

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hip arthroplasty has emerged as one of the most successful orthopedic interventions. Many long-term follow-up studies have reported clinical success including patient satisfaction, pain reduction, functional improvement, and the absence of further surgery1). Various cementless stems have been developed to improve clinical outcomes and promote firm fixation123). Cementless rectangular tapered stems, which are fixed at the femoral metaphyseal-diaphyseal junction and provide stability mediated by three-point fixation in the proximal part of the diaphysis, have shown excellent clinical results456). Recent studies have shown that cementless rectangular tapered stems are associated with improved clinical outcomes compared with cemented stems78). Importantly, however, proximal radiolucency, calcar resorption, stress shielding, and thigh pain remain possible adverse events when cementless stems are used91011). The C2 stem (LimaCorporate SpA, Udine, Italy) is a rectangular tapered stem. To date, there have been no published clinical trials for the C2 stem among elderly Asian patients.
This study was designed to retrospectively evaluate the mid- to long-term clinical and radiological outcomes in Korean patients over 60 years of age who underwent hip arthroplasty using a cementless rectangular tapered stem; we hypothesized that these outcomes may vary depending on the proximal femur geometry.
MATERIALS AND METHODS
The design and protocol of this retrospective study were approved by the Institutional Review Board of Inha University Hospital (IRB No. INHAUH 2018-12-025-001). Informed consent was waived due to its retrospective nature.
1. Patients
A total of 107 patients (112 hips) who received hip arthroplasty using a C2 cementless femoral stem between January 2007 and December 2013 were enrolled in this retrospective study. There were 27 men (27 hips) and 80 women (85 hips) of mean age 77.4 years (range, 60–91 years). The preoperative diagnoses were fracture (n=99), avascular necrosis (n=7), and osteoarthritis (n=6). Bipolar hemiarthroplasty was performed in 90 patients and total hip arthroplasty was used in 22 hips using ceramic bearing couples (DELTA-PF cup; LimaCorporate SpA). All primary hip arthroplasties were performed through the posterolateral approach by a single experienced surgeon. The mean follow-up duration was 91.1 months (range, 60–116 months).
2. Stem
The C2 femoral stem used in this study has a rectangular section with sharp edges and consists of a titanium alloy (Ti6Al4V) component (6% aluminum and 4% vanadium); the entire stem surface was sandblasted except for the neck region (Fig. 1). The microstructure of such a rough surface is designed to better induce bone ingrowth1213). This stem is classified as a C3-type stem according to the Mont classification514).
3. Clinical Outcome Assessment
Patient follow-up was conducted at six weeks, six months, one year, and annually thereafter. We estimated Harris hip score (HHS), thigh pain, complications, and stem survival rate by reviewing patient charts just after surgery (i.e., postoperative) and at final follow-up. Thigh pain was assessed by hip physicians at follow-up visits, with a particular focus on starting pain and walking pain.
4. Radiological Outcome Assessment
One observer who had not been involved in the surgical procedures evaluated all radiographs. Preoperative radiographs were evaluated for Dorr type15), calcar-canal (CC) ratio, and cortical index (CI)16). Osteolytic lesions were recorded when they were detected during follow-up. Radiologic results (i.e., fit and fill, percentage of the canal filled by the stem at four levels) were evaluated using anteroposterior-view radiographs conducted at the five-year follow-up. These levels were named by Dorr et al.17) as calcar fill, metaphyseal fill, midstem, and distal fill. The presence of radiolucent lines (RLLs) and stress shielding were evaluated at final follow-up. The presence and extent of RLLs at the bone implant were measured according to Gruen criteria18). Stress shielding of the proximal femur was categorized into degrees of severity using Engh's classification19).
5. Statistical Analysis
Kaplan–Meier survival analysis was performed with the end point of revision time for any reason. Statistical analysis was performed using the ANOVA test for the results of the three Dorr-type groups. Preoperative and postoperative HHS were compared using a two-sample t-test. A comparison of fit and fill between with and without RLLs was conducted using an independent t-test. A P-value <0.05 was considered statistically significant. IBM SPSS ver. 19.0 statistical software (IBM Corp., Armonk, NY, USA) was used to analyze the data.
RESULTS
1. Radiological Outcomes
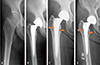
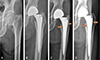
Preoperative femoral geometry was classified using the Dorr classification system (type A [n=20], type B [n=49], type C [n=43]). RLLs were observed in Gruen zones 1, 2, and 7 in 15 hips (13.4%). Generally, the lines appeared 2 to 12 months after arthroplasty (Fig. 2, 3). After the appearance of RLL, five hips (33.3%) remained unchanged with gradual sclerotic change of the outer margin. RLLs according to Dorr type are as follows: type A (n=6), type B (n=7), and type C (n=2). Patients with Dorr type C had significantly fewer RLL (4.7%) compared to types A (30.0%) and B (14.3%) (P=0.021) Stress shielding was observed in 48 cases and there was a significant difference between Dorr types: 12 in type A (60.0%), 24 in type B (49.0%), and 12 in type C (27.9%) (P=0.030) (Table 1, Fig. 4).
Calcar fill, CC ratio, and CI were 94.39±3.16%, 0.57±0.03, and 0.53±0.04 at five-year follow-up, respectively; these values were not significantly different among patients with Dorr types A, B, and C. Metaphyseal fill, midstem fill, distal fill, and lateral proximal fill were 95.77±2.82%, 81.45±5.49%, 69.16±12.58%, and 81.32±7.54% at five-year follow-up, respectively (Table 1). In those experiencing RLL, metaphyseal fill, midstem fill, distal fill, and lateral proximal fill were 94.27±4.60%, 83.47±5.85%, 72.69±14.43%, and 83.15±8.24%, respectively. Calcar fill was significantly lower in the group with RLL compared with the non-RLL group (P=0.033) (Table 2). There were no significant differences between Dorr types and the focal osteolytic area detected in two hips in Gruen zone 1 at postoperative two years and remained without change in size until final follow-up. No changes in the position of implants, including stem subsidence, were detected in this study.
2. Clinical Outcomes
There was a significant improvement in the mean HHS at final follow-up (90.5±15.9) compared with preoperative values (65.5±16.0) (P≤0.01). Pre- and postoperative HHS did not vary significantly among Dorr types. Nine patients (8.0%) experienced occasional activity-related thigh pain that was related to Dorr type (P=0.006) and RLL (P≤0.01) (Table 1, Fig. 4). Thigh pain was relieved in all patients within two years of surgery.
3. Complications
Two cases of periprosthetic femoral fracture occurred during stem implantation. All hips were treated with circumferential wiring and healed without complication. Hip dislocation was noted in three hips and all cases were treated with closed reduction and hip brace fitting. One stem revision was performed due to deep infection.
DISCUSSION
Cementless stems can be divided into different categories depending on their conceptual approach (i.e., fit and fill, proximal fitting, distal taper). The rectangular tapered stem was designed to fill the proximal femur as much as possible while reducing: i) the force delivered to the distal femur and ii) the biomechanical bending stiffness with the aim of limiting postoperative stress shielding and thigh pain. The Zweymüller stem, a typical rectangular tapered stem designed in Europe, reported to provide initial stability both axially and rotationally81220). The Zweymüller stem showed excellent clinical results in older patients with Dorr type B and C femoral geometry6112122). However, other papers reported complications associated with this stem type (e.g., thigh pain, proximal radiolucency, calcar resorption, stress shielding, and subsidence)91023).
The C2 stem is very similar to the Zweymüller stem in terms of their design, shape, and surface-coating. The greatest difference between the Zweymüller stem and the C2 stem is that there is no proximal lateral shoulder in the C2 stem. Additionally, the C2 stem has: i) sharp edges and a rounded section beneath the medial neck side for increased calcar contact area and ii) a distal end with a thinner conical shape compared to other rectangular stems.
In our series, 15 cases (13.4%) experienced RLLs in Gruen zone 1 or 7. Importantly, however, these RLLs did not expand or impact stem stability. The fine motion of the femoral stem causes bone resorption, and the fibrous membrane fills the gap between the femoral stem and inner cortex. This gap appears radiolucent in plain radiography. Choy et al.24) reported that RLL (zone 3, 4, and 5) was observed in 15% of patients after performing hip arthroplasty in elderly patients using a C2 stem. Although the RLL incidence in our study (13.4%) is similar to this study, there are notable differences in the zones involved. While further studies to better understand this observation are warranted, this difference may be explained by the surgical techniques used. Patients with Dorr type C femoral geometry experienced significantly fewer RLL (4.7%) compared to those with type A (30.0%) and type B (14.3%). Dorr type A femurs have wide metaphysis and narrow diaphysis15). Because of these structural features, the rectangular tapered stem does not fit the metaphyseal-diaphyseal junction of Dorr type A femurs, which leads to the fine motion of the femoral stem and RLL.
The most common adverse event following hip arthroplasty is persistent thigh pain25). The incidence of thigh pain in patients treated with cementless femoral stems has been reported to range from 10% to 20%26). Although the cause of thigh pain has not yet been clearly defined, fixation stability and stress transfer from the femoral stem to the endocortex are two commonly cited hypotheses25262728). In our study, nine patients (8.0%) experienced occasional thigh pain that was related to activities. The incidence of thigh pain and RLL varied significantly according to Dorr type (highest in type A). These data suggest that RLL and thigh pain are associated with femoral geometry. The average bone mineral density of the proximal femur among older Asians is lower compared with the Western population2930). Therefore, the use of a small C2 stem for these patients may induce a high probability of micromotion at the proximal femur.
This study has a several limitations. First, this study is a retrospective study and thus may be subject to a selection bias. Specifically, the uneven distribution of Dorr types and over-representation of femur neck fracture among patients might bias the results. Second, this study is limited by the relatively small sample size (n=112) and lack of longer follow-up (mean, 91.1 months) to assess implant survivorship. Despite these noted limitations, we believe that the number of cases and the follow-up length were sufficient to allow for an objective analysis. This study is meaningful in suggesting a relationship between femoral geometry and thigh pain when using this kind of rectangular tapered stem in elderly Asian patients.
CONCLUSION
The clinical results of hip arthroplasties using a C2 stem revealed a stem survival rate of greater than 97%; survival rates according to Dorr classifications were not significantly different. The incidences of RLL and thigh pain were correlated to femoral geometry (highest for patients with Dorr type A). Special attention is recommended when performing hip arthroplasty using C2 stems in elderly patients with Dorr type A femoral bone classification.




 XML Download
XML Download