

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the introduction of laparoscopic cholecystectomy (LC) in 1985,1 it has been accepted as the gold-standard surgical procedure for benign gallbladder (GB) diseases. With the development of laparoscopic skills and equipment in response to the demand for cosmesis after surgery, efforts have moved towards reducing wound size and postoperative pain. After single-incision laparoscopic cholecystectomy (SILC) was described in 1997 by Navarra et al.,2 several studies have been conducted to demonstrate the benefits of the procedure compared to conventional LC. Three studies using a wound satisfaction score detected significantly improved cosmetic appearance provided by SILC compared with LC.345 Other studies demonstrated significantly reduced postoperative pain in the SILC cohort.678 However, an overall complication rate of 7.3% and ductal injury rate of 0.39% were reported in previous studies, which exceed those of conventional LC.9101112 According to a recent review article by Greaves and Nicholson, “As surgeons, we should not advocate for slightly improved cosmetic value over safety”.13 Due to technical difficulties and safety issues, SILC was introduced 20 years ago but is still not considered a standard procedure.
Some surgeons consider SILC to be associated with frequent deviations from safe standards and believe that evidence regarding such techniques offering any real benefit to patients is lacking.14 This is because SILC is a difficult procedure and the total wound size is similar to that associated with conventional LC. Furthermore, the procedure can be stressful for the surgeon.
When performing SILC, the operator and camera operator (scopist) share the operative field, which limits the operator's activity (Fig. 1A). This exacerbates the clashing of instruments, which is the major limitation of SILC procedures.15 These issues result in a steep learning curve for SILC. Our center started performing solo SILC (Solo-SILC) in 2014. Our variation uses the parallel method rather than the crossing method. This widens the activity range of the operator and solves difficulties associated with the crossing method. A solo surgery is defined as a procedure in which the surgeon alone manipulates all instruments, including the camera, to avoid communication problems and unnecessary camera movements (Fig. 1B).16 Recently, our center reported that Solo-SILC is a feasible technique in a small group of patients.17
With the above in mind, this report describes the technique, short-term outcomes, and learning curve of Solo-SILC with the aim of helping other surgeons overcome the initial learning period smoothly and safely.
MATERIALS AND METHODS
A total of 664 patients underwent Solo-SILC at Seoul National University Bundang Hospital from July 2014 to December 2016. Of these, we extracted the data of 591 patients who underwent Solo-SILC performed by four hepatobiliary surgeons with ≥2 years of clinical experience in hepatobiliary surgery (surgeons A–D). The prospectively recorded data of the patients were collected and retrospectively reviewed. Surgeons A, B, and C had independently performed >50, 100, and 80 consecutive conventional LCs. They started to perform Solo-SILC immediately despite having no experience of SILC. They trained in Solo-SILC and 3-port LC simultaneously. Surgeon D is a highly experienced surgeon who had performed >500 conventional LCs. Moreover, before starting to perform Solo-SILC, surgeon D had experienced 10 cases of SILC before changing the surgical procedure because of difficulties with the solo and parallel method.
Solo-SILC is performed for all patients with benign GB diseases at our institution. If the patients had an American Society of Anesthesiologist score (ASA) >3 or were unable to tolerate general anesthesia due to other reasons, they were excluded from the study.18 To compare the severity of disease, we categorized the presence of preoperative percutaneous transhepatic biliary drainage (PTGBD) and emergency surgery. We compared the presence of preoperative fever (℃), white blood cell (WBC) count (103/L), and C-reactive protein (CRP) (mg/dl) levels. The parameters used to assess surgical outcomes included operative time (min), estimated blood loss (EBL) (ml), use of additional trocars, the presence of GB stones and their maximal size (mm), insertion of a Jackson-Pratt drain, GB perforation during surgery, length of hospital stay (days), complications, and histologic diagnosis of resected GB. All patients who underwent Solo-SILC received the same clinical pathway for postoperative management. If there were no problems, patients were permitted sips of water 6 hours after surgery. Laboratory examinations were performed on postoperative day 1. If there was no issue with diet or postoperative problems, the patients were discharged on postoperative day 1. To clarify the learning curve, we used the simple moving average method with operative time as the measure of improvements in technique. We reviewed the studies through MEDLINE to compare outcomes and learning curves between Solo-SILC and SILC.
Surgical technique
Position of the patient
The patient is placed in the supine position with the legs straightened and apart. The operator is positioned between the patient's legs during the main procedures. The laparoscopic scope holder (Laparostat™, CIVCO Medical Solutions, IA, USA) is positioned around the level of the lowest margin of the left rib. The monitor is located above the patient's head. The diathermy pedal is placed near the surgeon's right or left foot (Fig. 1B, C).
Single port placement and patient position
A longitudinal 2–2.5-cm trans-umbilical incision is made (symptomatic GB stones or chronic cholecystitis suspected: 2 cm; acute cholecystitis suspected: 2.5 cm). After an incision is made, 0.5-% bupivacaine hydrochloride is injected into the wound to relieve postoperative wound pain. After it has been confirmed that there are no adhesions around the umbilicus in the peritoneal cavity, a Glove port (Nelis, Bucheon-si, Gyeonggi-do, Korea) is inserted through the incision site. Pneumoperitoneum is induced and maintained at 12 mmHg. The patient is then placed in the reverse-Trendelenburg position with a left-sided tilt.
Manipulating instruments using the parallel method
As the camera (10-mm laparoscopic flexible scope [Olympus CV-190, Shinjuku-ku, Japan]) is placed at the upper area of the single incision site, two conventional laparoscopic instruments are inserted through the lower side holes (Fig. 1D). The parallel method is used instead of the crossing method. This establishes a triangular approach between the target organ and the two instruments and allows the instruments to perform push/pull movements while minimizing sideways movement. This push/pull movement reduces the overlapping activity range between the two instruments (Fig. 1E). The left instrument grabs the fundus of the GB and pushes it to exposure the hilar area. In the case of adhesions around the liver, a large quadrate lobe hiding the hilar area, or difficulty when exposing the hilar area, an Endo-grab or Organ retractor (AESCULAP Inc. U.S.A) can be used to retract the GB. The operator alters the surgical view during the operation by manipulating the laparoscopic camera holder.
Specimen extraction and closure
After isolating and dividing the cystic duct and cystic artery, the GB is dissected from the liver and extracted through the glove port. If GB perforation occurs during the procedure, we use a laparoscopic vinyl bag to reduce the risk of abdominal cavity infection and bile leakage during GB extraction. The pneumoperitoneum is reduced to 5–6 mmHg to identify the minor bleeding point before the retrieval of instruments.
The umbilical port site is then repaired using interrupted sutures in the fascia layer with only 1–2 intradermal sutures at both ends of the skin incision site for skin closure and drainage for fluid collection in the umbilicus.
Statistical analysis
All statistical calculations were performed using the SPSS software package for Windows, version 21 (IBM Corporation, Armonk, NY, USA). The demographic and clinicopathological characteristics were summarized using descriptive analysis, and all qualitative values are presented as means and standard deviations unless expressed otherwise. The statistical analysis was performed with one-way analysis of variance and the Tukey post-hoc honest significant difference test. A p-value <0.05 was considered statistically significantly.
RESULTS
Patient characteristics and pre-operative findings
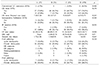
During the study period, 121 patients underwent Solo-SILC performed by surgeon A (n=37), B (n=51), and C (n=33). Surgeon D performed 470 cases of Solo-SILC during the same period. The patients' preoperative baseline demographics and pre-operative findings are shown in Table 1. The mean age was 55.0±17.02, 52.8±15.34, 57.6±16.09, and 53.2±15.52 years for patients treated by surgeon A, B, C, and D (p=0.424). The mean body mass index (kg/m2) was 24.77±3.29, 25.84±4.14, 24.93±3.41, and 24.72±4.04 for patients treated by surgeon A, B, C, and D (p=0.35). The proportion of each gender did not differ significantly among the groups (p=0.74). No significant differences were found in the history of abdominal surgery (p=0.361). Although, ASA score was significantly higher in patients treated by surgeon C and D (p=0.001), the incidence of diabetes mellitus was not different among the groups (surgeons A:B:C:D=18.9%:17.65%:9.1%: 13.8%, p=0.473). The proportion of patients who underwent insertion of a PTGBD or ERBD before the operation was not different among the groups (p=0.312). Thirteen (35.1%), 13 (25.5%), nine (27.3%), and 171 (36.6%) patients treated by surgeon A, B, C, and D were emergency cholecystectomy cases (p=0.604). Local and systemic signs of inflammation, including the presence of fever, preoperative WBC counts, and preoperative CRP level, were not significantly different (pre-operative fever, p=0.26; preoperative WBC counts, p=0.254; pre-operative CRP level, p=0.34).
Surgical outcomes and histologic diagnosis of the resected GB
The surgical outcomes and histologic diagnoses of the resected GB are shown in Table 2. The mean operative time (min) was 63.59±18.71, 60.49±23.39, 91.36±26.93, and 54.85±24.72 in patients treated by surgeon A, B, C, and D (p=0.000), respectively. The mean EBL (ml) was <5, 5.88±23.76, 18.78±45.86, and 7.29±61.59 in patients treated by surgeon A, B, C, and D (p=0.57). Additional trocar insertion was required in one (2.7%), zero, one (3.0%), and 21 (4.5%) patients treated by surgeon A, B, C, and D (p=0.444). Conversion to open surgery occurred in one case due to bile duct injury in the patients treated by surgeon C. A drainage tube was placed in zero, two (3.9%), three (9.1%), and 17 (3.6%) patients (p=0.252). There was no difference in the presence of GB stones or their maximal size (mm) (GB stones, p=0.263; GB stone maximal size (mm), p=0.184). As mentioned above, all patients who underwent Solo-SILC received the same clinical pathway. The mean hospital stay was 1.72±1.86, 1.54±0.90, 2.0±1.98, and 1±2.01 days in patients treated by surgeon A, B, C, and D (p=0.663).
Complications
During the mean follow-up period (24±7.2 months), the incidence of postoperative complications was not significantly different among the different surgeon groups (p=0.27) (Table 3). Wound infection (total incidence, 10 of 591 [1.69%]) and incisional hernia (total incidence, 5 of 591 [0.85%]), which resolved without special treatment, occurred in all study groups. Three postoperative complications that delayed bile leakage occurred in patients treated by surgeon D (0.63%). These complications were resolved by ultrasound-guided puncture and drainage. One patient underwent endoscopic retrograde cholangiography due to abnormalities on liver function tests after surgery and was diagnosed with common bile duct stricture.
Learning curve of Solo-SILC
Fig. 2 shows the learning curve of each surgeon. The operative time stabilized for surgeon A after 14 cases (learning period: 64.85±6.72 min; experienced period: 62.73±19.31 min; p=0.04), for surgeon B after 12 cases (learning period: 62.51±20.86 min; experienced period: 60.89±23.33 min; p=0.04), and for surgeon C after 12 cases (learning period: 102.75±29.50 mins; experienced period: 84.38±21.51 mins; p=0.013).
DISCUSSION
This study demonstrated that the learning curve of Solo-SILC was approximately 12–14 cases for hepatobiliary surgeons who are experienced in conventional LC. In addition, the surgeon who was fluent in both LC and SILC had no learning curve when starting to perform Solo-SILC. In the patients treated by surgeons A, B, C, and D, there was one case of bile duct injury (0.17% [1 of 591]). This was lower than the overall rate of bile duct injury for SILC (0.39% [9 of 2236]) across all previous studies.31920 Moreover, the mean operative time in this study group (59.93±25.77 min) was shorter than that reported in other studies of SILC (median operative time across studies=80.75 [range 40–186] min).21
Hodgett et al. demonstrated a consistent operative time for 29 patients undergoing SILC.22 Pan et al.23 concluded that surgeons who are experienced in conventional LC are likely to pass the learning curve after performing 20 cases of SILC. Mutter et al.24 did not show any significant reduction in operative time with increasing experience. Compared to the above results, the present study showed a relatively short learning curve for Solo-SILC, and the mean operative time was shorter than that in other studies. The learning curve is influenced by operator skill, surgical procedures, the surgical team, and the surgical devices used. When performing SILC, a skilled scopist is required to visualize the surgical field. However, the number of experienced scopists is insufficient and they have a fixed working time, which limits the practice of SILC in Korea. An unexperienced scopist who is not familiar with the surgical procedures might cause the surgical view to be unstable. However, in the case of Solo-SILC, the procedure is performed by one surgeon who understands the entire procedure. This eliminates miscommunication between the operator and scopist. Therefore, the learning curve of SILC is influenced by the scopist, whereas Solo-SILC is influenced only by the skill of the operator. This study revealed that stabilization of surgical skill is achieved more rapidly when Solo-SILC is performed.
In our center, the equipment and surgical procedures of Solo-SILC are standardized by the experienced surgeon D. This surgeon used trial and error while implementing SILC, and introduced and standardized the Solo-SILC program to train other hepatobiliary and pancreatic surgeons. Recently, surgeon D has been performing solo single incision laparoscopic hepatectomy.25 Surgeons A, B, and C, who have been trained in Solo-SILC with a relatively standardized procedure, were able to overcome the learning curve relatively quickly despite having no experience of SILC. The primary concern and source of skepticism for many surgeons considering the place of SILC is the frequent deviation from standards.13 However, this study shows that standardization of procedures can ensure stability. Several studies have described SILC using the crossing method to overcome the left-right reversal of in struments.1415 In our center, we use the parallel method, which is similar to the conventional instrumental manipulation method. The most important thing when starting a new procedure is patient safety. As shown in Table 3, the total complication rate was 3.21% in the present study. There were only 24 (3.72%) cases of additional port insertion and one case of open conversion (0.17%). As Table 4 shows, when comparing these outcomes with those of SILC, the patient safety provided by our novel approach to Solo-SILC is acceptable.
There are several methods for assessing a surgeon's learning curve. The ideal approach is to use multivariate logistic regression or the cumulative sum method, both of which have been used recently.2627 These methods usually use outcome-related variables, such as the rate of conversion to open procedures and the occurrence of severe complications. In this study, the rate of open conversion was 0.83%, with a rate of Clavien-Dindo classification >IIIa complications of 0.83%. Considering these rates, we deemed that it was appropriate to use a moving average method to assess the learning curve. Among the variables for evaluating skill when performing SILC, operative time is the most direct and accurate indicator because it reflects a surgeon's mastery of the technique.
This study has several limitations that should be noted. First, this was a retrospective study, which means that the possibility of selection bias cannot be excluded. Second, the follow-up period was short. A longer follow-up will be required to confirm our findings and investigate other issues, such as the rate of incisional hernia. Third, the results of resected GB histology included acute cholecystitis, GB empyema, GB gangrene, and xanthogranulomatous inflammation. In the early period, we performed Solo-SILC for suspected symptomatic GB stones or chronic cholecystitis. With the accumulation of cases, the indications for Solo-SILC were expanded to include acute cholecystitis.
In conclusion, this study reports that hepatobiliary surgeons experienced in LC can overcome the learning curve of Solo SILC within 12–14 cases. Moreover, a surgeon with more experience in conventional LC and SILC experienced no learning curve. Solo-SILC is a technique that can overcome the shortcomings of SILC after the learning curve and provide a more stable surgical option. Solo-SILC is a promising treatment for GB disease.




 XML Download
XML Download