

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Left-sided gallbladder (LSGB) is a rare anomaly in which the gallbladder is located on the left side of the round ligament without situs inversus viscerum [12]. LSGB was first described by Hochstetter in 1856 [3]. The reported incidence of this anomaly is 0.1%–1.2% [2345].
In LSGB, cystic duct and cystic artery anomalies are observed due to gallbladder location. The cystic duct is anastomosed to the left or right side of the common bile duct (CBD) or, rarely, anastomosed to the hepatic duct [2]. The cystic artery is usually long, originates on the right side of the CBD, and courses to the left in front of the bile duct to the gallbladder [2].
LSGB is reportedly associated with right-sided round ligaments accompanied by abnormal intrahepatic portal venous branching, segment IV atrophy, congenital liver cysts, complete or partial situs inversus, a duplicate gallbladder, hypoplastic bile duct, and an anomalous pancreatobiliary ductal junction [236789]. In addition, anomalies such as the main bile duct lying in front of the first part of the duodenum and malrotation of the intestine, an anteduodenal portal vein, an annular pancreas, agenesis of the dorsal pancreas, polysplenia, and highly mobile right colon are associated with LSGB [1011].
Most cases of LSGB are diagnosed intraoperatively despite repeated radiological interventions [1]. The recognition of LSGB is important during cholecystectomy to avoid injury to the biliary tree [1]. When patients with LSGB undergo laparoscopic cholecystectomy, several modifications of the laparoscopic procedure may be effective, such as that the right-hand surgical ports should be placed to the left of the midline or preparation and clipping of the cystic duct should be performed as closely as possible to the infundibulum after the surrounding tissue is stripped down [212].
The aims of this case series study were to review the 10 patients who were diagnosed with LSGB and analyze their anatomic variations of the bile duct, portal vein, and hepatic vessels.
METHODS
Patients and preoperative evaluation
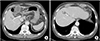
We retrospectively analyzed the clinical data of 10 patients who were diagnosed with LSGB in Gachon University Gil Medical Center and Kangdong Sacred Heart Hospital between April 2004 and May 2019. Eight patients were diagnosed with LSGB at the time of laparoscopic cholecystectomy. Two patients were diagnosed with LSGB by incidental findings on abdominal CT (Fig. 1). In the patients diagnosed with LSGB, the intrahepatic vascular and biliary systems, especially portal venous branching, were evaluated based on the ultrasound (US) imaging, abdominal CT, and/or magnetic resonance cholangiopancreatography (MRCP) findings (Fig. 2). One patient underwent endoscopic retrograde cholangiopancreatography for a CBD stone before the laparoscopic cholecystectomy. The right and left liver volumes were calculated respectively using PACS (pitcture archiving and communication system) software (INFINITT Healthcare, Seoul, Korea), excluding the volumes of vessels in preoperative abdominal CT scan. The study was approved by the Institutional Review Board at Gachon University Gil Medical Center (IRB No. 2019-259) and Kangdong Sacred Heart Hospital (IRB No. 2019-08-003). The informed consent was waived by the Institutional Review Board in both centers.
Laparoscopic cholecystectomy for the LSGB patient
Ten patients underwent laparoscopic cholecystectomy. When we performed conventional laparoscopic cholecystectomy, the second (for the left hand) and third (for the right hand; main working port) laparoscopic ports were inserted in the right upper quadrant area and epigastric area of the abdomen, respectively (Fig. 3A). In laparoscopic cholecystectomy for LSGB patients who diagnosed before the surgery, the second and third laparoscopic ports were inserted in the right upper and left upper quadrants of the abdomen, respectively (Fig. 3B). In laparoscopic cholecystectomy for LSGB patients who diagnosed during the surgery, the position of the third port can be determined after confirmation of the gallbladder's position through the second port (Fig. 4). Because of getting the proper angle for the right hand, the third port must be located in the left side of round ligament of LSGB patient. When the operators could not get the critical view of safety during laparoscopic cholecystectomy for LSGB, we did top-down technique that removes the gallbladder from liver bed firstly.
RESULTS
Patient characteristics and perioperative outcomes
The patients' characteristics and perioperative outcomes are listed in Table 1. There were 7 women and 3 men; the median patient age (range) was 56.5 years (52–71 years), and the median body mass index (range) was 22.5 kg/m2 (20.4–30.5 kg/m2). Ten patients underwent laparoscopic cholecystectomy for acute cholecystitis or symptomatic gallbladder stone. The median operation time (range) of laparoscopic cholecystectomy was 50 minutes (35–160 minutes). In 2 patients, operation time was relatively long due to severe gallbladder inflammation. Three ports were used in all laparoscopic cholecystectomy procedures. Seven patients underwent laparoscopic cholecystectomy with top-down technique. Median postoperative hospital stay (range) was 3 days (3–5 days); there were no cases of surgery-related morbidity. There were no cases of intraoperative cholangiography (IOC) procedure to prevent bile duct injury.
Bile duct variation
Five of 10 patients were evaluated with MRCP preoperatively for bile duct anatomy; of them, one also underwent ERCP due to CBD stones (Table 2). Two patients had a type 1 bile duct, in which a common hepatic duct (CHD) is formed by fusion of the right hepatic duct (RHD) and left hepatic duct (LHD) [13]. The RHD arises through fusion of the right anterior segmental duct, which drains anterior segments V and VIII, and the right posterior segmental duct (RPSD), which drains posterior segments VI and VII. Three patients had type 3 bile duct (2 with type 3B, 1 with type 3A) [13]. Type 3 bile duct, representing anomalous drainage of the RPSD, is subdivided into types 3A, 3B, and 3C according to the drainage pattern: type 3A drains into the LHD; type 3B into the CHD; and type 3C into the cystic duct (Fig. 2).
Portal vein variation
The portal vein anatomy of 10 patients was evaluated preoperatively using abdominal CT (Table 2). Right posterior portal vein as the first branch of the main portal vein (type 3) was observed in all patients with LSGB (Fig. 5A) [14]. Segment IV branches of left portal vein crossing over to segment VIII territory were observed in 7 of the 10 patients with LSGB (Fig. 5B).
Hepatic vessels variation
An accessory left hepatic artery originating from the left gastric artery was observed in 2 of 10 patients, while normal hepatic artery anatomy was observed in rest (Table 2). Hepatic vein variation was evaluated preoperatively using abdominal CT and classified into 4 types according to superior right hepatic vein morphology [15]. Five of 10 patients were categorized into type 2, in which a proximal confluence was formed by 2 tributaries running along the intersegmental border and draining nearby segments (V/VI or VI/VII) and a substantial tributary from segment VII close to the hepatocaval confluence was always present. Three of 10 patients were categorized into type 3, in which the distal confluence was formed by 2 tributaries, creating posterolateral drainage of the complete segment VII and anteromedial drainage of the rest of the right side of the liver (segment VI, part of segments V and VIII). Two of 10 patients were categorized into type 4, in which the distal confluence was formed by 2 tributaries from segments VII and VIII, respectively, while the accessory right hepatic veins, an inferior right hepatic vein alone, or an inferior right hepatic vein and a middle hepatic vein were always present.
DISCUSSION
In this case series, we reported 10 cases of LSGB in which all patients underwent laparoscopic cholecystectomy. Although LSGB is a rare anomaly, this study is one of the largest case series of it and is clinically significant because of the anatomic variations observed.
Most LSGB cases are diagnosed intraoperatively. In this study, 2 patients were diagnosed preoperatively according to abdominal CT findings, while the others were diagnosed intraoperatively. When we reviewed the abdominal CT findings, the 8 patients diagnosed intraoperatively could have been diagnosed preoperatively. Despite most of our patients being diagnosed intraoperatively, each laparoscopic procedure was performed safely.
When we performed conventional laparoscopic cholecystectomy, the second (for the left hand) and third (for the right hand) laparoscopic ports were inserted in the right upper quadrant and epigastric area of the abdomen. In laparoscopic cholecystectomy for LSGB patients, it was helpful for the surgeon to adjust the positions of the second and third laparoscopic ports in the left upper quadrant of the abdomen and epigastric area [1]. The location of the third working port was important to create a proper angle of dissection of Calot's triangle. The position of the third port can be determined after confirmation of the gallbladder's position through the second port. Also, it was more helpful to find cystic duct and cystic vessels that dissection of gallbladder bed was performed firstly, and then approaching the Calot's triangle was performed.
The IOC procedure, in which a catheter is introduced into the CBD for drainage of bile and injection of dye, can improve visualization of the bile duct anatomy and help the operator to avoid laparoscopic cholecystectomy induced damage [1617]. Some studies have suggested that the most cost-effective treatment strategy for most patients with symptomatic cholelithiasis involved laparoscopic cholecystectomy with routine IOC, as IOC could help surgeon to visualize the biliary anatomy and detect unexpected CBD stones [1819]. However, it remains debated whether IOC provides sufficient benefits in terms of its efficacy and safety to justify its routine application [1620]. In this study, there were no cases of IOC procedure to prevent bile duct injury in LSGB patient who underwent laparoscopic cholecystectomy. Early 4 cases underwent MRCP preoperatively for bile duct anatomy; of them, one also underwent ERCP due to CBD stones. In recent 5 cases, the operator could distinguish the cystic duct and CBD during the operation because of accumulated experience of the surgeon.
Bile duct and portal vein variations were observed in 10 patients with LSGB. The right posterior portal vein as the first branch of the main portal vein (type 3) was observed in all patients with LSGB [14]. In addition, 7 patients had segment IV branches of the left portal vein crossing over to the segment VIII territory. These variations may have important clinical implications in the management of cholecystectomy as well as in the hepatic resection including donor hepatectomy [521]. Combined hepatic anomalies can complicate or prevent the resection of hepatobiliary malignancies. Thus, it is essential to establish a specific surgical plan after a thorough evaluation of the combined anomaly and tumor extent [22].
Patients with LSBG are generally considered unsuitable donors; however, several cases of successful living donor transplantation have been reported, in which portal vein anomalies were recognized [232425]. Shimizu et al. [23] reported a patient with LSGB as a living liver donor in whom a right donor hepatectomy was performed in a patient with a right portal vein trifurcation anomaly. Hwang et al. [24] reported 3 cases of living donors with LSGB, among whom one had a bifurcating portal anomaly, intrahepatic right portal vein confluence, and extremely low bifurcation of the bile ducts, while the second donor had a trifurcating portal anomaly with a separate right posterior portal branch and replaced right posterior hepatic artery.
This case series found that the important feature of LSGB was the distribution of the left portal vein crossing over to the right side of the liver. In addition, a relative size reduction of the right portal vein, increased size of left portal vein, and portal vein supplying the left medial section extends to segment VIII of the liver, which was also observed in most patients.
In conclusion, although LSGB is a very rare disease, it is possible to diagnose it before surgery and safely perform laparoscopic cholecystectomy by adjusting the port positions. The common and important features of LSGB include the distribution of the left portal vein crossing over to the right side of the liver and increasing the size of the left portal vein. These variations may have important clinical implications in the management of hepatic resection including donor hepatectomy. To our knowledge, this is the largest case series of the clinical implications of LSGB and its anatomical variations.






 XML Download
XML Download