

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mortality rates in pancreatic surgery have declined markedly throughout the last decade due to the advancement of surgical methods and imaging techniques;123 however, morbidity rates remain high for distal pancreatectomy (DP).45 The most life-threatening complication of DP is a postoperative pancreatic fistula (POPF). The incidence of POPF after DP has been reported to range from 18.6 to 64.9%.67 POPF causes a variety of complications, such as intra-abdominal abscess, delayted gastric emptying, and postoperative hemorrhage. Therefore, early diagnosis and treatment of POPF are of vital importance.
Leukocytosis is frequently found in the early postoperative period after major surgery. Although leukocytosis may be a sign of developing infection in the early postoperative period, it may also be part of a normal surgical response. Systemic inflammatory response syndrome (SIRS) is considered a useful parameter for early detection of postoperative complications and end-organ dysfunction after gastrointestinal surgery.8 One of the diagnostic criteria for SIRS is a white blood cell (WBC) count >12k cells/µl or <4k cells/µl. Thus, it is reasonable to infer that a higher WBC count in the post-operative blood test after DP indicates a worse prognosis.
Interestingly, in clinical practice, it is uncommon to find a WBC count >20k cells/µl on postoperative day 1 (POD1) following DP, raising questions about the use of this parameter as a predictor of complication following DP. Therefore, in this study, we investigated whether a WBC count >20k cells/µl on POD1 influences the postoperative course following DP for benign and low-grade malignant tumors of the left-side of the pancreas.
Go to : 
MATERIALS AND METHODS
Study design
The Yonsei Institutional Review Board approved the current study protocol (4-2018-1114). The medical records of 474 patients who underwent DP from December 2005 to December 2016 were retrospectively reviewed using the Electronic Medical Record Database. Among them, patients with malignant pancreatic tumors (n=179) and DP secondary to primary cancer surgery (n=35) were excluded (Fig. 1). Patients were categorized into two groups according to their WBC count on POD1: >20k cells/µl (Group 20K-High) or <20k cells/µl (Group 20K-Low). Perioperative outcomes were compared according to WBC count on POD1.

Data collection
Perioperative variables, including age, gender, body mass index (BMI), length of hospital (LOH) stay, operative time, estimated blood loss (EBL), intraoperative transfusion (Yes/No, ml), reoperation, readmission, and surgical approach (distal pancreatectomy with splenectomy [DPS] vs. spleen-preserving distal pancreatectomy [SPDP]), were retrospectively determined. Additionally, the WBC counts on preoperative day, operation (OP) day, POD1, POD2, POD3, POD5, POD7, and day 1 of out-patient department (OPD) follow-up were collected. Complications were classified according to the Clavien-Dindo classification system.9 POPF was defined by the amylase level in the drainage fluid on POD3 based on the (Internal Study Group of Pancreatic Fistula (ISGPF) guidelines.10
Statistical analysis
Continuous variables were described as mean±standard deviation, and categorical variables were described as frequency (%). Student's t-test, Chi-square test with Fisher's exact test, and linear-by-linear association were performed using SPSS 20.0 for Windows (SPSS Inc., Chicago, IL, USA). The resultant p-values <0.05 were considered to be statistically significant.
Go to :
RESULTS
Patient characteristics
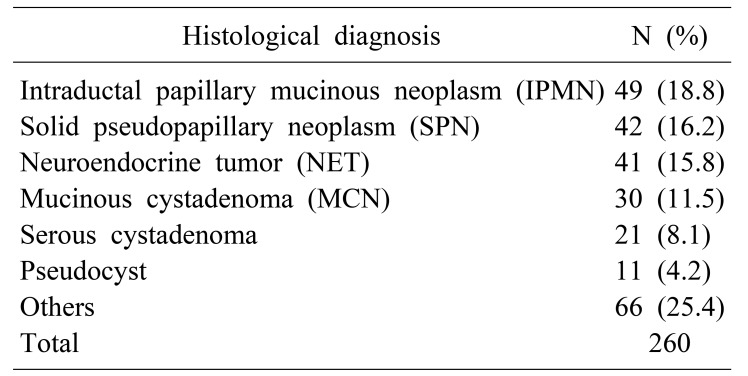
Of the 260 intention-to-treat patients, 164 (63%) were female. The average patient age was 51.75±15.2 y. The preoperative mean BMI was 23.09±3.2 kg/m2. Intraductal papillary mucinous neoplasm (IPMN) of the pancreas was the most common pathologic condition (18.8%), and solid pseudopapillary neoplasm (SPN) was the second most common (16.2%; Table 1).
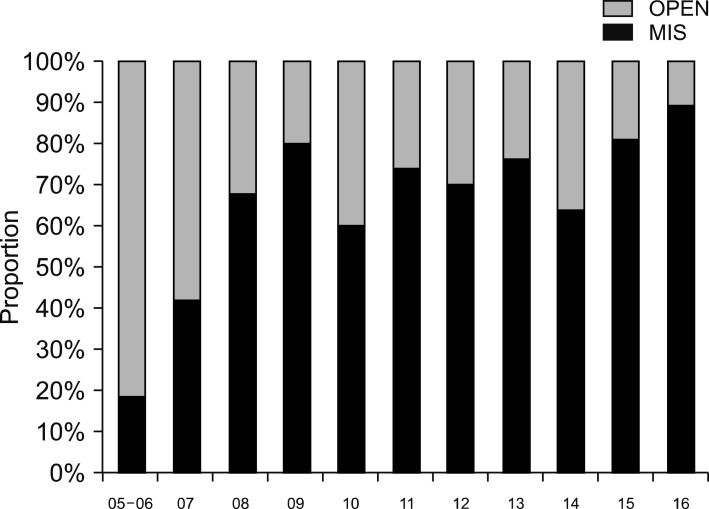
Among the study population, 84 (32.3%) patients underwent open surgery, while the remaining 176 (67.6%) patients underwent minimally invasive surgery (MIS). It was found that the use of MIS for DP increased annually (Fig. 2; p<0.001). Among the MIS patients, 36 (13.8%) underwent robot-assisted surgery, and 140 (53.8%) underwent laparoscopic surgery. Combined splenectomy was performed on 146 patients (56.2%). The mean operative time was 235.4±90.9 min. The mean length of hospital stay was 11.88±10.0 d. Of the total number of patients, 12 (4.6%) were categorized into Group 20K-High, and the other 248 (95.4%) were categorized into Group 20K-Low.
Postoperative WBC count after DP in Group 20K-High and Group 20K-Low
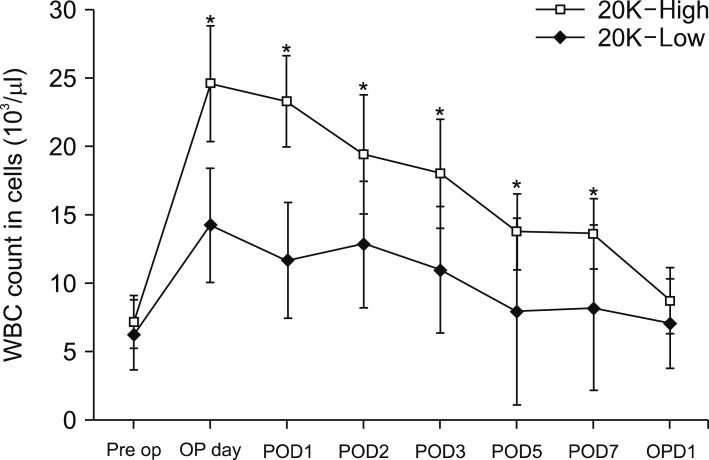
The WBC count of Group 20K-High and Group 20K-Low were significantly different on OP day, POD1, POD2, POD3, POD5, and POD7 (Fig. 3). There was no statistically significant difference between the groups, however, on pre-operative day (7.19±2.57 vs. 6.28±1.90, p=0.12) or day one of OPD (8.75±3.26 vs. 7.09±2.41, p=0.14). Furthermore, there was no statistically significant difference in mean time from discharge day to first OPD between Group 20K-High and Group 20K-low (10.92 vs. 10.85 days, p=0.97).
Comparative analysis of perioperative outcomes between Group 20K-High and Group 20K-Low
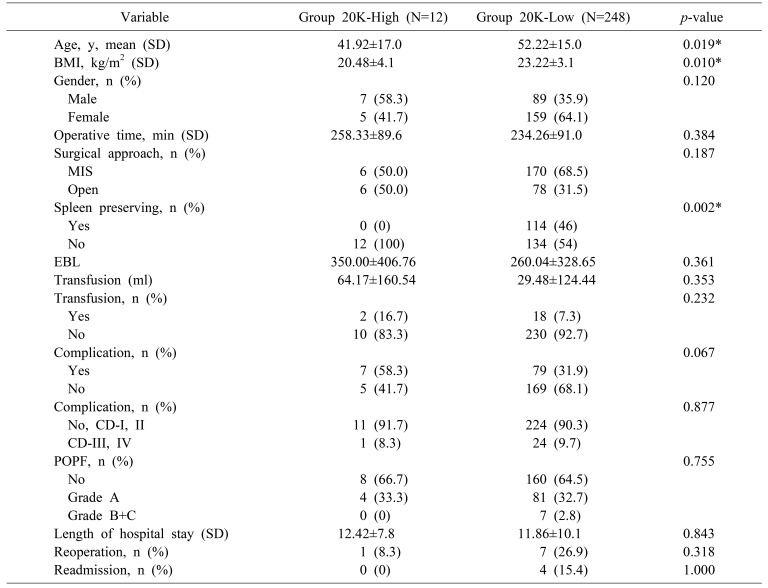
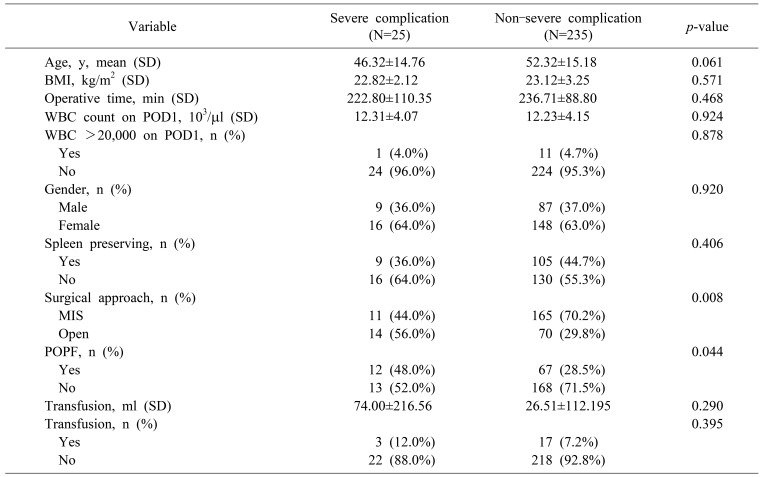
There was no statistically significant difference between Group 20K-High and Group 20K-Low with respect to gender, operation time, surgical approach, estimated blood loss, intraoperative transfusion, length of hospital stays, reoperation, or readmission (p>0.05). The overall complication rate was slightly higher in Group 20K-High with marginal significance, but the frequencies of clinically relevant major complications, including POPF, were similar between the two groups (Table 2). However, it was shown that age (41.92±17.03 years vs. 52.22±15.00 years, p=0.019), BMI (20.48±4.08 kg/m2, vs. 23.22±3.06 kg/m2, p=0.01), and spleen-preserving rate (0% vs. 46%, p=0.002) were significantly different between the two groups.
Prediction of severe complications CD-III/IV following DP
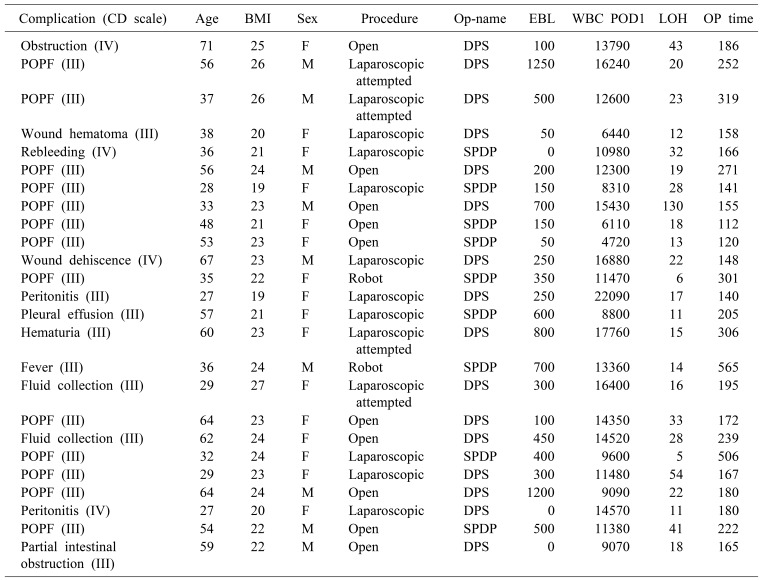
Table 3 shows the severe complications following DP. According to the Clavien-Dindo classification, 25 patients (9.6%) had complications classified as grade III (n=21) and IV (n=4). There was pancreatic leakage in 13 patients (52%), sustained abdominal pain with free air (peritonitis) in 2 patients (8%), fluid collection in 2 patients (8%), and wound complication in 2 patients (8%). Since 2005, the number of cases of DP increased, but the rate of severe complications decreased annually (p<0.001, Fig. 4), with no noted cases of severe complications in 2015 and 2016.
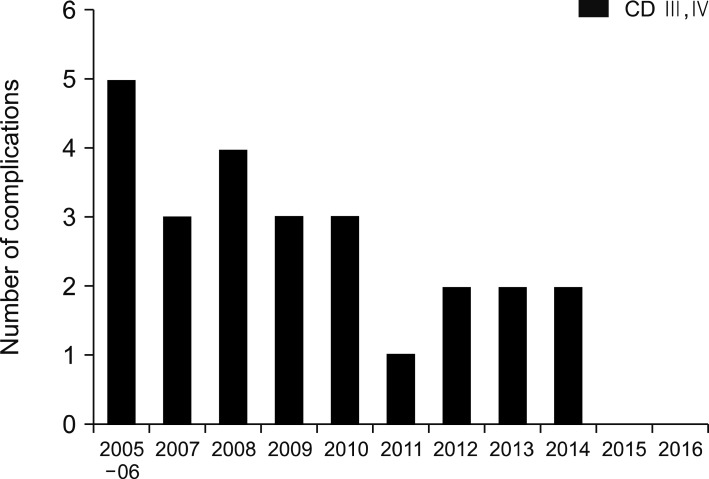 | Fig. 4Incidence of CD-III/IV complications after DP. There was annually decreasing trend (p<0.001). CD, calvien-dindo; DP, distal pancreatectomy.
|
Table 3
Summary of severe complications following DP
CD scale, clavien dindo scale; BMI, body mass index; Op-name, operation name; EBL, estimated blood loss; WBC POD1, white blood cell(count) postoperative day 1; LOH, length of hospitalization; Op-time, operation time; DPS, distal pancreatectomy; SPDP, spleen preserving distal pancreatectomy; POPF, postoperative pancreatic fistula
![]()
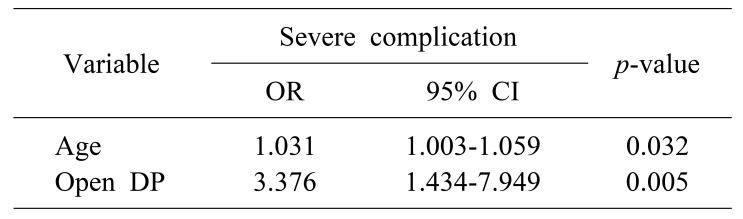
Univariate analysis demonstrated that surgical approach (p=0.008) and POPF (p=0.044) were associated with severe complications following DP (Table 4). Age was noted to have a marginal relationship with severe complications (p=0.061). WBC count over 20K on POD1 was not associated with severe complications after DP (p=0.878). Subsequent multivariate analysis showed that age (OR=1.031, [95% CI: 1.003–1.059], p=0.032) and surgical approach (OR=3.376, [95% CI: 1.434–7.949], p=0.005) were associated with severe complications (Table 5).
Go to :
DISCUSSION
POPF is the most serious complication in patients undergoing DP. POPF after DP has been reported in as many as 40% of patients, and this rate is higher than after pancreaticoduodenectomy.111213 Objective data from perioperative laboratory tests may help surgeons predict complications after surgery;1415 however, the prognostic significance of the WBC count in surgical patients with infection has not been thoroughly assessed. This study sought to predict the development of POPF or other severe complications after DP using the POD1 WBC count.
An elevation in WBC count can be used as a prognostic marker for infection or inflammation, but a variety of factors can lead to such elevation in otherwise asymptomatic individuals. Observational studies often fail to show an association between WBC extremes and infection in the immediate postoperative period in the surgical population.1617 POPF after DP may lead to a systemic inflammatory response with leukocytosis and fever, resulting in a more complicated postoperative recovery and prolonged hospitalization. Thus, it is hypothesized that there is an association between POD1 leukocytosis and postoperative complications due to infection.
In this study, we enrolled 260 patients with benign and low-grade malignant tumors in the left side of the pancreas and retrospectively compared the postoperative outcomes of two groups (Group 20K-High and Group 20K-Low) based on their WBC count on POD1 after DP. Twelve (4.6%) of 260 patients in Group 20K-High associated with young age (p=0.019), low BMI (p=0.01), and splenectomy (p=0.002). The high WBC count of Group 20K-High gradually decreased to near normal levels between POD7 and day 1 of OPD. A high WBC count immediately after the postoperative period was not associated with POPF or any severe complications. Multivariate analysis showed that age (OR=1.031) and open DP (OR=3.376) were independent factors capable of predicting severe complications following DP.
Since Velanovich18 reported in 2006 the first comparative study between laparoscopic DP (LDP) and open DP (ODP) and concluded that LDP produced surgical results equivalent to OPD, there have been several studies showing that MIS in DP is associated with decreased morbidity.1920 Our retrospective results support that MIS in DP is associated with fewer severe complications. The potential association between severe complications and open DP was analyzed in this study by comparing the proportions of severe complications according to the laparoscopic approach used. Recent meta-analyses comparing LDP and ODP have shown the superiority of LDP in terms of intraoperative blood loss, patient recovery, and hospital stay.7212223 The first multicenter patient-blinded randomized control study of MIS in DP versus ODP (LEOPARD) reported MIS reduced the time to functional recovery compared with ODP.24
We found that a WBC count >20K cells/µl on POD1 after DP was a clinically uncommon phenomenon that occurred in only 12 (4.6%) of 260 patients with DP. A postoperative WBC count >20K cells/µl was found in the combined splenectomy group, and it returned to a normal range without clinically relevant severe complications. Thus, a WBC count >20K cells/µl appears to be a physiologic change associated with splenectomy but not with severe complications after surgery. Previous reports2526 demonstrated that DPS is associated with a statistically significant increase in postoperative WBC and platelet counts. Kehoe et al.27 also demonstrated that leukocytosis and thrombocytosis are common in upper abdominal surgery after a splenectomy. Additionally, investigators reported efforts to identify the mechanism underlying splenectomy-related leukocytosis.28 These studies suggested that the spleen exerts an inhibitory effect on bone marrow cell release and that after splenectomy, the circulation loses a factor that promotes cell apoptosis, thereby increasing the WBC count. Our results are in agreement with these findings, indicating that splenectomy is the most important factor for POD1 leukocytosis, as elevated WBC counts in the DPS group decrease to near-normal levels between POD7 and day 1 of OPD.
A major limitation of this study is the retrospective design and the limited number of patients. In addition, during the long study period, there may have been significant differences in postoperative techniques and perioperative management. Therefore, significant differences in severe complication rates between our early and late time periods were evident, as the standardized surgical techniques for DP changed during that time (p<0.001). Nonetheless, it is interesting to note that the complication rate decreased annually. With increasing laparoscopic or robotic enhancement and the development of new surgical techniques, DP has become safer even during the course of this study. Currently, the MIS technique should be considered the operation of choice.
POD1 WBC counts >20K cells/µl are not common following DP. POD1 WBC counts >20K cells/µl were related to a physiologic phenomenon resulting from combined splenectomy, not found to be a useful predictor of severe complications following DP. Instead, severe complications were found to be associated with age and open DP. Therefore, it may not necessary to imply clinical significance of the WBC count on POD1 after DP. It should be considered as a physiological change associated with the splenectomy. Surgeons are advised to apply laparoscopic or robotic surgery when performing DP in well selected patients with benign and low grade malignant tumor of the pancreas.
Go to :
 XML Download
XML Download