table 3). Gram-positive bacteria were the most common pathogens in IAIs of the upper gastrointestinal tract compared with gram-negative bacteria in the lower gastrointestinal tract. Klebsiella pneumoniae and Enterococcus spp. were the most commonly isolated pathogens in patients with IAIs of the liver and pancreaticobiliary tract, respectively.
Table 3
The 3 most common pathogens isolated from patients with intraabdominal infections segregated by infection sources

![]()
Antimicrobial susceptibilities of major pathogens isolated from IAIs
The antimicrobial susceptibility profiles of the most common gram-negative bacteria are detailed in Table 4. The most active antibiotics against Enterobacterales were amikacin (susceptibility rates ranging from 97.4% to 100%), ertapenem (92.2% to 99.5%), imipenem (94.3% to 99.8%), and tigecycline (94.9% to 99.0%). The susceptibility rate to ciprofloxacin was as low as 56.4% in E. coli but was 86.3% in K. pneumonia, 94.3% in Enterobacter spp., and 82.3% in Citrobacter spp. The susceptibility rates of ß-lactam/ß-lactamase inhibitors to piperacillin/tazobactam and amoxicillin/clavulanate were 99.0% and 62.5%, respectively, in E. coli and 84.8% and 83.0%, respectively, in Klebsiella spp. With respect to cephalosporins, the susceptibility rates to cefoxitin, cefotaxime, ceftazidime, and cefepime were 82.7%, 61.4%, 63.7%, and 65.3%, respectively, in E. coli and 88.1%, 80.7%, 83.1%, and 84.3%, respectively, in Klebsiella spp. In P. aeruginosa, the susceptibility rates to amikacin, ciprofloxacin, imipenem, and ceftazidime were 94.5%, 83.5%, 77.4%, and 73.3%, respectively, while the rates to piperacillin/tazobactam was as low as 58.0%. In Acinetobacter spp., the susceptibility rates to amikacin, ampicillin/sulbactam, piperacillin/tazobactam, and imipenem were less than 50% (Table 4).
Table 4
Antimicrobial susceptibilities of aerobic gram-negative bacteria according to CO and N infections
The data are presented as number of susceptible/total number (%).
AMP/SM = ampicillin/sulbactam, AMX/CA = amoxicillin/clavulanate, AMK = amikacin, CAZ = ceftazidime, CFO = ceftriaxone, CFX = cefoxitin, CIP = ciprofloxacin, CO = community-onset, CTX = cefotaxime, EPM = ertapenem, FEP = cefepime, GEN = gentamicin, IPM = imipenem, N = nosocomial, TIG = tigecycline, TZP = piperacillin/tazobactam.
![]()
Table 4 shows the susceptibility rates to major antimicrobial agents against community-onset and nosocomial isolates of the gram-negative bacteria most frequently recovered from IAIs. Overall, the susceptibility rates to most antibiotics were higher in microorganisms isolated from community-onset IAIs than in those isolated from nosocomial IAIs. In E. coli and Klebsiella spp., the susceptibility rates to cefotaxime, cefepime, ciprofloxacin, and piperacillin/tazobactam differed by more than 10% between the 2 groups, whereas the rates to amikacin and imipenem did not (Table 4). The tigecycline susceptibility rate for Klebsiella spp. isolated from nosocomial IAIs was 10.1% lower than that for isolates from community-onset IAIs. However, the E. coli susceptibility rates to tigecycline were similar between the 2 groups (Table 4).
On comparison between ESBL-producer and non-ESBL-producer E. coli and Klebsiella spp., the susceptibility rates to imipenem, amikacin, and tigecycline were above 90% in both groups. The susceptibility rates to cefoxitin and piperacillin/tazobactam in ESBL-producing E. coli were 73.2% and 77.4%, respectively, whereas those in ESBL-producing Klebsiella spp. were 66.2% and 41.3%, respectively (Table 5).
Table 5
Antimicrobial susceptibilities of ESBL-producing and non-ESBL-producing Escherichia coli and Klebsiella pneumoniae
The data are presented as number of susceptible/total number (%).
ESBL = extended-spectrum ß-lactamase; AMX/CA = amoxicillin/clavulanate, AMK = amikacin, CAZ = ceftazidime, CFX = cefoxitin, CIP = ciprofloxacin, FEP = cefepime, IPM = imipenem, GEN = gentamicin, IPM = imipenem, TIG = tigecycline, TZP = piperacillin/tazobactam.
![]()
The antimicrobial susceptibility profiles of the most common gram-positive bacteria are described in Table 6. Considering the susceptibility rates of gram-positive bacteria to major antibiotics, vancomycin, tigecycline, and linezolid were most consistently active in vitro in both community-onset and nosocomial infections (Table 6). However, even in community-onset IAIs, the susceptibility rates to ampicillin/sulbactam and ciprofloxacin in Enterococcus spp. and those to clindamycin and ciprofloxacin in Staphylococcus aureus were less than 70% (Table 6). The prevalence of methicillin-resistant S. aureus and VRE was 21.8% and 59.5%, respectively.
Table 6
Antimicrobial susceptibilities of aerobic gram-positive bacteria according to CO or N infection status

The data are presented as the number susceptible/total number (%).
CO = community-onset, N = nosocomial, AMP = ampicillin, AMP/SM = ampicillin/sulbactam, CFO = ceftriaxone, CIP = ciprofloxacin, CLI = clindamycin, IMP = imipenem, LVX = levofloxacin, LZD = linezolid, OXA = oxacillin, TIG = tigecycline, VAN = vancomycin.
![]()
DISCUSSION
To our knowledge, this is the first multicenter study on IAIs in Korea to describe the microbiological distribution and antimicrobial susceptibility patterns of pathogens isolated from patients with IAIs. In this descriptive study, Enterococcus spp. was the second most common isolate in patients with IAIs, accounting for 23.1% of isolates. These enteric microorganisms frequently show multidrug resistance to various antibiotics recommended as empirical antibiotics.
In the present study, the 3 most common pathogens in community-onset IAIs were E. coli (24.0%), Klebsiella spp. (23.0%), and Enterococcus spp. (22.1%), whereas those in nosocomial IAIs were Enterococcus spp. (26.1%), E. coli (23.1%), and Streptococcus spp. (10.0%). Previous studies mainly focused on gram-negative bacteria have reported Enterobacteriaceae to be the major pathogens involved in complicated IAIs.122324 In contrast, our study included both uncomplicated and complicated IAIs to report the microbiological distribution of IAIs, observing a relatively high composition ratio of gram-positive pathogens, particularly Enterococcus spp. The heterogeneity of study populations with various IAI origins can also affect the microbiologic profile of pathogens associated with IAIs (Table 3).25 Although clinicians in real-world settings commonly encounter Enterococcus isolates while treating IAIs, the necessity of empirical and directed antimicrobial agents against Enterococcus spp. continues to be debated.262728 Some studies have suggested that the isolation of Enterococcus in patients with IAIs results in treatment failure or increased mortality,293031 while others demonstrated no association with mortality.3233 Furthermore, some studies have shown equivalent therapeutic effects among empiric antibiotic regimens, regardless of the antimicrobial activity against enterococci.34353637 At present, prominent guidelines recommend empirical anti-enterococcal therapy for patients with nosocomial IAIs and severe community-acquired IAIs.1028
Our findings reveal a much smaller proportion of anaerobes than previously reported (0.9% vs. 7.7%–22.9%),121638 although one study reported a similar proportion.23 Several guidelines on the management of complicated IAIs have indicated the role of intraabdominal culture and susceptibility testing. However, they did not provide detailed culture methods to identify anaerobic bacteria.81018 Considering the increasing prevalence of antibiotic resistance in anaerobes, regional susceptibility patterns are crucial for the empirical treatment of anaerobic infections.394041
The guidelines from the World Society of Emergency Surgery suggest amoxicillin/clavulanate and cefotaxime or ciprofloxacin in combination with metronidazole as appropriate regimens for mild-to-moderate community-acquired IAIs.9 Moreover, cefepime in combination with metronidazole has been recommended for high-risk community-acquired IAIs.9 In the present study, however, we observed poor susceptibility rates of < 70% to amoxicillin/clavulanate (62.5%), cefotaxime (61.4%), ceftazidime (63.7%), cefepime (65.3%), and ciprofloxacin (56.4%) among E. coli isolates and good susceptibility rates of ≥ 80% to cefoxitin (82.7%), piperacillin/tazobactam (99.0%), ertapenem (99.5%), imipenem (99.8%), meropenem (99.2%), amikacin (97.4%), and tigecycline (99.0%) in both community-onset IAIs and nosocomial IAIs. In both nosocomial and community-onset IAIs, increased Enterobacteriaceae resistance to cefotaxime along with high resistance rates to cefepime undermine the rationale for the use of extended-spectrum cephalosporins as empirical therapy for IAIs in Korea. However, carbapenem monotherapy and amikacin-based combination therapy are expected to have broad-spectrum activity against bacterial pathogens of IAIs, and thus, the clinical value of cefoxitin mentioned in the guidelines for the diagnosis and management of complicated IAIs by the Infectious Diseases Society of America should be evaluated clinically.10 In addition, active bacterial culture and susceptibility testing may be useful in guiding pathogen-directed therapy to ensure appropriate antibiotic therapy and minimize excessive exposure to broad-spectrum antibiotics with step-down therapy. Among Klebsiella spp. isolated from community-onset IAIs, good susceptibility rates of ≥ 80% to all antibiotics tested were observed (Table 4). In contrast, among isolates from nosocomial IAIs, the susceptibility rates to amoxicillin/clavulanate, cefepime, ciprofloxacin, and piperacillin/tazobactam were < 70%, whereas those to amikacin, imipenem, ertapenem, and tigecycline were ≥ 80%.
The main resistance problems are currently represented by ESBL-producing Enterobacteriaceae, CRE, and carbapenem-resistant non-fermentative bacteria. In our study, ESBL-producing strains accounted for 39.8% of E. coli spp. and 17.7% of Klebsiella spp. Data from the Study for Monitoring Antimicrobial Resistance Trends from 2005 to 2010 also showed that the Asia–Pacific region consistently had the highest ESBL positivity rates of 23%–38% for E. coli and K. pneumoniae, respectively, in IAI isolates.42 The susceptibility rates of the P. aeruginosa and Acinetobacter spp. isolates to imipenem were 77.4% and 36.7%, respectively, which were similar to those mentioned in previous reports.124344 As the susceptibilities of P. aeruginosa and Acinetobacter spp. isolates to imipenem were less than 80% in nosocomial IAIs, antimicrobial coverage of the potential pathogens of nosocomial IAIs may become more convoluted.10
To reduce carbapenem resistance, carbapenem-sparing therapy has been proposed for infections caused by ESBL-producing Enterobacteriaceae.45 In our findings, the high susceptibility rates of ESBL-producing E. coli to piperacillin/tazobactam (77.4%), cefoxitin (73.2%), amikacin (93.9%), and tigecycline (99.0%) (Table 5) suggest that these antibiotics may be acceptable alternatives to imipenem (99.5%). However, the low susceptibility rates of ESBL-producing Klebsiella spp. to piperacillin/tazobactam (41.3%) and cefoxitin (66.2%) and reduced activity against ESBL-producing E. coli with a high inoculum of bacteria may impede the general use of piperacillin/tazobactam and cefoxitin against ESBL producers.4647
Ciprofloxacin and amoxicillin/clavulanate, previously recommended for mild-to-moderate community-acquired IAIs, were active against less than 60% of E. coli isolates in vitro, as shown in previous studies.1213 Therefore, their roles as empirical antibiotics even for community-acquired IAIs are limited. However, their role as directed antibiotics should be guaranteed to control the emergence of antimicrobial resistance.
Our study has several limitations. First, the limitations pertain mostly to the study's retrospective design. In particular, data on the community-onset versus nosocomial nature of the infections were determined retrospectively using the length of stay as a surrogate marker. Second, because centralized microbiological analysis of the strains in a reference laboratory was not available, complete susceptibility data could not be elucidated. However, all microbiological laboratories are periodically accredited under the Korean Laboratory Accreditation Program developed by the Korean Society of Laboratory Medicine. Third, the IAI-causative pathogens in this study were initially selected based on objective criteria. However, the clinical significance of the microorganisms was determined by researchers at each participating institution.
In conclusion, the results of this study demonstrate the prevalent antimicrobial resistance patterns among pathogens isolated from patients with IAIs in Korea, which are inconsistent with the international guidelines for IAIs. The establishment of local guidelines for IAIs is required according to more basic data reflecting the national situation.
 XML Download
XML Download