

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cholangiocarcinomas account for approximately 3% of all gastrointestinal malignancies, with a prevalence in autopsy studies of 0.01 to 0.46 percent. In the United States, the incidence of bile duct cancer is between one and two patients per 100,000 people and 3,500 cases occur every year.1 However, South Korea has been reported to be one of the countries with a high incidence of bile duct cancer.2 Of the 214,701 newly-registered cancer patients in 2015, patients with extrahepatic bile duct cancer ranked ninth and had the sixth highest mortality rate in South Korea.3 Cholangiocarcinomas can be classified into intrahepatic cholangiocarcinomas and extrahepatic cholangiocarcinomas according to their location. Extrahepatic cholangiocarcinoma can be further classified into hilar cholangiocarcinomas (HLC), mid-bile duct cancer, and distal bile duct cancer (CBDC).45 Hilar cholangiocarcinoma (HLC) involves the common hepatic duct and the confluence of the left and right hepatic duct and accounts for 60–70% of all extrahepatic cholangiocarcinomas.6 Middle-to-distal cholangiocarcinomas (CBDC) account for 20–40% of the extrahepatic cholangiocarcinomas.7
The primary treatment for cholangiocarcinoma is surgical treatment but it has been reported that only 10 to 40% of patients with cholangiocarcinomas could be resected.8 Curative surgery for cholangiocarcinoma depends on the site of tumor development. Pancreaticoduodenectomy is usually performed for CBDC. For the resection of HCC, right or left hepatectomy and caudate lobectomy are frequently necessary, in addition to bile duct resection, depending on the extent and direction of the invasion into the liver. If radical surgery for cholangiocarcinoma is not possible, palliative surgery is considered. Several studies have reported that the prognosis for HLC was worse than that for CBDC.910 The possible cause of the difference is that symptoms, such as jaundice and cholangitis, develop more quickly, so can be diagnosed quickly in CBDC. The relatively higher resection rate in CBDC is due to the lower incidence of liver and major vessel invasions compared to HLC.11
The purpose of this study was to compare the prognosis of HLC and CBDC after curative resections in our hospital.
MATERIALS AND METHODS
Patient and data collection
From January 1990 to December 2013, 281 patients underwent surgery for extrahepatic bile duct cancer in the Department of Surgery at the Korea Cancer Center Hospital, Seoul, South Korea. We selected T2 and T3 patients based on AJCC (American Joint Committee on Cancer, 7th edition) criteria who successfully underwent curative resections. There were 139 patients in the study. Among the 139 patients, 74 patients had hilar cholangiocarcinoma and 65 had distal bile duct cancer.
Clinical data, including age, sex, tumor markers, transfusions, operative complications, and 90-day hospital mortality; and pathologic data, including T stage, N stage, and histological differentiation were collected for the patients retrospectively. We analyzed the clinical data and compared the survival results between the hilar cholangiocarcinoma and distal bile duct cancer groups. In addition, the prognostic factors for all 139 patients were analyzed.
This study was approved by the institutional review board of the Korea Institute of Radiological and Medical Sciences (KIRAMS) (IRB no. 2018-11-007).
The data were analyzed using IBM SPSS STATISTICS KOREAN VERSION 23, Kaplan-Meier analysis, Cox regression analysis, and chi-squared test. p-values less than 0.05 were considered statistically significant.
RESULTS
Sex, age, tumor markers, operative complications, hospital mortality, T-stage, histological differentiation, and lymph node metastasis were not statistically different between the HLC and the CBDC patients. In the HLC patients, right hemihepatectomies with extrahepatic bile duct resections were performed in 29 patients, right trisectionectomies with extrahepatic bile duct resections in 24 patients, left hemihepatectomies in six patients, left trisectionectomies in five patients, hepato-pancreatico-duodenectomies in eight patients, extrahepatic bile duct resection in one patient, and pancreatico-duodenectomy in one patient. In the CBDC patients, pancreatico-duodenectomies were performed in 59 patients and bile duct resections were performed in six patients (Table 1).
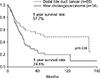
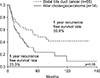
In the HLC patients, R1 resections were done in 23 patients (31%) and in the CBDC patients, R1 resections were performed in eight patients (12%). The difference between the R1 resection rates between the groups was statistically significant (p=0.006). The 5-year overall survival rate was 24.5% in the HLC group and 51.7% in the CBDC group. The difference between the 5-year overall survival rates were statistically significant (p=0.039) (Fig. 1). In the T2 patients, the 5-year overall survival rate of patients with HLC was not different from that of the CBDC patients. In contrast, in the T3 patients, the 5-year survival rate of the HLC patients was 15.5% and that of the CBDC patients was 59.5 percent. The difference was statistically significant (p=0.043) (Fig. 2). The 5-year overall survival rate of HLC in N0 patients was 28.6% and that of the CBDC patients was 70.0 percent. The rates were statistically significant (p=0.001). In the N1 patients, the 5-year overall survival rate in patients with HLC was 14.1% and was not statistically different from CBDC, which was 29.3 percent (Fig. 3).
In the R0 resection patients, the 5-year overall survival rate of patients with HLC was 19.8% and that of CBDC was 55.5%, which was significantly different (p=0.019). The 5-year overall survival rates of HLC and CBDC were not statistically different in patients with R1 resections (Fig. 4).
The 5-year recurrence-free survival rate of HLC was 23.3% and this was lower than that of the CBDC patients, but this difference was not statistically significant (p=0.06) (Fig. 5). The 5-year recurrence-free survival rate of T2 HLCs was 26.6% and that of the CBDC T2 group was 47.1%, but the difference was not statistically significant (p=0.300). The 5-year recurrence-free survival rate of T3 HLC was 23.1%, and that of distal bile duct cancer was 55.7%, but the difference was not statistically significant (p=0.102) (Fig. 6). In N0 patients, the 5-year recurrence-free survival rate based on cancer location was statistically significant (p=0.001), with a 5-year recurrence-free survival rate of 23.2% for HLC patients, while that for CBDC patients was 60.6 percent. The 5-year recurrence-free survival of patients with HLC and CBDC did not differ significantly in N1 patients (p=0.667) (Fig. 7).
In the R0 resection patients, the 5-year recurrence-free survival rate of the HLC patients was 21.5% and that of the CBDC patients was 50.8%, which was statistically significant (p=0.039). The 5-year recurrence-free survival rates of R0 patients in the HLC and CBDC groups were not significantly different (Fig. 8).
Multivariate analysis revealed that lymph node metastases and hilar tumor locations were independent poor prognostic factors for both the overall and recurrence-free survival rates in these patients (Table 2).
DISCUSSION
Occasionally, extrahepatic bile duct cancer is found at an advanced stage.1213 Surgical removal of the extrahepatic bile duct cancer ensures the highest survival rate, so surgery should be considered whenever possible.14 Previous studies have suggested that the factors affecting recurrence and survival after the surgical resection of extrahepatic bile duct cancer are invasion to adjacent organs; perineural invasion; lymphovascular invasion; lymph node metastasis; TMN stage; alkaline phosphatase, total bilirubin, direct bilirubin, aspartate aminotransferase, alanine aminotransferase, and gamma-glutamyl transferase levels; tumor differentiation status and blood transfusions.1516 The results of adjuvant treatment for extrahepatic bile duct cancer, such as chemotherapy and radiotherapy, are not satisfactory.17 But a few recent studies showed a slight survival gain.18 Gabriel et al.19 reported that gemcitabine plus cisplatin for biliary cancer provided survival benefit. Moureau-Zabotto et al. reported that the conformal-3D external-beam-radiotherapy (EBRT) seemed efficient to treat locally-advanced and unresectable extrahepatic cholangiocarcinomas, with acceptable toxicity.20
Many studies have demonstrated that the prognosis for HLC was worse than that for CBDC.2122 Park et al.23 reported that the 5-year survival rate of patients with extrahepatic cholangiocarcinoma, on the site of the tumor, were higher in CBDC. The histologic structure of the extrahepatic bile duct can be different depending on its location. In the hilar area, the muscle fiber is scattered. But the distal bile duct consists of smooth muscle bundles. Although differences in the degree of tumor invasion have been investigated, the fibromuscular, subserosa, and serosa layers are very thin histologically, therefore, it is difficult to distinguish the infiltration limit between them.24 Differences in local invasion or lymph node metastases due to these anatomical and histologic differences may lead to differences in survival rates but currently, there is no definitive consensus in the literature. Baek et al. reported that there was no difference in prognosis related to the location of bile duct cancer and that R0 resection was the most important factor affecting prognosis.25
In our study, a total of 281 patients underwent surgery for extrahepatic cholangiocarcinomas. However, the number of patients with T1 was small and curative resections frequently could not be performed in the patients with T4. Therefore, we selected patients with only T2 and T3 stage cancers who underwent successful resection for our study. In this study, a hilar location of the cholangiocarcinoma was an independent poor prognostic factor.
In R0 resected patients with HLC, the prognosis was poorer than for those with CBDC. In R1 resected patients, the prognosis was poor and not different between HLC and CBDC patients. The rate of R1 resection was higher in HLC patients. The rate of transfusion was higher in hilar cholangiocarcinoma patients. When multivariate analysis was performed, tumor site (hilar location of cholangiocarcinoma) and lymph node metastases were independent poor prognostic factors. R1 resection was not an independent prognostic factor.
Lymph node metastasis is well known as an important prognostic factor affecting survival or recurrence in patients with extrahepatic bile duct cancer. Choi et al. reported that the 5-year survival rate was 50.4% in patients who had no lymph node metastases compared to a 13.0% 5-year survival rate in patients with lymph node metastases.26 Yoshida et al.27 also reported that lymph node stage was an independent prognostic factor. Patients with up to two positive lymph nodes had a more favorable prognosis than that of other patients. The authors recommended pancreaticoduodenectomies with extended lymphadenectomies and adjuvant chemotherapy for the treatment of patients with CBDC. Kitagawa et al.28 analyzed the patterns of lymph node metastases of HLC and emphasized that aggressive lymphadenectomy was necessary because the pericholedocal node was the most common site of lymph node metastasis and that metastasis occurred along the lymphatic drainage system. Patients with lymph node metastases also had significantly lower overall survivals and recurrence-free survivals in this study.
This study revealed that the prognosis for HLC patients was worse than for CBDC patients under curative surgical conditions. However, in cases of lymph node metastases or R1 resections, the prognosis was poor and not different between patients with HLC or CBDC.
In conclusion, we should do our best to perform R0 resections to achieve better prognoses. The development of new adjuvant treatment methods for extrahepatic bile duct cancers with lymph node metastases is necessary. Further studies into the cause of the differences in survival rates between HLC and CBDC patients are needed.








 XML Download
XML Download