

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nontuberculous mycobacteria (NTM) are ubiquitous in the environment and are found in soil, tap, fresh, salt water, animals, milk and food.1 Although infection is rare in immunocompetent subjects, exposure to environments colonized by NTM is an important route of disease acquisition in children. Outbreaks in the community associated with common contaminated sources including swimming pools or ponds have been reported.2 NTM has also been known as an important source of healthcare-associated infection through contaminated medical equipment3 or via cosmetic procedures.45 NTM infection leads to four main clinical syndromes, including pulmonary disease, lymphadenitis, skin and soft tissue infection, and disseminated disease.13
Among immunocompetent children, cervico-facial lymphadenitis is a predominant clinical presentation, which mostly has been reported to affect children between one and five years of age.3 The majority of cases are caused by Mycobacterium avium complex (MAC), which includes M. avium and M. intracellulare. Other important pathogens of lymphadenitis include M. haemophilum, M. malmoense, and M. kansasii.1 Submandibular nodes are most commonly affected, followed by preauricular, and submental lymph nodes.6 Early diagnosis is difficult as most lesions are generally associated with minimal or negligible tenderness or heating sense. Also, patients rarely experience constitutional symptoms including fever, weight loss, malaise, and night sweats.1 Later in the course of disease, patients may show discoloration (red to purple) with thinning, peeling, and scaling of the overlying skin.7
NTM lymphadenitis is an under-recognized entity and data on the true burden is limited. Its risk has been known to be reduced with Bacille Calmette-Guérin (BCG) vaccination.3 Cases among healthy children are rarely reported in Korea where BCG vaccination is included in the national immunization program. In this study, we report a cluster of ten cases of NTM lymphadenitis that occurred during an 18-month period at a single tertiary hospital.
METHODS
Study subjects
Subjects under 19 years of age who were diagnosed with NTM lymphadenitis at Seoul National University Bundang Hospital, Seongnam, Korea were included in the study. Electronic medical records were reviewed for clinical, laboratory and pathology findings in a retrospective manner. Information regarding underlying health conditions and environmental exposure factors; such as, BCG vaccination history, tuberculosis or NTM exposure history, household activities, outdoor activities, utilization of public facilities, exposure to pets or animals and travel history, was obtained via questionnaires and direct interviews.
Microbial identification and pathology
For NTM identification, biopsies were obtained for microbiologic and histopathologic examination. Acid-fast bacteria (AFB) smearing and mycobacterial cultures were performed at 28°C–30°C in special medium enriched with hemin. The species of the causative NTM organism was identified via polymerase chain reaction (PCR) amplification and sequencing for rpoB and hsp65. PCR for Mycobacterium tuberculosis (MTB) was done with fresh tissue and PCR for MTB and NTM (AdvanSureTM MTB/NTM RT-PCR kit; LG Life Sciences, Seoul, Korea) was done with formalin-fixed, paraffin-embedded (FFPE) specimen. Gomori methenamine-silver (GMS) and periodic acid-Schiff (PAS) staining was performed for the possibility of fungal infection.
NTM lymphadenitis case classification
Patients were classified into three categories: confirmed, presumptive, and suspected. “Confirmed” cases were defined as NTM identified by AFB culture or NTM PCR positive. “Presumptive” cases included subjects which showed typical histopathological and clinical findings of NTM lymphadenitis with no evidence of tuberculosis or fungal infection. “Suspected” cases showed typical clinical features of NTM lymphadenitis including subacute (duration longer than 3 weeks), unilateral, nontender lymphadenitis not responding to empirical antibiotics with none or limited systemic symptoms and exclusion of MTB (Table 1).
Table 1
Case definition of NTM lymphadenitis

RESULTS
Clinical characteristic of NTM lymphadenitis
During the study period, ten patients with cervicofacial lymphadenitis were diagnosed with NTM lymphadenitis. A cluster of nine patients was identified during a relatively short six-month period (November 2016–April 2017) and one more patient was encountered (April 2018) one year later. All ten patients were male, previously healthy with BCG vaccination history, and were between 8–15 years of age (Table 2).
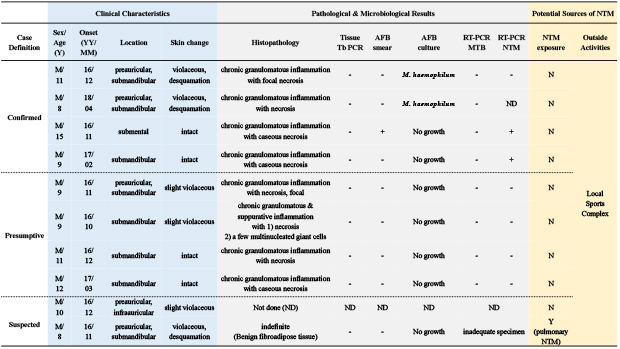
Table 2
Clinical characteristics, sonographic/pathological/microbiological findings, and TB/NTM exposure history of children with NTM lymphadenitis

All children experienced unilateral, non-tender cervicofacial lymphadenitis lasting longer than three weeks, showing no response to empirical antibiotics, including cefadroxil, cefradine, cefaclor, amoxicillin/clavulanic acid or ampicillin/sulbactam. None of the children had associated systemic symptoms, including fever, myalgia, fatigue, and weight loss. Violaceous skin discoloration was observed for seven patients and three patients experienced desquamation of overlying skin. Affected lymph nodes were located at submandibular region (n = 8), preauricular area (n = 6), and submental area (n = 1). Among the ten subjects, five were affected with two lymph nodes (Table 2).
Laboratory findings of NTM lymphadenitis
Tuberculin skin test was performed in six patients, where five had positive results with induration between 10–15 mm. Interferon gamma assay was done in nine patients in which eight were negative while one reported indeterminate in multiple tests (Table 2).
Ultrasonographic evaluation was done for eight patients, where none showed abscess formation, three showed perinodal fat swelling, two presented as cystic masses, and one had internal stippled calcification (Table 2).
Tissue samples were obtained from nine patients via incision and drainage (I&D), fine needle aspiration, or excisional biopsy and none showed the presence of bacteria under AFB smear and fungus under GMS/PAS staining. M. haemophilum was identified from two samples under AFB culture, both which were positive after 48–50 days of growth. Tuberculous (TB)-PCR was done on eight fresh tissue samples and all were negative. RT-PCR for MTB/NTM was done on all (n = 9) FFPE specimens. All samples were negative for MTB and two samples were positive for NTM (Table 2).
Among nine samples, after excluding one sample which was considered inadequate, histopathologic findings showed chronic granulomatous inflammation in all eight samples, of which three also showed caseous necrosis, four showed focal or diffuse necrosis, and one showed combined suppurative inflammation (Table 2).
Based on these findings, among all ten NTM lymphadenitis cases, four were classified as “confirmed”, four as “presumptive”, and two cases were classified as “suspected” NTM lymphadenitis.
Treatment of NTM lymphadenitis
Two patients underwent the combination of using anti-TB and anti-NTM medication and I&D (n = 2). Two subjects were given anti-NTM medication with I&D (n = 2). Anti-NTM medication included clarithromycin, ethambutol and rifampin. One patient was treated with oral clarithromycin and steroid injection by a dermatologist (n = 1). Others underwent I&D (n = 1) and excision (n = 1) only without oral medication. Two patients were followed up under close observation (n = 2) where one patient showed spontaneous regression and one patient was lost for follow-up. All the patients who visited the follow-up clinic have experienced completely resolved state of lymphadenopathy regardless of the type of treatment they received.
Potential exposure of NTM
Interviews and questionnaires revealed that three patients had been exposed to TB in the past; two during their infancy and one subject was exposed to TB two years in advance of NTM lymphadenitis. Although one patient reported to have recent exposure to a family member with pulmonary NTM, none of the patients acknowledged any exposure to persons with suspicious NTM lymphadenitis. All subjects reported to be enrolled in various daily indoor and outdoor activities, such as visiting farms, exposure to pets, playing in sand, and going on a travel with no common exposure points. Among the 5 cases with animal exposure, 2 cases had dogs and 3 cases reported to have fish in an aquarium in the home. None of the patients had recent exposure to cats or any scratches from animals. Utilization of public facilities was also questioned which showed similarities in various activities because more than half had experience of visiting swimming pools, beauty salon, oriental/physical therapy clinics, and dentistry. Among these activities, there was no common exposure site, although all ten patients have visited the same local sports complex in advance to disease onset (Table 3). However, environmental sampling was unavailable, making it impossible to identify an actual source for infection.
Table 3
Interview results for potential sources of NTM exposure

DISCUSSION
NTM lymphadenitis is a rare entity, however incidence is increasing worldwide partially due to enhanced accuracy in detection.1 In this study, we report a cluster of ten NTM lymphadenitis cases that were diagnosed and treated at a single tertiary hospital within a relatively short time period. Nine patients occurred during November of 2016 to April of 2014 and one more patient was added in April of 2018. All cases were previously healthy children without underlying diseases and had documented history of BCG vaccination.
NTM infection is suspected to be acquired from environmental exposures however, commonly the specific source cannot be identified. In this study, interestingly all the patients were found to have used the same local sports complex. Thus, exposure in the sports complex could be considered as a suspicious common source of infection. However, environmental sampling was unavailable, making it impossible to identify an actual source for infection.
Recently there have been reports of increase in NTM infections in Korea, however the majority were due to pulmonary disease and the number of extrapulmonary NTM disease were reported to remain unchanged.89 Due to the rarity of NTM lymphadenitis in Korea, we encountered numerous obstacles during the diagnostic process in both clinical and laboratory fields. Patients were all previously healthy and its low incidence among immunocompetent children led to a delayed recognition of NTM lymphadenitis as a potential differential diagnosis. Additionally, the atypical age presentation of the patients, who were between eight and fifteen years old, made it more difficult to suggest the possibility of NTM lymphadenitis, which is known to mostly affect children under the age of five. However, reports have shown that among patients with NTM lymphadenitis, cases due to M. haemophilum tended to be older than patients compared with M. avium.610 Cohen et al.10 reported that 23% (9/39) of children infected with M. haemophilum were > 7 years whereas all children infected with MAC were younger than 7 years of age.
Whether BCG vaccination protects against NTM infections has been controversial. However recently, a systemic review and meta-analysis showed evidence from large European surveillance studies that BCG vaccination protects against NTM lymphadenitis in children.11 Reports showed increase in NTM infection in children under 5 years of age after stopping universal neonatal BCG vaccination in various countries including Czech Republic, Sweden and Finland.12131415 In Sweden and Finland where information of strains was reported, the most common strains were MAC or M. avium.1215 The effectiveness may vary between NTM diseases and species, age groups and BCG strain, however data from various countries show that there is an effect on the incidence of NTM infection in children.11 Interestingly, all children in this study were previously vaccinated with BCG, over 5 years of age and in cases where the organism was identified, M. haemophilum was identified as a causative organism. These might be reasons to which these cases were able to develop lymphadenitis.
There were obstacles in diagnostic procedures also. Orders were initially placed from different departments including pediatrics, dermatology, otorhinolaryngology, and orthopedics. Sampling done by gun biopsy acquired a small amount of tissue thus leading to low yield in AFB culture and in initial cases where NTM was not suspected, specimen obtainment (formalin-fixed specimens) or culture conditions limited chances for NTM recovery.3 Of four confirmed cases, M. haemophilum was identified as a causative organism from two cases by culture while other two cases showed PCR positive. The fact that M. haemophilum was identified only from the samples acquired through I&D or excision also suggests the importance of acquiring adequate amount of tissue to achieve higher NTM recovery yield. In addition, the innate traits of M. haemophilium posed difficulties in its laboratory confirmation. The slow-growing, fastidious NTM preferentially grows at 30°C to 32°C only on media supplemented with iron-containing compounds such as ferric ammonium citrate, hemin or hemoglobin.16 In situations of suspicion, samples need optimal growth conditions along with prolonged duration of culture. Samples with culture positive for M. haemophilum reported growth after 48 days of culture. Even under optimal conditions only 50% to 82% yield positive cultures.3
In this study, we presented ten clustered cases of NTM lymphadenitis. There were obstacles in diagnosis due to its rare incidence in Korea, the atypical age of presentation and fastidious growth conditions of the pathogen. Considering the increasing incidence worldwide, especially among children and adolescents, clinicians should consider NTM as an important cause for subacute or chronic lymphadenitis even in countries with programs with universal BCG vaccination. Further studies on the epidemiology and clinical features of NTM lymphadenitis in children are needed and its optimal management guideline should be developed accordingly.
 XML Download
XML Download