

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prognostic nutritional index (PNI) is calculated using the following formula: 10×serum albumin concentration (g/dl)+0.005×lymphocyte count (number/mm3) in the peripheral blood.1 Thus, this index reveals patients' immune status and nutritional condition. A low PNI indicates malnutrition, reduced neutrophil function, and reduced immunity.23 Additionally, a low preoperative PNI is reportedly associated with a high incidence of postoperative complications.4 Moreover, a significant correlation has been between a low preoperative PNI and poor survival of patients with various neoplasms.567 These reports indicate that the preoperative PNI may be a good prognostic indicator for patients with cancer.
The prognosis of patients with pancreatic ductal adenocarcinoma (PDAC) is extremely poor. Even if curative resection is performed, many patients die of cancer recurrence within a few months. Yamamoto et al.8 reported that the median survival duration of 195 patients who underwent pancreatic resection was 27.1 months. Additionally, Sato et al.9 reported that in patients who had undergone resection of PDAC in Japan, the estimated 5-year disease-specific survival rate was 23.1% and the disease-free survival rate was 16.8%. Moreover, postoperative complications such as anastomotic leakage between the pancreatic duct and the jejunum after pancreaticoduodenectomy (PD) or pancreatic fistula formation after distal pancreatectomy (DP) occur very frequently after resection of the pancreas. Thus, the nutritional status of many patients with PDAC is likely insufficient during treatment. However, changes in the postoperative PNI compared with the preoperative level and the relationship between the postoperative PNI and patients' prognosis have not been thoroughly studied. Therefore, we evaluated the clinical importance of the preoperative and postoperative PNI as a prognostic marker in patients with PDAC.
PATIENTS AND METHODS
Patients
From 2006 to 2017, we enrolled 50 patients who were diagnosed with operable PDAC and underwent curative resection (no residual tumors macroscopically) at Tottori Prefectural Central Hospital. The patients' details are shown in Table 1. Clinical and pathological staging of PDACs was performed using the American Joint Committee on Cancer 6th edition TNM staging system for pancreatic cancer.10 All patients were followed up at Tottori Prefectural Central Hospital until April 2019. No patients received chemotherapy or radiation therapy before the operation. Informed consent for medical treatment and use of clinical data from the medical records was obtained from all patients.
Surgical procedure
All patients underwent open laparotomy. According to the tumor location, we performed DP with splenectomy in 15 patients, PD in 27 patients, PD combined with portal vein partial resection in 6 patients, and total pancreatectomy with splenectomy in 2 patients. Reconstruction after PD with or without partial resection of the portal vein was performed by Child's method. An internal short stent was placed across the pancreatojejunostomy, but no stent was placed following choledochojejunostomy.
Postoperative complications
Postoperative complications were analyzed by reviewing the patients' clinical data. The severity of postoperative complications was graded according to the Clavien Dindo classification.11 Clavien Dindo grade ≥III complications were considered major complications.
Clinical data
We recorded clinical parameters including the operation time, postoperative hospital stay, and occurrence of postoperative complications. Blood samples were routinely taken from each patient at the time of admission to our hospital. The serum albumin concentration, total lymphocyte count, and level of the tumor marker (carbohydrate antigen 19-9, CA 19-9) were recorded. The reported reference range of the serum CA 19-9 level is 0 to 37 U/ml.12 Additionally, the PNI was calculated preoperatively and at 1 and 2 months postoperatively. This study was approved by the ethics review board of Tottori Prefectural Central Hospital (approval number: 2019 - 2).
Statistical analysis
Differences between two normally distributed parameters were compared using the χ2 test and Fisher's exact probability test. Wilcoxon's signed rank test was used to assess the correlation between the two numerical parameters (preoperative and postoperative PNI). The Mann Whitney U test was used to compare differences between two parameters with non-normal distributions. Long-term overall survival (OS) was calculated using the Kaplan–Meier method, and the prognostic difference between the two groups was compared using the log-rank test. All data were analyzed by StatView software (Abacus Concepts, Inc., Berkeley, CA, USA). A p value of <0.05 was considered statistically significant.
RESULTS
The mean PNI at 1 month postoperatively was 39.8 (range, 14–57.2), which was significantly lower than the preoperative PNI of 45.5 (range, 27.8–57.6; p<0.001). The mean PNI significantly recovered to 42.7 (range, 16.9–59.5) at 2 months postoperatively compared with that at 1 month postoperatively (p=0.002). However, the PNI at 2 months postoperatively did not reach the preoperative level (p=0.045, Fig. 1). In 23 patients, the PNI at 2 months postoperatively recovered to the preoperative level (recovered group), but in the remaining 27 patients, the PNI at 2 months postoperatively did not reach the preoperative level (non-recovered group). At 1 and 2 months postoperatively, the PNI in the recovered group was significantly better than that in the non-recovered group (p<0.001, Table 2)
Major postoperative complications occurred in 40% of patients. One patient died of postoperative peritonitis secondary to leakage at the pancreatojejunostomy site 3 months postoperatively. Thus, the operative mortality rate in our series was 2%. The mean postoperative hospital stay among the 20 patients with major postoperative complications (54.9 days) was significantly longer than that among the 30 patients without postoperative complications (21.6 days, p<0.001). However, we found no significant correlation between the preoperative PNI and the occurrence of postoperative complications (p=0.751). Among the 27 patients in the non-recovered group, 22 underwent PD or total pancreatectomy (81.5%). Although this proportion of patients was higher than that in the recovered group (13/23, 56.5%), the difference was not statistically significant (p=0.055).
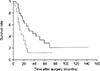
The 5-year OS rate of the 50 patients was 14.4%, and the median OS time was 18 months. The correlations between the median OS time and the eight candidate factors (patients' age, operative procedure, operation time, tumor stage, occurrence of postoperative complications, preoperative CA 19-9 concentration, preoperative PNI, and postoperative PNI) among the 50 patients are shown in Table 3. The 50 patients were divided into 2 subgroups for each parameter according to the median values (patient age, operation time, and preoperative PNI). We found that only the postoperative PNI was an important risk factor for poor survival in patients with PDAC in the univariate and multivariate survival analyses (Tables 3, 4). Fig. 2 shows the OS curves of the patients.
DISCUSSION
Surgical resection is an essential treatment modality for many potentially curable solid tumors. However, surgery induces alterations in patients' immune function. Surgical tissue damage promotes a strong inflammatory response and suppresses components of the immune system that protect against cancer. Thus, such surgical stresses can reportedly accelerate cancer growth and the risk of recurrence and may be correlated with poor patient survival.131415
PD with or without portal vein resection, DP with splenectomy, and total pancreatectomy with splenectomy are common operative procedures for PDAC. These operative procedures are associated with a long operation time and large blood loss volume, and in some cases, blood transfusions are required intraoperatively and postoperatively. Moreover, many patients develop postoperative complications. Thus, the surgical stresses of PDAC resection may be much greater than those of other gastrointestinal malignancies. Such surgical stress may be a poor prognostic factor for patients with resected PDAC.
The PNI represents patients' nutritional and immunological conditions. This index is designed to assess the nutritional and immunological status of patients. A low preoperative PNI has been used to estimate the occurrence of postoperative complications, and the postoperative PNI can be used to assess patients' recovery from operative damage. Murakami et al.16 recently reported the prognostic importance of comparison between the preoperative and postoperative PNI in patients with gastric cancer. Thus, in the present study, we focused on the changes in the PNI during the preoperative and postoperative periods as a new prognostic indicator for patients with PDAC. We analyzed the PNI of patients with PDAC at three time points (preoperatively and 1 month and 2 months postoperatively). We found that in 23 of 50 patients, the PNI at 2 months postoperatively recovered to the preoperative level, however, in the remaining 27 patients, the PNI at 2 months postoperatively did not recover. We also found that among several preoperative prognostic indicators in patients with PDAC, including the preoperative PNI, recovery of the PNI after the operation was a strong prognostic indicator in both the univariate and multivariate survival analyses.
Improvement of the nutritional status before and after the operation may improve the postoperative prognosis in patients with PDAC.





 XML Download
XML Download