

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporotic hip fractures are common enough to have a considerable impact on the healthcare system. Although hip fractures are commonly known to negatively affect the life expectancy of patients12), like the overall population, these patients have also begun to live longer because of improvements of general health status, and possibly, the advancement of patient care34).
Hemiarthroplasty (HA) is a common procedure for displaced intracapsular proximal femoral fracture (ICPF) and allows early full weight-bearing and functional rehabilitation. Limited studies have addressed the long-term outcomes of elderly patients with low-energy fractures treated with HA, however, given the current situation in many developed countries (i.e., aging populations), this issue now urgently demands attention. Two implant fixation techniques exist (i.e., cemented, cementless) and in the short term, both techniques are reported to have comparable functional results5678). Cemented HA is reportedly associated with: i) less thigh pain910), ii) better mobility11), and iii) a lower frequency of periprosthetic fractures61213). However, other studies have shown that cementless prostheses were associated with: i) a shorter operative time, ii) less blood loss2141516), iii) less complicated revision surgery17), iv) lower perioperative mortality, and v) no risk of bone cement implantation syndrome18192021). Long-term studies (>10-years) predominantly involve cemented HA222324); information about the long-term outcomes following cementless HA is limited. Furthermore, to the best of our knowledge, all mid- to long-term studies of HA in the English literature are limited to those from European countries, the ability to extrapolate these findings to individuals from East Asia remains unclear.
In this study, we aimed to assess implant survivorship (primary outcome) among elderly East-Asian patients who underwent cementless HA for low-energy ICPF and to evaluate procedure-related complications and functional outcomes among long-term survivors (secondary outcomes).
MATERIALS AND METHODS
The Institutional Review Board of Ohta-Nishinouchi Hospital approved this study which involved a retrospective chart review of 250 consecutive ICPF patients treated surgically between 2001 and 2007 at Ohta-Nishinouchi Hospital (Nishinouchi No. 26). Of these cases, we excluded those with the following conditions: i) internal fixation (n=43), ii) cemented HA (n=24), iii) age of initial injury under 60 years (n=10), iv) high-energy trauma (n=4), v) patients followed-up at an outside institution (n=30), and vi) missing data (n=4). In total, 135 cases of cementless HA were included in this analysis.
All patients in the study period were treated with bipolar head HA via the posterior approach25). During the study period at the institution, cementless HA was the standard or first-choice procedure, and cemented HA was performed only for cases with a trochanteric extension of the fracture, severe osteoporosis, or pre-existing deformity of the hip. We utilized a double wedge, metaphyseal filling stem as the first-choice implant when performing HA for osteoporotic fractures, unless preoperative templating revealed the shape of the proximal femur was mismatched to the type. The choice of specific implant within the same implant type was based on the treating surgeon's discretion. During the study period, all operations were performed by or under the direct supervision of board-certified orthopedic surgeons who had at least 5 years of experience in HA for hip fracture. From the first postoperative day, patients were mobilized and allowed full weight-bearing under supervision of a physiotherapist, unless an intraoperative fracture had occurred or the stability of the femoral component was in doubt. As standard protocol at the institution, patients were instructed—as far as their medical condition allowed—to visit the outpatient department at least once in the first 3 months, then every 6 months for the following 12 months, and once a year thereafter, or more frequently, based on the discretion of the treating physicians.
In all cases, we documented bone- or implant-related complications, including i) revision hip surgery for any cause with or without revision arthroplasty, ii) radiographic loosening/subsidence of the stem over 5 mm26), iii) dislocation of the HA head, iv) intraoperative fracture—defined as any fracture in the ipsilateral femoral bone recognized during surgery or on radiography immediately after the surgery, v) postoperative peri-prosthetic fracture, and vi) contralateral hip fracture. We also included surviving patients who were followed-up 10 years after the index surgery in the assessment of their functional states for pain, ambulation (bedridden, wheelchair, walker, cane, or without any aid), and residence (home, nursing facility, or hospital) as outcome measures.
We defined patients who were alive during at least 10 years of follow-up as a survivor and those who were deceased or lost from follow-up for any reason as a non-survivor and conducted statistical analyses of any potential differences in baseline demographics between these two groups using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan)27), a graphical user interface for the R environment (ver. 3.1.1). We used the Fisher's exact test and the Mann–Whitney U-test for binary and continuous variables, respectively; P-values less than 0.05 bilaterally were considered statistically significant.
RESULTS
During the follow-up period, patient dispositions were confirmed as deceased (n=48), unable to visit for follow-up because of: i) severe medical conditions (n=26), ii) a move to a distant place (n=5), and iii) transportation issues or other unknown reasons (n=30). This left 26 surviving patients who were followed-up 10 years after the index surgery in the final analysis. The mean age at injury was 78.3 years (range: 60–85 years) and at the final follow-up was 85.3 years (range: 74–96 years). The mean follow-up period of survivors was 11.3 years (range: 10–15 years). Compared to patients who did not survive, surviving patients: i) were younger at the time of injury, ii) included more female patients, and iii) had a lower preoperative American Society of Anesthesiologists grade (Table 1).
The implants used during the study period were Natural Hip® (Type 2 [double wedge]28); Zimmer Biomed, Warsaw, IN, USA; n=93), Synergy select II® (Type 2; Smith & Nephew, Memphis, TN, USA; n=20), CKA® (Type 2; KYOCERA Medical, Osaka, Japan; n=6), Bicontact® (Type 3A [tapered and round])28); Aesculap, Tuttlingen, Germany; n=3), Alloclassic® (Type 3C [tapered and rectangular])28), ODC® (Type 3A [tapered and round]28); Ortho Development, Draper, UT, USA; n=3), AML plus® (Type 4 [cylindrical and fully coated]28); DePuy Synthes, Warsaw, IN, USA; n=3, Zimmer Biomed; n=2), Meridian® (Type 2; Stryker, Kalamazoo, MI, USA; n=2), Reliance® (Type 3A28); Stryker, Kalamazoo; n=1), VerSys® (Type 2; Zimmer Biomed; n=1), and VECTOR-Titan® (Type 1 [single wedge]28); B.BRAUN, Melsungen, Germany; n=1).
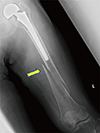
In terms of bone- or implant-related complications, one survivor underwent revision total hip arthroplasty because of the central migration of the bipolar head 15 years after HA. The patient had no history of osteoarthritis of the hip before the index surgery and demonstrated painful osteolysis of the acetabular bone (Paprosky type 2B29); Fig. 1 and 2). In one non-survivor, the Girdlestone procedure for septic loosening of the HA stem was conducted. The total revision rate was 1.5% (2/135). Six patients experienced asymptomatic sinking of the cementless stem, but no intervention was required (4.4%, 6/135). Only five non-survivors (3.7%, 5/135) presented with dislocation of the HA head; closed reduction was successfully achieved in all cases. No recurring dislocations requiring surgical intervention occurred. We observed intraoperative fracture only in non-survivors (Vancouver30) type A:3, C:1). In three cases of Vancouver type A, these fractures were noticed during the HA procedure, and the patients were treated with additional cerclage wiring performed simultaneously. In the first postoperative radiograph taken immediately after the surgery, one patient with undisplaced Vancouver type C was diagnosed and treated conservatively. Overall, there were eight instances of postoperative periprosthetic fractures (5.9%, 8/135): four cases among survivors and four cases among non-survivors. Among the survivors, three cases were classified as Vancouver type A and conservatively treated. The other case among the survivors was classified as Vancouver type B1 and required internal fixation with a plate (Fig. 3). All four non-surviving patients with periprosthetic fracture were conservatively treated. Of these, three patients had a Vancouver type A fracture, and one had a type B fracture. The patient with a type B fracture was considered inoperable because of concomitant respiratory distress. In two survivors and two non-survivors, contralateral hip fractures were observed during the follow-up period (3.0%, 4/135; Table 2).
Among survivors from whom ambulatory status information was available, six had secondary fractures (periprosthetic or contralateral), and two previously ambulating patients had become non-ambulatory after secondary injuries (7.7% of total survivors [2/26], 33.3% of patients [2/6] with secondary fractures). One of these two patients had a Vancouver type A periprosthetic fracture, and the other had a contralateral femoral trochanteric fracture.
An analysis of 10-year functional outcomes among survivors revealed that six patients (23.1%) complained of pain around the injured hip, but reported the intensity of pain was mild in most cases; only one patient required oral analgesics. Two patients experienced periprosthetic fractures, and no patient experienced femoral component subsidence or other complications. Twenty patients (76.9%) were still able to walk. Two cases had become wheelchair-bound, and two cases were bedridden. While 22 patients (84.6%) resided at home, four resided in nursing homes (Table 3).
DISCUSSION
In our study, 19.3% of the included patients were followed-up for over 10 years. Previous studies showed a mortality rate 1 year after hip fracture of 20% to 30%1431) and 10-year survival rates are reported to be 15% to 32.9%151632). To the best of our knowledge, this is the first reported long-term study on cementless HA in an Asian population in the English literature. Even including all drop-out cases in the denominator, the survival rate in our study was comparable to that of previous studies. Our surviving patients were younger and healthier than those who did not reach the 10-year follow-up mark (i.e., non-survivors), and these trends were similar to those in a previous report by Chatterton et al.31).
In this study, only two cases of revision were required, a revision rate lower than that in previous reports. Only a few studies have reported differences between over 5-year results for cemented and cementless HAs. Summarizing these previous reports (Table 4), the 10-year revision rates among survivors were up to 8.8% in cementless HAs and 2.4% to 3.5% in cemented HAs. In a retrospective study of HA patients older than 75 years of age with a follow-up of 12 to 19 years, Viberg et al.32) reported the hazard ratio of reoperation among patients treated with cemented HA as lower than that of patients with cementless HA. Most patients in these previous reports had revision arthroplasty within 5 years. Within the same time span, in our study, there was only one (0.9%) revision (for septic loosening). This lower incidence of revision hip surgery might be the result of difference in bodily habits and/or the lower prevalence of pre-clinical chondral injury in the acetabulum among East-Asians compared with Europeans. According to total hip arthroplasty studies, high body mass index (BMI)33) or body weight34) are associated with the risk of revision surgery after arthroplasty. Relatively low BMI and body weight among Asian patients might have a protective effect against symptomatic failure after HA. Additionally, a recent review reported that the prevalence of primary osteoarthritis of the hip is substantially higher, probably because of some genetic reasons, among European patients than that in other races; the prevalence was found to be 60 to 120 per million among European populations, whereas that in Asian population was <10 per million35). Furthermore, studies on osteonecrosis of the femoral head demonstrated that acetabular cartilage degenerative changes are commonly observed in patients with osteonecrosis of the femoral head, even when radiographs of the acetabulum appear normal36). In such cases, evidence showed that HA resulted in unacceptably high failure rates, mainly due to central migration of the prosthetic femoral head3738). Thus, it is suggested that pre-exiting acetabular cartilage lesions are more prevalent among European fracture patients, and a certain proportion of these lesions appears normal on radiographs eventually leading to high failure rate after HA.
In our study, the intraoperative fracture rate was 3.0%, which is comparable to the majority of other studies (range: 2.3–3.0%3940)). On the other hand, Chana et al.41) reported higher incidences of intraoperative fractures among patients who underwent cemented or cementless HAs: 5.9% and 15.2%, respectively. They concluded that cementless HA was a risk factor for intraoperative fracture. We believe this may have been caused by a technical issue in their procedure or the implant they used.
The incidence of postoperative periprosthetic fractures was reported to be higher among patients with cementless HA than that among patients with cemented HA (at 5 years, 5.7–15.2% in cementless and 0.9–5.9% in cemented)8134142). In these reports, periprosthetic fractures occurred mostly within 5 years. Viberg et al.32) also found most reoperation cases to be due to periprosthetic fractures (they did not demonstrate the exact percentages of underlying conditions) and 89.4% (42/47) of the total reoperation cases to be required within 5 years. In our cohort, although the overall incidence of periprosthetic fracture was 8.9%, only 6.7% (9/135) of patients experienced a periprosthetic fracture (including intraoperative fractures) within 5 years. Although this was high, the 5-year incidence of periprosthetic fracture was nevertheless lower than reported previously. The high intraoperative or early periprosthetic fracture rates in previous studies may be attributed to the technical challenges of surgery and/or the implant design during those earlier study periods.
Furthermore, in the follow-up period, 3.0% of our patients had contralateral hip fractures. Secondary hip fractures reportedly occurred in 2% to 5% of the proximal femoral fracture patients within one year of the initial injury43444546), and the highest risk of secondary hip fractures occurred in the first postoperative year4748). In our study, no patient had a contralateral fracture within 1 year. No studies of mid- to long-term results of HA mention contralateral fractures, but a patient's functioning can be greatly impacted by contralateral fracture. In our cohort, one of two contralateral hip fracture patients became non-ambulatory after the secondary injury; we believe that this issue cannot be ignored and should be addressed in future preventive studies.
An analysis of the 10-year functional status data revealed that most surviving patients were functionally able, and 76.9% of patients were pain-free or with occasional and/or mild pain which did not require analgesics. Our analysis of ambulation status suggested that long-term postoperative ambulatory and residential states were determined roughly within 3 months following the index surgery. Zhang et al.49) reported the effectiveness of intensive rehabilitation programs in the early recovery phase (<3 weeks) on the mobility of elderly patients with a femoral neck fracture, and their results indicated that the efficacy of early intense rehabilitation was maintained even at 1 year after surgery. Our results were consistent with their findings. Although functional outcomes are multifactorial, our results also highlight the importance of early rehabilitation for long-term functional results.
Because of the study design and characteristics of the patient population, this study inherently included several limitations. The first and biggest was the small, retrospective, single-center nature of our study, with no control. Additionally, detailed functional outcomes were only available for patients with over 10-year follow-up and we could not include several patient factors in detail (e.g., accessibility to rehabilitation facility in the assessment of functional outcome, complications). In this study, the surgical experience of the treating surgeons and choice of the implant, which might affect clinical outcomes, were not controlled. Lastly, the drop-out rate was considerable. The institution in which the study was conducted is located in a rural area with an elderly (over 65 years) population ratio of over 30%; more than half of these people lived alone or only with their spouses. Because the institution was the only tertiary referral center with well-functioning trauma service in that area, patients with conditions which required an immediate medical attention (e.g., dislocation, secondary fractures), were likely transferred to the institution; the results of analyses might have underestimated the proportions of complications among non-survivors because of this follow-up issue. Because of transportation issues and patients' medical/cognitive conditions, the follow-up is a major barrier for studies evaluating long-term outcomes in elderly patients5051). However, we strongly believe that such isolated elderly people can receive inestimable benefit from maintaining their mobility; thus, a further, direct, comparative study, with a proper follow-up strategy, is necessary to make robust recommendations.
CONCLUSION
Our results suggest that, among elderly East-Asian patients, the incidence of revision surgery after cementless HA might be lower, whereas the incidence of periprosthetic fractures was consistent with previous reports. Although most patients treated with cementless HA were functionally capable 10 years after the initial injury, a considerable percentage of survivors also sustained periprosthetic fractures and contralateral hip fractures.






 XML Download
XML Download