

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Pulmonary lymphangitic carcinomatosis (PLC) and pulmonary tumor thrombotic microangiopathy (PTMA) are lethal forms of pulmonary metastasis that can lead to sudden death. In clinical settings, it has been well documented that it is notoriously difficult to make antemortem diagnoses of them and therefore most cases have been confirmed on postmortem examination [12]. In those cases, several studies including bronchoscopy were performed for further evaluation. Bronchoscopy is widely used for diagnosis and treatment and is considered to be safe and effective. However, various complications can occur during bronchoscopy [3]. If a fatal complication such as sudden death occurs during bronchoscopy in a patient with PLC or PTMA, a potential medicolegal dispute can be anticipated, and postmortem examination is important to confirm the cause of death. In such cases, if lymphatic tumor emboli are observed frequently in the lungs but the features of PLC or PTMA are not predominant, it would be very difficult to determine the cause of death.
Herein we present a case of sudden unexpected death in a woman with PLC and PTMA due to gastric cancer, with review of literature. This study should be helpful to a forensic pathologist what should be considered from a perspective of forensic pathology.
Case Report
The deceased was 48-year-old woman who suddenly collapsed during a bronchoscopy. She had complained of cough and sputum that had lasted for about 3 months. She was initially diagnosed as reflux esophagitis but her condition did not improve with medications. She visited an outpatient allergy clinic at a university hospital, but the cause could not be determined despite several studies. The deceased visited another outpatient pulmonology clinic in the same hospital again because of recently occurred dyspnea, cold sweat, general weakness, loss of appetite, and a 10 kg weight loss over the past 6 months. The deceased was ultimately admitted for further evaluation. The chest computed tomography (CT) revealed diffuse interstitial thickenings and ground-glass opacities on both lungs. When compared to the chest CT from about 2 months prior, these pathologic findings were considered to be newly formed lesions. Her echocardiogram showed moderate pulmonary hypertension (right ventricular systolic pressure 60 mm Hg) with D-shaped left ventricle, an enlarged right atrium and right ventricle with reduced right ventricular systolic function, a small-sized left ventricle (LV) with normal global left ventricular systolic function, a relaxation abnormality of LV filling pattern, and mild tricuspid regurgitation. A blood test revealed anemia and thrombocytopenia. The abdominopelvic CT revealed an ulceroinfiltrative lesion in stomach (upper body, greater curvature), which suggested stomach cancer with serosal exposure. Multiple nodular lesions and peritoneal thickening were identified at left upper abdomen. There was no evidence of pulmonary embolism. Flexible bronchoscopy was performed under sedation. No endobronchial lesion or mucosal changes were identified and a transbronchial lung biopsy was done at the left lower lobe bronchus. During the procedure, the deceased became agitated with violent movement and was uncooperative even though physical restraint was applied. Fentanyl and midazolam were administered for sedation. After the procedure, Flunil was administered, and the deceased was intubated due to a reduction in oxygen saturation (SpO2 87%). Her heart rate suddenly dropped lower and led to cardiac arrest. Cardiopulmonary resuscitation was performed but the deceased expired. The deceased did not have any significant past medical history and the gastroscopy 2 years prior was nonspecific.
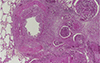
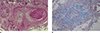
The deceased appeared well-nourished and healthy. On external examination, there were no significant injuries except small contusions on the arms and legs. There are also contusions with abrasions on the chest related to cardiopulmonary resuscitation and needle puncture marks on the arms and legs related to medical procedure. On internal examination, an advanced gastric cancer (10.0×7.0×1.0 cm, ulceroinfiltrative type, Borrmann type 3) was identified on the stomach (the greater curvature of the body). It extended to the serosa, hilum of spleen and the pancreas tail. The serosal surface of the lesion was adhered to the omentum and the mesentery. Small multiple nodules were identified on the omentum and the serosal surface of the sigmoid colon and rectum, as well as in the pouch of Douglas. Both ovarian surfaces were irregular. There were no emboli in pulmonary main arteries. The pleural surface of the lungs revealed prominent fine lymphatic network with mild fibrosis (Fig. 1). The cut surface of both lungs revealed multiple tiny nodules, and the interstitium appeared to be embossed. The left anterior descending coronary artery had fibrous atherosclerotic plaque with approximately 50% occlusion. The other internal organs were unremarkable. On microscopic examination, poorly differentiated adenocarcinoma was observed with invasion to the pancreas, serosa and perigastric soft tissue with lymphovascular and perineural invasion, and with metastasis to the lymph nodes, lungs, adrenal gland, kidneys, peritoneal cavity, omentum, ovaries, and colon. Both lungs revealed multifocal tumor emboli in the lymphatics of the pleura and the lung parenchyma (Fig. 2). Some tumor cells invaded the adjacent connective tissue and the bronchial wall in some bronchovascular trees (Fig. 3). Microscopic tumor emboli with thrombi and fibrointimal proliferation were also identified in some pulmonary arterioles (Fig. 4).
Lidocaine, atropine, midazolam, and fentanyl were detected within therapeutic levels on a toxicological test. Low thyroxine (T4) and free thyroxine (FT4) were observed, but triiodothyronine (T3) and thyroid-stimulating hormone were unremarkable. Eosinophil cationic protein (ECP) levels were higher on a postmortem blood test. We assumed that higher ECP level would be related to the deceased's condition of cancer with metastasis, given that ECP is considered to mediate anticancer effects [4]. Other ancillary tests, including blood alcohol concentration, biochemistry, tryptase and ketone bodies were unremarkable.
Although the deceased had advanced gastric cancer and multiple metastases with aggravating symptoms, it was a chronic condition and the deceased's condition seemed to be bearable. Her sudden unexpected death during bronchoscopy suggests the possibility of various complications related to bronchoscopy. There are some limitations with evaluating such complications, however, as the evaluations are dependent on the clinical information. Therefore, the cause of death was ruled to be undetermined.
Discussion
This case illustrates an unexpected sudden death during bronchoscopy in a patient with advanced gastric cancer (poorly differentiated adenocarcinoma) with multiple metastases including pulmonary tumor emboli with some features of PLC and PTMA. Her initial clinical presentation was sustained cough and recently occurred dyspnea with a loss of appetite and weight loss. This suggests that the deceased may have had chronic debilitating disease including malignancy, which is consistent with gastric cancer with multiple metastases. The deceased's condition went downhill but did seem to be tolerable, which would not enough to explain the sudden unexpected death. During bronchoscopy, the deceased was agitated with violent movement and was uncooperative, despite the use of physical restraint. And then bradycardia and cardiac arrest occurred, which led to sudden death. This clinical course suggests the possibility of functional abnormality or cardiovascular complications related to bronchoscopy. It is not easy, however, to prove this directly based on the findings of the postmortem examination.
Sudden unexpected deaths can occur in patients with malignancy [5]. One study showed that the causes of death in these patients were acute myocardial infarction, aortic dissection, thrombotic pulmonary emboli, cardiac involvement by malignancy, cardiac tamponade, neoplastic pulmonary emboli, esophagoaortic fistula, duodenal-inferior vena cava fistula, hepatic rupture, and anaphylaxis reaction due to drugs. However, this case did not fall into any of these categories. In this case, there were no emboli in the main branches of the pulmonary arteries, and the other internal organs, including the heart and aorta, were unremarkable.
The deceased's lungs revealed multifocal tumor emboli in the lymphatics of the pleura, the bronchovascular trees, and the septal space. In some bronchovascular trees, the tumor cells invaded the adjacent connective tissue and the bronchial wall with fibrosis. These findings indicate the possibility of PLC, which can be a lethal form of pulmonary metastasis. Of the patients with malignancy, 30%–40% can metastasize into the thoracic region, and 6%–8% of them might have lymphangitic carcinomatosis [6]. Nine cases of PLC in patients with gastric cancer have been reported as hospital cases [1789]. Eight cases were young adults where the possibility of malignancy was unlikely to be considered due to their young ages. The initial impressions in these cases were thus interstitial lung disease, collagen vascular diseases, and infectious diseases. Six of these patients expired within 4 to 48 days, and one experienced partial remission after 2 months of chemotherapy. The remaining patient was lost to follow up. The other case was similar to this case in that it involved a middle-aged woman with worsening dyspnea and weight loss, but she was lost to follow up. These were hospital cases where the patients' symptoms and conditions deteriorated despite treatment, ultimately leading to death. In this case, however, the deceased was still in tolerable condition, although the deceased's condition went downhill with newly developed dyspnea. In the lungs, the thickening of the bronchovascular trees and septa, and dilatation of pleural lymphatics were not predominant, as tumor cell invasion or stromal reaction such as fibrosis were only identified in some areas of the lungs. This may explain why the deceased's condition was still tolerable.
PTMA is another lethal form of pulmonary metastasis that is related to microscopic vascular tumor embolism. The clinical manifestations of PTMA are pulmonary hypertension, right heart failure, and sudden death. The pathologic findings of PTMA are characterized by microscopic tumor emboli in small pulmonary arteries with fibrointimal proliferation. In most studies that are based on autopsy cases, the primary cancer was gastric cancer [21011]. Like PLC, it was hard to diagnose upon antemortem examination, and in most cases, diagnoses were made after postmortem examination. In this case, the deceased's echocardiogram showed pulmonary hypertension and her blood test revealed thrombocytopenia. On microscopic examination, microscopic tumor emboli with thrombi were found only in some pulmonary arteries, and fibrointimal proliferation was observed in a few arterioles. These findings suggest that the deceased also had some characteristic features of PTMA. However, it is not enough to explain the deceased's sudden unexpected death, because the histologic features of PTMA were not predominant and were observed only in some areas of the lung.
Given that the deceased expired during a bronchoscopy, it is important to consider the possibility of a fatal complication related to sedation and bronchoscopy. The toxicology test revealed medications which are assumed to be administered for sedation, and those drugs were detected within the therapeutic levels. According to the medical record, the deceased appeared to have been closely monitored during sedation and bronchoscopy. The oral cavity and larynx were unremarkable, as was the level of tryptase. Based on these findings, complications related to sedation or anaphylaxis are unlikely to be considered. Complications related to bronchoscopy include active bleeding related to endobronchial biopsy, myocardial infarction, preexisting pulmonary disease, respiratory arrest, and cardiac arrest due to unknown causes [31213]. In this case, there was no bleeding or injury in the main bronchi and bronchioles, and there was no endobronchial lesion. Given that the sudden death occurred following hypoxemia, bradycardia and cardiac arrest, cardiovascular complications related to bronchoscopy should be taken into consideration. During the procedure, cardiac arrhythmias, which are mostly related to the occurrence of hypoxemia can occur in response to complex cellular dysfunction that is due to the metabolic effects of severe acute hypoxia [13]. Interestingly, in a pediatric case of a 15-years-old female with PLC [14], bronchoscopy was performed for further evaluation and she was intubated and mechanical ventilation were applied to her after the procedure. This finding also suggests that bronchoscopy may have aggravated the clinical course of PLC. Therefore, we hypothesized that the sudden death of the deceased with PLC and PTMA, may have been induced by cardiovascular complications related to bronchoscopy. There are still some limitations to this study. We were dependent on the medical records to obtain the clinical information that was needed to evaluate the possible complications during sedation and to ascertain whether the deceased was closely monitored. Furthermore, a cardiovascular complication related to bronchoscopy is a diagnosis of exclusion based on clinical information.
In summary, we present a case of sudden unexpected death during bronchoscopy in a patient with PLC and PTMA due to gastric cancer. PLC and PTMA are the lethal lesions of pulmonary metastasis, but the extent and severity of them should be meticulously examined with clinical information. When unexpected death occurs during bronchoscopy and complications related to the procedure considered, postmortem examination is very important with review of the medical records. Given that some complications are diagnoses of exclusion, clinical information may be the only key to the correct diagnosis.


 XML Download
XML Download