

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Infants and young children are most susceptible to influenza because they have not yet been exposed to vaccination or natural infection. Children younger than 5 years of age have the highest rates of laboratory-confirmed influenza and a high risk for influenza complications during seasonal influenza epidemics.1 Vaccination is the best available preventive measure against influenza infection. However, it is more challenging for infants and young children than the other age groups to achieve proper protection with the influenza vaccine because of lower immunogenicity and short-lasting immunity due to their immature immune system or insufficient immunological priming by previous vaccination.23 In the United States, seasonal influenza vaccinations are recommended as soon as possible after it is available in their community, preferably by the end of October. Vaccine can be offered until the end of the influenza season.45 In Korea, influenza vaccine is recommended for immunization by the end of October and early November.6 The peak epidemic of influenza virus is from January to March, but it is actually thought to be the influenza season for six months from December to May.7 Children are expected to continue protective immunity during the epidemic period after influenza vaccination89 If the protective antibody response induced by influenza vaccination at this age disappears sooner than the anticipated viral epidemic period, adjustment of the vaccination time is required for effective prevention during the entire influenza season.101112 In order to maximize the prevention effect of influenza vaccination, the duration of protective immunity should be able to cover the peak epidemic period of influenza virus. In this study, we measured the antibody titers at 6 months after influenza vaccination by analyzing the seroprotection rate and geometric mean titer (GMT) in Korean children aged 6 to 35 months. We compared the persistent antibodies between a full dose (0.5 mL) quadrivalent influenza vaccine (QIV) and a half dose (0.25 mL) trivalent influenza vaccine containing the B-Victoria strain (TIV-Vic). We aimed to suggest a proper vaccination strategy to maintain adequate protective immunity throughout the influenza season in young children.
METHODS
Study design
This was a study of a randomized, double-blinded, multi-center trial to assess the long-term immunity of a full dose QIV and a half dose TIV-Vic in healthy children, aged 6–35 months. This study was conducted between September 2016 and July 2017 at 10 hospitals in Korea. Using a randomization table, participants were randomly assigned to be vaccinated with either full dose of QIV or a half dose of TIV-Vic.
Participants
The study included 124 healthy children aged 6–35 months who had not been previously vaccinated for the current influenza season (2016–2017). The exclusion criteria were participants who had chronic medical diseases, including immunodeficiency disorder, acute febrile illness; were treated with immunosuppressive agents and corticosteroids; or were contraindicated to influenza vaccine. Children who received the influenza vaccine for the first time or who had received only one dose of vaccine in the previous season were administered two doses with a four-week interval in accordance with the Korean Advisory Committee on Immunization Practices guidelines.6 At 6 months after the final dose of vaccine was administered, blood samples were obtained, centrifuged, and stored at −70°C until the hemagglutination-inhibition (HI) test. Influenza infection was assessed from enrollment to blood sampling, which was approximately for 6 months. The enrollees had been encouraged to visit our clinic for rapid antigen test and reverse transcription polymerase chain reaction (RT-PCR) when they had an influenza illness.
Vaccination
Children were vaccinated with either a Madin-Darby Canine Kidney cell culture-derived quadrivalent inactivated subunit influenza vaccine (SKYCellflu4®; SK Chemicals, Seongnam, Korea) or a trivalent inactivated subunit influenza vaccine (SK influenza trivaccine®; SK Chemicals). A full dose (0.5 mL) QIV or a half dose (0.25 mL) of TIV was administered to the enrollees, both of which were loaded into pre-filled syringes. A full dose QIV contained 15 µg hemagglutinin per strain, and a half dose TIV contained 7.5 µg hemagglutinin per strain. The 2016-2017 TIV included A/California/7/2009 (H1N1) pdm09, A/Hong Kong/4801/2014 (H3N2), and B/Brisbane/60/2008 (B/Victoria lineage) and the QIV included additionally B/Phuket/3073/2013 (B/Yamagata lineage), in accordance with the WHO recommendation for the composition of the northern hemisphere 2016–2017 influenza vaccine.13
Immunity assessment
HI antibody titers were measured for each hemagglutinin of the A/H1N1, A/H3N2, B/Yamagata and B/Victoria strains contained in the vaccine using standard assays with cell-derived hemagglutination antigens and turkey erythrocytes. The lower limit of HI antibody titers was assigned a value of 1:5 that was below the lowest dilution (1:10), and the upper limit was set as the highest dilution (1:10, 240) used in the assay. Samples were titrated to determine absolute endpoint titers. The seroprotection rate was defined as the proportion of individuals with antibody titers of 1:40 or more according to the HI assay. The GMT was calculated with 95% confidence intervals (CIs).
Statistical analysis
To compare the seroprotection rates between the two groups (vaccine types and number of shots), a χ2 test was used. GMTs and their 95% CIs were calculated as the anti-log of the mean and 95% of the log10 values. P values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS for Windows ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic characteristics
A total of 124 participants were enrolled from September to December 2016. Participants were randomly assigned in QIV (n = 81; 65.3%) or TIV-Vic (n = 43; 34.7%) groups. Forty-one participants (33.1%) had unprimed status of influenza immunization and were vaccinated twice at intervals of 4 weeks. The mean age at first dose of vaccination was 24.8 ± 7.4 months old and the proportion of boys was 49.2% (n = 61). There was no significant difference in age and sex between QIV and TIV-Vic groups. During the study period, 13 participants (10.5%) were diagnosed with influenza infection. (Fig. 1 and Table 1).
Fig. 1
Flow chart of the study.
QIV = quadrivalent influenza vaccine, TIV = trivalent influenza vaccine.

Table 1
Demographic characteristics of enrolled individuals
Immunity at 6 months after vaccination in all participants, excluding those with influenza infection
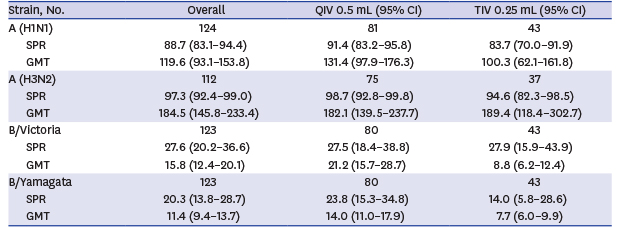
The seroprotection rates were 88.7% for influenza A (H1N1), 97.3% for influenza A (H3N2), 27.6% for influenza B/Victoria lineage and 20.3% for influenza B/Yamagata lineage. Their GMTs were 119.6 (95% CI, 93.1–153.8) for influenza A (H1N1), 184.5 (95% CI, 145.8–233.4) for influenza A (H3N2), 27.6 (95% CI, 20.2–36.6) for influenza B/Victoria lineage and 20.3 (95% CI, 13.8–28.7) for influenza B/Yamagata lineage (Table 2). The seroprotection rates and the GMTs at 6 months post vaccination were higher against the influenza A strains than against the influenza B strains.
Table 2
Comparison of post-vaccination immunity after 6 months between a full dose of quadrivalent influenza vaccine and a half dose of trivalent influenza vaccine, excluding naturally infected individuals

Comparison of immunity at 6 months after vaccination between QIV and TIV
Three common strains (A [H1N1], A [H3N2] and B [Victoria]) and one additional strain (B [Yamagata]) were included in the 2016–2017 recommended influenza QIV. The seroprotection rates for A (H1N1), A (H3N2), and B (Victoria) were 91.4%, 98.7% and 27.5% in a full dose of QIV vs. 83.7%, 94.6% and 27.9% in a half dose of TIV-Vic, respectively. The GMTs (95% CI) for A (H1N1), A (H3N2) and B (Victoria) were 131.4 (97.9–176.3), 182.1 (139.5–237.7) and 21.2 (15.7–28.7) in a full dose of QIV vs. 100.3 (62.1–161.8), 189.4 (118.4–302.7), 8.8 (6.2–12.4) in a half dose of TIV-Vic, respectively. Both groups shared three strains of antigen but differed in the amount of antigen inoculated. The seroprotection rate for additional B (Yamagata) was 23.8% and the GMT was 14.0 (11.0–17.9) in a full dose QIV versus 14.0% and 7.7 (6.0–9.9) in a half dose TIV-Vic, respectively. None of the results were statistically significant (Table 2).
Comparison of immunity at 6 months after vaccination according to the primed status
The seroprotection rate and the GMT were not significantly different according to the immunization status. In both the vaccine groups, the seroprotection rate and the GMT against influenza A strains were similar between the primed group and the unprimed group. The seroprotection rate and the GMT against the common B strain (Victoria) were higher in the unprimed group: 32.0% and 18.4 (10.9–31.2) in the unprimed group vs. 25.5% and 14.4 (10.0–19.7) in the primed group; with QIV vaccination: 40.0% and 31.7 (14.2–70.9) versus 21.4% and 11.9 (7.2–19.6) with TIV-Vic vaccination. The seroprotection rate and the GMT for the additional B strain (Yamagata) were higher in the primed group with QIV vaccination but similar with TIV-Vic vaccination: 25.5% and 12.9 (9.9–16.8) in the primed group vs. 20.0% and 13.6 (8.2–22.6) in the unprimed group with QIV vaccination; 14.3% and 9.5 (6.6–13.7) in the primed group vs. 13.3% and 7.6 (4.8–12.0) in the unprimed group with TIV-Vic vaccination (Table 3).
Table 3
Comparison of post-vaccination immunogenicity after 6 months between one shot and two shots, excluding naturally infected individuals
Influenza infection after vaccination
Laboratory-confirmed, symptomatic influenza virus infection was diagnosed in 13 patients (10.5%), including 12 infected with influenza A (H3N2) virus and 1 infected with influenza B virus. Their antibody titers were excluded from analysis of immunity at 6 months after vaccination.
The median age of influenza virus-infected participants was 20 (17–28) months old and the boys-to-girls ratio was 6:7. Influenza infections occurred in 7 cases among the QIV recipients and 6 cases among the TIV recipients. Among the 13, 5 were unprimed (38.5%), who were administered the vaccine drug twice with a 4-week interval. Ten of the infected participants were administered their last dose of vaccination in November and 3 in December. Infection occurred mostly in December and January. Only one case was diagnosed with influenza infection with B strain in March. The median time interval from the last vaccination dose to diagnosis of influenza infection was 47 (39–56) days (Table 4).
Table 4
Characteristics of influenza patients after vaccination
DISCUSSION
In this study, we found that the persistence of antibodies at 6 months was significantly lower against influenza B strains than A strains in infants and young children, which seemed to be insufficient to protect from influenza B infections during the late influenza season. Moreover, the young children who were primed with TIV showed a lack of immunogenicity against a different B strain.
Our results showed that HI antibody persistence at 6 months after vaccination varied according to influenza virus strains in children aged 6–35 months. Immunity was maintained at higher levels against influenza A (H1N1) and A (H3N2) than against both types of influenza B virus up to 6 months after vaccination. Immunity at 6 months after vaccination indirectly reflected the protection rate in late periods of the influenza season. The HI antibodies to both the influenza A subtypes—H1N1 and H3N2—were sustained at sufficiently high levels until the late influenza season, regardless of the vaccine type, antigenic dose, and the primed state. Although immunity against all four strains decreased over time,12 the HI antibody levels against B strains at 6 months were much lower and varied according to the vaccine type and the primed status. Our results did not include pre- and post-vaccination data, thus it may be difficult to discriminate whether antibody titers against influenza B were low even immediately after vaccination, or whether antibodies were fully produced but rapidly degraded. Previous studies have shown that immunity was lower against influenza B strains than against A strains.91014151617 Kang, et al.9 reported that the seroprotection rates at 1 month, 6 months, and 12 months after vaccination against influenza B were 65.8%, 26.5% and 10.0%, respectively, in 6–35-month-old children. Eun et al.18 reported that a half dose of QIV induced relative weaker immunogenicity against both B strains at one month after immunization in children aged 6 to 35 months: seroprotection rate at 1 month after immunization was 62.6% against B/Yamagata strain and 51.4% of B/Victoria strain. According their study, the seroprotection rate against influenza B strains were 62.6% (Yamagata) and 51.4% (Victoria), while the seroprotection rates against influenza A strains were 91.6% (H1N1) and 96.3% (H3N2). These results indicate the rapid decline in the antibody titers against B strains and are consistent with our results at 6 months after immunization. Thus, we may carefully conclude that waning of protection against influenza B strain was rapid in infants and toddlers.
At 6 months after the last dose of vaccine, HI titers against the three common strains in both vaccines (A [H1N1], A [H3N2] and B [Victoria]) was not different between QIV and TIV-Vic groups, although a full dose antigen was administered in the QIV group. The unprimed children younger than 3 years old elicit a diminished immune response compared with the older children.3 Several previous studies that compared the immunity between a full dose vs. a half dose of influenza vaccine in young children had inconsistent results.192021 In this study, persistence of antibodies to influenza virus at 6 months showed no difference according to injected antigenic dose against the three shared strains in both vaccines. In contrast, persistence of antibodies at 6 months against the additional B (Yamagata) strain was relatively more preserved in the QIV group than in the TIV-Vic group. Previous studies have reported QIV induced superior antibody titers for the added B lineage strain and non-inferior titers for all the shared strains in children aged 6–35 months.2223 These results suggest that QIV for young children was advantageous not only for children with naive state but also for children who had been primed with another B lineage previously.
In comparison according to the primed state, HI antibody levels of all four strains were not statistically different. However, the primed group showed favorable tendency in the seroprotection rate and the GMT in A (H1N1), A (H3N2) and additional B (Yamagata) subtypes, regardless of vaccine type. However, B (Victoria) strain showed higher seroprotection rate and the GMT in the unprimed group. It is well-known that the primed children by previous vaccinations or natural influenza infection have better antibody response to the next influenza immunization.112425 This discordance may be caused by number of shots against Victoria. Ito et al.24 suggested that one B lineage could not prime the immune response to other B lineages. The antigenic difference between the two B lineage strains suggested that antibodies against the two lineages were monospecific and showed little heterotypic reactivity.26 Cross-protection between the two influenza B lineages was limited.27 A previous study proved that children primed with one lineage of B antigen showed less seroprotection to different B antigens.1428 Because the current immunization policy defined the group primed, irrespective of the previous covered B strain, the primed group may be unable to elicit proper immune responses against different B strains. TIVs for the 2015–2016 season included B (Yamagata lineage), and those for 2016–2017 included B (Victoria lineage). Considering that the B (Victoria) strain was not included in the 2015–2016 influenza vaccination, the primed group was actually not primed to the B (Victoria) strain. But they got only one shot because they were considered as primed. This would explain how the unprimed group with two shots had higher antibody response to Victoria strain.
Among our study population, 13 participants (10.5%) were diagnosed with natural influenza virus infection. There was no difference in the number of infected children between vaccine types. Five out of 13 (38%) infected individuals were from unprimed state. During the 2016–2017 influenza season in Korea, influenza A (H3N2) viruses predominated with co-circulation of influenza B viruses, according to a primary clinic-based sentinel surveillance conducted by the Korea Centers for Disease Control and Prevention.7 According to the Korea Influenza and Respiratory Viruses Surveillance System, peak influenza activity was determined at 86.2 out of 1,000 outpatient visits at week 52. Most of the detected influenza viruses were A (H3N2) strains until the end of February, followed by influenza B (both lineages) viruses from week 2 to week 25, 2017. A small peak of influenza B activity occurred at week 15, 2017.7 Noh et al.29 reported low vaccine effectiveness against A (H3N2) influenza in the 2016–2017 season due to amino acid substitutions in the hemagglutinin, in a Korean adult-based study. The vaccine effectiveness against A (H3N2) and B was reported at 34% and 56%, respectively, in the US during the 2016–2017 influenza season.30 In our study, the natural infection cases coincided with the epidemic trend in the 2016–2017 season. Most of them were infected with influenza A (H3N2) during the peak influenza season. Usually the epidemic trend of influenza in the northern hemisphere, including Korea, shows a major peak from the end of December to January caused mainly by influenza A strains, followed by a sporadic or small peak of influenza B strain epidemic in late spring. The prevalence of influenza B tends to start lately, hence it is necessary to maintain long term immunogenicity against B strains.
The strength of this study is that it was a prospective study that assessed waning of antibodies to influenza virus after 6 months of immunization in infants and toddlers. The study was conducted as a multi-institutional study throughout Korea. Considering that the participants in this research were in a vulnerable age group, we collected blood samples only once at 6 months after vaccination for minimizing invasive procedures. Therefore, there were no data for pre- and post-vaccination antibody titers in this study. The limitation of this study is that it was not possible to examine the serial declining tendency of the antibody titer.
In conclusion, persistent antibodies to influenza virus after 6 months of immunization was more favorable against influenza A strains than against B strains. Immunity of additional B strains at 6 months was superior in the QIV group. The higher dose was not effective for the persistence of antibodies against all the three shared strains. The immunity of the primed children with different B strains did not show superiority to that of the naive group with another B strain. Because young children are less likely to have had priming experience with influenza, the recent recommendation of priming was not effective on major changes in the influenza B lineage from year to year. Rapid waning immunity against B strains should be one of the important factors to decide the best timing of influenza vaccination. QIV can induce immunity against both B strains, so it seems to have advantage as priming vaccine, especially when genotype of B vaccine strain is changed in next seasons.
 XML Download
XML Download