

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bullying is an aggressive behavior that is repetitive and intentional in which a power differential exists between the victim and bully.1 Since there have been reports of suicides caused by school bullying in the mid-80s, various studies have been conducted to investigate the impact of peer bullying on the mental health of children and adolescents.2 Previous studies suggest that peer bullying is very common, with 10%–30% of children being bullied.34 Bullying is considered a major public concern in many countries because it may be associated with a broad spectrum of adverse outcomes for the victims. Being a victim of bullying has been reported to increase the risk of anxiety, depression, psychosomatic symptoms, substance use, and suicide attempts.56789 Moreover, the negative effects on mental health can last into adulthood. Bullied children have an increased risk for depression, anxiety, psychotic experience, and suicidality even after they become adults.1011 However, most studies have focused on the negative outcomes of peer victimization based on symptoms (i.e., anxiety) rather than diagnoses (i.e., specific phobia); hence, information about the impact of childhood bullying experience on specific psychiatric diagnosis is limited. There are a number of distinct types of anxiety disorders in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) (panic disorder, post-traumatic stress disorder [PTSD], social phobia, etc.), which have different clinical features, pathophysiologies, prognoses, and therapeutic strategies. To understand the effect of childhood bullying on adulthood psychiatric outcomes, it is essential to investigate the psychiatric outcomes based on separate diagnoses. Nevertheless, only a few studies have attempted to examine the association between childhood bullying and adulthood mental problems based on the DSM criteria, and they reported inconsistent findings for specific disorders.1213 In addition, most epidemiological studies on peer bullying have been conducted in Western countries, thus increasing the need to examine this issue in areas with different sociocultural backgrounds.14
In this study, we investigated the association of childhood experience of peer bullying with psychiatric disorders and suicidality in adults using data from the 2016 Korean Epidemiologic Catchment Area study (KECA-2016). We also determined whether a dose-effect relationship exists (more frequent peer bullying results in greater detrimental outcomes in adulthood).
METHODS
Participants
The KECA-2016, a nationally representative survey on psychiatric disorders in Korea, was carried out from April 2016 to November 2016. We used a multistage area sampling design and drew the sample from respondents to the 2010 population census of the community registry office in Korea. First, we stratified Korea into 16 large divisions in consideration of administrative districts and sociocultural differences. A total of 21 catchment areas based on municipalities (Si/Gun/Gu in Korean) were selected according to the population size of each division and accessibility to research centers, which comprised the primary sampling units (PSUs). Second, a sample of administrative regions (Eup/Myeon/Dong in Korean) was selected from the PSUs with probability proportional to size, representing the secondary sampling units (SSUs). Third, tertiary sampling units (TSUs) were created according to census tracts used in the 2010 population census. Overall, 2–22 TSUs were selected from each SSU with probability proportional to size, resulting in a sample of 645 TSUs. Fourth, each TSU was divided into chunks, with each sampling unit consisting of 24 households. Two chunks were randomly selected from each TSU, representing the quaternary sampling units (QSUs). Finally, a segment composed of four households was selected from each chunk by systematic sampling methods, representing the ultimate sampling units (USUs). By using the last-birthday method, one person per household was selected and interviewed. The sample size required for the present study was determined based on the prevalence rates of major psychiatric disorders reported in the 2011 KECA study15; enrollment continued until the target sample size was achieved (n = 5,100). A total of 5,102 respondents aged 18 or over completed face-to-face interviews.
Assessment of sociodemographic variables
We collected data on the following sociodemographic variables via interview: age (18–29; 30–44; 45–59; 60 or more years), gender, years of education (less than 10; 10–12; more than 12 years), area of residence (urban/rural), marital status (married/never married/separated, divorced, or widowed), and employment status (full-time job/part-time job/unemployed).
Assessment of experience of being bullied
We evaluated peer bullying using an item in the Adverse Childhood Experiences International Questionnaire (ACE-IQ).16 Participants were asked the following question about their experience of peer bullying: “The next question is about being bullied when you were growing up. Bullying is when a young person or group of young people say or do bad and unpleasant things to another young person. It is also bullying when a young person is teased a lot in an unpleasant way or when a young person is left out of things on purpose. It is not bullying when two young people of about the same strength or power argue or fight or when teasing is done in a friendly and fun way. When you were growing up, during the first 18 years of your life, how often were you bullied?” The participants could choose one of four answers: none, once, a few times, or many times. We considered respondents who chose “once,” “a few times,” or “many times” to have experienced peer bullying when they were growing up. To assess the effect of the frequency of bullying on the odds ratios (ORs) for adult psychiatric disorders and suicidality, we grouped respondents who answered “once” or “a few times” together under the category of “occasional victimization” and we classified those who answered “many times” under the category of “frequent victimization.”
Assessment of psychiatric disorders
The diagnostic interview used in the KECA-2016 was the Korean version of the Composite International Diagnostic Interview 2.1 (K-CIDI).17 Diagnoses were categorized according to the DSM-IV. The CIDI 2.1 was translated into Korean using the World Health Organization (WHO) guidelines. The validity and reliability of the K-CIDI has been shown to be high.18 In this study, we assessed 19 types of diagnoses and grouped them into five categories according to the DSM-IV classification system; the diagnoses included alcohol use disorders (alcohol abuse and alcohol dependence), nicotine use disorders (nicotine dependence and nicotine withdrawal), mood disorders (major depressive disorder, dysthymic disorder, and bipolar disorder), anxiety disorders (obsessive-compulsive disorder [OCD], PTSD, panic disorder, agoraphobia, social phobia, specific phobia, and generalized anxiety disorder [GAD]), and psychotic disorders (schizophrenia, schizoaffective disorder, schizophreniform disorder, delusional disorder, and brief psychotic disorder). In the analyses of the effects of frequency of peer bullying on the ORs for adult psychiatric disorders, we used five categories instead of individual psychiatric disorders because the number of participants diagnosed with each disorder was too small for the analyses. The lifetime prevalence of these disorders was assessed by trained interviewers. To exclude cases in which the onset of the psychiatric disorders preceded the time when bullying occurred, we considered only cases in which the age of onset was 18 or over in the assessment of adulthood prevalence. Therefore, we could assume that the childhood experience of being bullied preceded the onset of psychiatric disorders in adulthood.
Assessment of suicidality
We assessed lifetime suicidal behavior using the modified Suicide Prevention Multisite Intervention Study on Suicidal Behaviors, which was developed by the WHO.19 Three main questions were asked to evaluate suicidality: 1) “Have you ever seriously thought about committing suicide?” (lifetime suicidal ideation); 2) “Have you ever made a plan for committing suicide?” (lifetime suicide plan); 3) “Have you ever attempted suicide?” (lifetime suicide attempt).
To assume that the childhood experience of being bullied preceded the onset of suicidality in adulthood, we excluded cases in which the onset of suicidality preceded the time when bullying occurred. As a result, only cases in which the age of onset was 18 or over were considered.
Statistical analysis
Each respondent in the sample was given a sampling weight proportional to the portion of the national population with respect to age and gender as defined by the 2015 census of the Korean National Statistical Office. To determine the ORs and 95% confidence intervals (CIs), logistic regression analyses were performed using DSM-IV psychiatric disorders and suicidality as the main outcome variables and the experience of peer bullying (victims) as the principal predictor with no experience of peer bullying (non-victims) as the reference group. ORs were adjusted for gender, age, marital status, educational attainment, employment status, and area of residence. For suicidality, we performed additional analyses with adjustments for gender, age, educational attainment, marital status, employment status, area of residence, nicotine use disorders, alcohol use disorders, mood disorders, anxiety disorders, and psychotic disorders. The co-linearity between independent variables was evaluated by calculating the variance inflation factor (VIF). The goodness-of-fit was evaluated by the Hosmer–Lemeshow test. Statistical analyses were performed using IBM SPSS Statistics for Windows (Version 18.0; Armonk, NY, USA). Statistical significance was based on two-sided design-based tests evaluated at the 0.05 level of significance.
RESULTS
Descriptive statistics
This sample consisted of 4,986 KECA-2016 respondents (from 5,102 possible respondents) who provided data on the experience of peer bullying. Demographic characteristics are presented in Table 1. About 8.8% of the general population in Korea reported the experience of being bullied at least once when growing up. The proportion of being bullied was similar between men and women. However, reports of peer bullying were lower for those aged 60 years or older than for those aged 18–29 years (3.8% and 17.2%, respectively). Younger age, higher educational attainment, urban residence, and non-marriage were associated with increased OR for the experience of being bullied in the univariate logistic regression analysis. However, only younger age was associated with increased OR for the experience of being bullied in the multivariate logistic regression analysis.
Table 1
Association between sociodemographic factors and experience of peer bullying (n = 4,986)
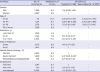
OR = odds ratio, CI = confidence interval.
aAdjusted for other variables in multiple logistic regression analysis with a backward stepwise method. The cut-off point of entry (PIN) was set at 0.05, and the cut-off point of exclusion (POUT) was set at 0.10. This model showed no significance in the Hosmer–Lemeshow goodness-of-fit test; bP < 0.001; cP < 0.01.
![]()
Association of the experience of being bullied with psychiatric disorders in adults
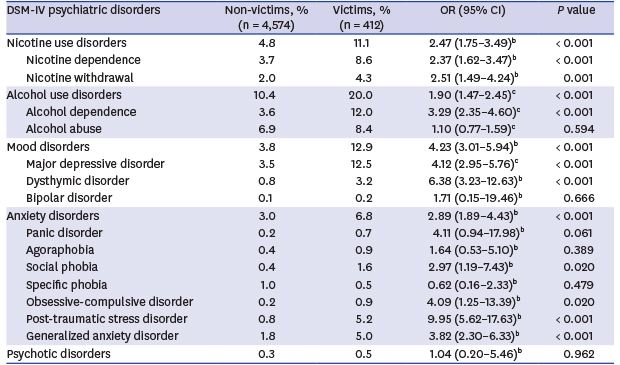
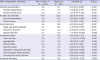
The adulthood prevalence and ORs of DSM-IV psychiatric disorders are shown in Table 2. The experience of being bullied was associated with an increase in the adulthood prevalence of nicotine use disorders (adjusted OR [aOR], 2.47; 95% CI, 1.75–3.49), alcohol use disorders (aOR, 1.93; 95% CI, 1.49–2.51), mood disorders (aOR, 4.23; 95% CI, 3.01–5.94), and anxiety disorders (aOR, 2.89; 95% CI, 1.89–4.43) after adjusting for gender, age, marital status, educational attainment, area of residence, and employment status. Among anxiety disorders, the OR for PTSD (aOR, 9.95; 95% CI, 5.62–17.63) was notably high. The effects of frequency of peer bullying on the ORs for DSM-IV psychiatric disorders are shown in Table 3. A dose-effect pattern was observed for nicotine use disorders, mood disorders, and anxiety disorders; however, it was not apparent for alcohol use disorders.
Table 2
Prevalence and odds ratios of adult psychiatric disorders in victims of peer bullying compared with non-victimsa
DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, fourth edition, OR = odds ratio, CI = confidence interval.
aOnly cases in which the age of onset was 18 or over were considered; bAdjusted for age, gender, education years, area of residence, marital status, and employment status. All models showed no significance in the Hosmer-Lemeshow goodness-of-fit test; cAdjusted for age. The models adjusted for sociodemographic variables showed significance in the Hosmer-Lemeshow goodness-of-fit test. Therefore, adjustments were made only for age, which was the only sociodemographic variable that showed a significant association with peer bullying in the multivariate analysis (Table 1). These models showed no significance in the Hosmer–Lemeshow goodness-of-fit test. The magnitudes of the results were similar between the two models.
![]()
Table 3
Effect of frequency of peer bullying on odds ratios for adult psychiatric disordersa

DSM-IV = Diagnostic and Statistical Manual of Mental Disorders, fourth edition, OR = odds ratio, CI = confidence interval.
aOnly cases in which the age of onset was 18 or over were considered; bAdjusted for age, gender, education years, area of residence, marital status, and employment status. All models showed no significance in the Hosmer-Lemeshow goodness-of-fit test; cAdjusted for age. The models adjusted for sociodemographic variables showed significance in the Hosmer-Lemeshow goodness-of-fit test. Therefore, adjustments were made only for age, which was the only sociodemographic variable that showed a significant association with peer bullying in the multivariate analysis (Table 1). These models showed no significance in the Hosmer–Lemeshow goodness-of-fit test. The magnitudes of the results were similar between the two models; dNo cases of psychotic disorders in the frequent victimization group.
![]()
Association of the experience of being bullied with suicidality in adults
The ORs for suicidality in victims of peer bullying are shown in Table 4. The experience of being bullied was associated with an increase in suicidal ideations (aOR, 2.07; 95% CI, 1.58–2.72), suicide plans (aOR, 3.92; 95% CI, 2.44–6.30), and suicide attempts (aOR, 4.19; 95% CI, 2.47–7.10) after adjusting for sociodemographic variables. A dose-effect pattern was also observed for suicidal behaviors. Frequent victimization was associated with larger ORs than occasional victimization. When adjusted for sociodemographic variables and psychiatric disorders, the relationship of childhood victimization with suicide plans (aOR, 2.07; 95% CI, 1.21–3.54) and suicide attempts (aOR, 2.02; 95% CI, 1.10–3.69) remained significant; however, the OR was decreased. When analyses based on the frequency of victimization were performed, frequent victimization was significantly associated with suicidality even after adjusting for sociodemographic variables and psychiatric disorders, whereas occasional victimization did not show significant results. There was no co-linearity between the independent variables in any of the analyses (VIF ≤ 2).
Table 4
OR for suicidality in victims of peer bullying compared with non-victimsa
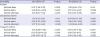
OR = odds ratio, CI = confidence interval.
aOnly cases in which the age of onset was 18 or over were considered; bAdjusted for age, gender, education years, area of residence, marital status, and employment status. All models showed no significance in the Hosmer-Lemeshow goodness-of-fit test; cAdjusted for age, gender, education years, area of residence, marital status, employment status, nicotine use disorders, alcohol use disorders, mood disorders, anxiety disorders, and psychotic disorders. All models showed no significance in the Hosmer-Lemeshow goodness-of-fit test.
![]()
DISCUSSION
In this study, we investigated the association of childhood experience of peer bullying with DSM-IV psychiatric disorders and suicidality in adulthood. The experience of being bullied in childhood was associated with an increase in adult psychiatric disorders, including nicotine use disorders, alcohol use disorders, mood disorders, anxiety disorders, and suicidality. In particular, the ORs for PTSD in adulthood were markedly high. Serious suicidal behaviors (i.e., suicide attempts) were associated with larger ORs, which demonstrated the high risk for serious suicidal behaviors such as suicide attempts in victims of peer bullying. A dose-effect pattern was evident for most psychiatric disorders except alcohol use disorders.
Reports of being bullied were the highest (17.2%) in the young age group (18–29 years) and lowest (3.8%) in the elderly group (60 or over). This declining trend with increasing age was also reported in a previous study.20 Recall bias may have played an important role; however, we considered the involvement of some other factors. For several decades, the competition among Korean students to obtain better grades and study at a higher ranking university has become more intense.21 In this stressful environment, the focus on academic performance may have affected the school climate negatively and lowered the self-esteem of many students, which could have resulted in increased bullying among students.22 Furthermore, the differences in mean education years between the age cohort groups may have also influenced the results. The mean number of years of education of the elderly group (8.8) was much smaller than those of other age cohort groups (14.4 for 18–29 years old, 14.8 for 30–44 years old, and 13.2 for 45–59 years old) because many elderly Koreans did not have educational opportunities in the period after the Korean War (1950–1953). This deprivation of education may have limited their exposure to peer bullying in school.
We found an association between childhood experience of peer bullying and most DSM-IV psychiatric disorders; however, some disorders did not show a significant association. The experience of being bullied was associated with an increased adulthood prevalence of nicotine use disorders. Similarly, a previous study reported that victims of peer bullying in childhood showed higher ORs for regular smoking compared with subjects not involved in bullying.23 In a Finnish study, being victimized at the age of 8 predicted daily heavy smoking at the age of 18; however, this study included only men.24
In this study, participants with childhood bullying experience showed higher ORs for alcohol dependence. A study has reported that adverse childhood experiences could increase the risk of heavy drinking and self-reported alcoholism.25 However, in some studies, there was no significant association between bullying victimization and adult alcohol dependence.1012 This discrepancy may be attributed to differences in the study populations, assessment methods, and prevalence of the disorders across countries. Therefore, further investigation may be necessary.
With respect to mood disorders, childhood victimization was strongly associated with major depressive disorder and dysthymic disorder. Since Olweus first reported that childhood bullying victims would have a higher risk of depression as young adults,1 there have been various studies supporting the observation.2627 Several hypotheses have been proposed to explain the association between childhood victimization and adulthood depression. Peer victimization may contribute to the development of cognitive vulnerability to depression.2829 In addition, hypothalamic-pituitary-adrenal (HPA) axis abnormality, specifically blunted cortisol reactivity, has been reported among bullied children.30 Genetic variability in the serotonin transporter (5-HTT) gene has been suggested to moderate the risk of emotional disturbance after the experience of being bullied.31
Previous studies have consistently reported that childhood victimization could increase the prevalence of aggregate anxiety disorders in adulthood,5101213 which was observed in this study. However, there is limited information on the association of specific anxiety disorders with childhood peer bullying. We found a significant association between the experience of being bullied and social phobia, OCD, PTSD, and GAD. For panic disorder, agoraphobia, and specific phobia, the proportions of each disorder seemed different between victims and non-victims; however, statistical analysis did not show any significance. Previously, a study reported increased risks for GAD, panic disorder, and agoraphobia in victims of peer bullying.12 Another study showed a linear relationship between peer victimization frequency and the risk for each of the anxiety disorders in adulthood (GAD, social phobia, specific phobia, panic disorder, and agoraphobia).13 One of the reasons we did not observe a significant association for panic disorder, agoraphobia, and specific phobia might be type II errors due to the small sample size of each disorder in the study. However, considering that some anxiety disorders (i.e., agoraphobia and specific phobia) seem to be more innate and do not arise directly from environmental experiences,32 it is possible that certain anxiety disorders have a weaker or no association with childhood peer bullying. A more in-depth study will be needed to clarify this issue.
Notably, the OR for PTSD in victims of peer bullying was the largest compared with the ORs for other DSM-IV psychiatric disorders. Several mechanisms may explain this association. From the biological perspective, early life experience has been shown to lead to long-term effects on HPA axis reactivity, which can be a predisposing factor for PTSD development in adulthood.33 From the perspective of cognitive vulnerability, the experience of peer bullying can develop or fortify cognitive biases, including negative thoughts about one’s self, the world, and others, contributing to the development of PTSD in adulthood.34
A study has reported that adolescents who experience more undesirable life events could have a higher risk for developing OCD.35 In addition, a significant association has been found between traumatic experience and the development of OCD in the general population.3637
In agreement with previous studies,1038 we observed a dose-effect pattern showing that children who experienced frequent bullying were more likely to suffer from adult psychiatric disorders. If we could identify and intervene in the events of peer bullying in earlier stages, we would be able to lower the risk of psychiatric disorders and suicidality.
The experience of childhood bullying was associated with all types of suicidality in adulthood (suicidal ideas, suicide plans, and suicide attempts). The ORs tended to be larger for more serious suicide-related behaviors (e.g., the OR for suicide planning was larger than that for suicidal ideas), which were more robust for more frequent bullying. Therefore, the experience of victimization is a highly specific risk factor for serious suicidal behaviors such as suicide attempts. After we adjusted for psychiatric disorders in adulthood, childhood bullying experience was associated with a two-fold increase in the OR for suicide plans or suicide attempts in adulthood. Frequent victimization showed a more robust relationship with adulthood suicidality, highlighting the importance of the early detection and management of bullying in childhood.
The strengths of this study include the following: 1) the nationally representative large sample; 2) the use of a structured diagnostic interview for psychiatric diagnoses; 3) the examination of the association of victimization with specific DSM-IV psychiatric disorders, which have rarely been reported in previous studies; 4) participants with a non-Western sociocultural background.
There are several limitations in this study. First, this was a cross-sectional study; thus, a causal relationship between childhood experience of bullying and psychiatric outcome in adulthood could not be explored. Second, information on the experience of peer bullying was gathered only from the participants. Although self-report has been suggested to be the most sensitive and reliable method for assessing victimization,39 recall bias or response bias could have influenced the results. For example, more depressive or anxious individuals might view their childhood experience more negatively and respond more affirmatively to the question about the experience of peer bullying. Furthermore, some people might have forgotten about their childhood experience over the years. The low number of reports of peer bullying in the elderly group reflect this tendency. Although age was adjusted for in the analyses, we should be cautious when interpreting the results. To minimize these types of biases, a longitudinal cohort study with multiple sources of information (e.g., children, parents, and teachers) is required. Third, we could not control for childhood psychiatric problems or detailed familial background because we did not gather the relevant data.
In conclusion, childhood experience of bullying was associated with adult psychiatric disorders and suicidality. The strong dose-effect relationship indicated the importance of the early detection and intervention of childhood peer bullying to decrease detrimental consequences in adulthood. This study may provide valuable information for clinicians to manage victims of peer bullying and for policymakers to implement health and education programs.
 XML Download
XML Download