

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The onset of temporomandibular joint (TMJ) ankylosis at early age can result in severe functional and esthetic problems, including limited mouth opening, mandibular retrusion, and facial asymmetry.123 In order to minimize these problems, TMJ ankylosis should be treated as soon as it is detected.4 Condylectomy, gap arthroplasty, interpositional arthroplasty, mandibular distraction osteogenesis (MDO), and TMJ reconstruction have been used as treatment modalities for TMJ ankylosis.
Although condylectomy and gap arthroplasty can result in pseudo-articulation, these procedures have some side effects such as anterior openbite in bilateral cases, premature contact on the affected side and openbite on the unaffected side in unilateral cases, and recurrent TMJ ankylosis.5 For prevention of re-ankylosis, interpositional arthroplasty has been performed using autogenous grafts (e.g., temporal muscle flap, dermis fat) or alloplastic materials (e.g., acrylic, silastic).6 However, gradual collapse of the gap by contraction forces from the masticatory muscles can also lead to recurrent TMJ ankylosis.6
MDO in conjunction with arthroplasty can transport the osteotomized bone toward the area of the glenoid fossa. The soft tissue between the transported segment and the glenoid fossa area can function as a new disc.789 However, it is controversial whether MDO can be performed simultaneously with arthroplasty.
Conventional TMJ reconstruction involves the surgical removal of ankylosed bone and replacement with an autogenous bone graft (e.g., costochondral, clavicular, or metatarsal bone). A costochondral graft offers advantages in terms of its morphological similarity with the condyle and capacity for regeneration and growth.3 However, this procedure has some limitations, including donor site morbidity, an unpredictable growth pattern, and re-ankylosis.10 If patients have a history of previous TMJ surgeries and recurrent TMJ ankylosis, TMJ reconstruction using an artificial prosthesis can be adopted as an alternative approach.111213
In order to understand the treatment flow for TMJ ankylosis, it is necessary to perform longitudinal followup for patients with recurrent ankylosis despite a series of conventional surgical treatments. Here we describe the longitudinal management of recurrent TMJ ankylosis in a young girl from infancy to adulthood in perspective of surgical and orthodontic treatment.
CASE REPORT
Patient
A 2-year-old infant girl visited the Department of Orthodontics, Seoul National University Dental Hospital, Seoul, South Korea. The patient exhibited a convex profile and a large overjet (5.0 mm) (Figure 1 and Table 1). The maximum mouth opening was 7 mm due to the bony ankylosis in both TMJs. Trauma during delivery or after birth was suspected to be the cause of ankylosis in this patient because there was no history of infection in the medical record.
Treatment
A three-stage approach was inevitably performed to resolve recurrent TMJ ankylosis and other skeletodental problems.
Stage I treatment during early childhood
Objectives and treatment plan
The objectives were as follows: (1) to remove the ankylosed part of TMJ and rehabilitate jaw function, and (2) to allow the chance of normal mandibular growth.
High condylectomy and interpositional arthroplasty were recommended to lower the risk of mandibular growth inhibition. And the patient's parents were informed of the possibility of re-ankylosis.
Treatment progress
Computed tomographic (CT) images and panoramic radiograph obtained before stage I treatment are presented in Figure 2. At 6 years and 3 months of age, the upper 3 to 5 mm of the condyle was removed, and the cut surface was given a round shape (Figure 2 and Table 2). Interpositional arthroplasty was performed by reshaping of the articular eminence and placement of the temporal musculofascial flap in the glenoid fossa (Figure 2 and Table 2).
Follow-up results
The mandible exhibited a downward and forward growth at one year after the stage I surgery (Figure 2). However, when the patient was 11 years and 10 months old, the maximum mouth opening decreased from 22 to 14 mm. In addition, she developed symptoms of obstructive sleep apnea (OSA; apnea-hypopnea index, 96.7; lowest oxygen saturation, 64%).
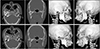
CT images exhibited mandibular retrusion, chin point deviation to the right side, recurrence of TMJ ankylosis, deepening of the antegonial notch, and elongation of the coronoid process (Figure 3).
Stage II treatment during early adolescence
Objectives and treatment plan
The objectives were as follows: (1) to remove the reankylosed portion of TMJ and increase the mouth opening, (2) to correct the mandibular retrusion and chin point deviation, (3) to establish normal occlusion, and (4) to restore the airway space.
Gap arthroplasty for the right TMJ and coronoidectomy of both sides were planned to remove the reankylosed portion and to increase the mouth opening, respectively. Bilateral MDO (BMDO) was planned to lengthen the mandibular body length and ramus height, correct the chin point deviation using differential distraction between the right and left sides, and increase the retroglossal airway volume.1415
Treatment progress
Gap arthroplasty and coronoidectomy were performed at the age of 11 years and 11 months according to the treatment plan (Figure 3 and Table 2). Six months later, when the patient was 12 years and 5 months old (hand-wrist radiograph: R-IJ growth stage, Figure 4),16 two extraoral unidirectional distractors (KLS Martin Corporation, Tuttlingen, Germany) were placed with a downward vector in the posterior mandibular body (Figure 5 and Table 2). The maxillary first premolars were extracted and a total of four miniplates were installed at the infrazygomatic crest area and the symphysis area on both sides (Figure 5). After a latency period of 5 days, active distraction at the rate of 1.0 mm/day was performed for 30 days on the right side and 19 days on the left side (Figure 5 and Table 2). During the distraction period, orthodontic treatment of the maxillary arch was started. When overcorrection of the mandibular dental midline was achieved, a two-month consolidation period was given. During the distraction and consolidation periods, Class III elastics (5/16 inch, 6 ounce) between the miniplates installed in the maxilla and mandible were used to mold the distracted bony segment and to minimize clockwise rotation of the mandible. At the time of removal of the distraction osteogenesis device, the mandibular first premolars were extracted and the orthodontic brackets were bonded on the mandibular arch. Post-BMDO orthodontic treatment was completed at the age of 14 years and 8 months (Figure 6 and Table 2).
Treatment outcomes
The treatment resulted in significant correction of the chin point deviation, an improvement in the facial profile, Class I canine and molar relationships, a normal overjet/overbite, and overcorrection of the mandibular dental midline (Figure 6 and Table 1). The maximum mouth opening increased from 14 to 33 mm.
Follow-up results
One year after post-BMDO debonding, slight bite opening was observed due to clockwise rotation of the mandible (Figure 7).
Five years after post-BMDO debonding, the maximum mouth opening decreased from 33 to 8 mm. CT images revealed re-ankylosis of both TMJs, particularly on the right side (Figure 8). Because the upper airway space was decreased (Figure 8), the patient had to use a continuous positive airway pressure device. In addition, the mandibular anterior teeth exhibited gingival recession caused by retraction forces from the labial frenum and muscles.
Stage III treatment after completion of growth
Despite a series of previous surgical interventions during stages I and II, re-ankylosis of the TMJs, skeletodental problems, and OSA symptoms were recurred at the age of 19 years and 4 months.
Objectives and treatment plans
The objectives were as follows: (1) to remove the reankylosed portion and increase the mouth opening; (2) to prevent the reankylosis; (3) to correct the mandibular retrusion and chin point deviation, (4) to establish normal occlusion, and (5) to restore the patency of the upper airway.
The three treatment options were suggested to the patient and her parents: (1) two-jaw surgery with counter- clockwise rotation for advancement of the maxillomandibular complex; (2) the same two-jaw surgery recommended in option 1 along with reconstruction of the bilateral TMJs using artificial prostheses; and (3) one-jaw surgery with counterclockwise rotational advancement of the mandible and reconstruction of the bilateral TMJs using artificial prostheses.
Treatment progress
As a preparatory surgery, low condylectomy on the right side and coronoidectomy on both sides were performed. As a result, the patient developed a severe Class II openbite with chin deviation to the right side (Figure 8 and Table 1).
During 8 months of pre-TMJ-reconstruction orthodontic treatment, the mandible slightly rotated counter-clockwise through physiologic repositioning (Figure 9). Reconstruction of the bilateral TMJs was performed using artificial prostheses (Biomet Microfixation TMJ replacement system, Warsaw, IN, USA): (1) Following Risdon and pre-auricular incision, the masseter and medial pterygoid muscles were reflected and the lateral surface of the ramus was contoured; (2) Once the fossa component of the artificial prosthesis was installed, the mandible was advanced with counterclockwise rotation using a surgical wafer; (3) Intermaxillary fixation was performed; (4) The mandibular component of the artificial prosthesis was fixed in the correct position; and (5) genioglossus advancement procedure was performed to pull the genioglossus/geniohyoid muscles forward for alleviation of the OSA symptoms. One month after surgery, post-TMJ-reconstruction orthodontic treatment was initiated and continued for three-and-half months (Table 2).
Treatment outcomes
The patient's facial profile exhibited a significant improvement and Class I canine and molar relationships were obtained along with a normal overjet/overbite (Figure 10 and Table 1). Fortunately, gingival recession in the mandibular anterior teeth area was not aggravated (Figure 10), and the patient refused to undergo gingival grafting. The maximum mouth opening increased from 14 to 38 mm.
Lateral cephalogram exhibited mandibular advancement by 18 mm at the pogonion and an increase in the ramus height by 5 mm (Figures 10, Table 1). Although the patient refused to undergo post-treatment polysomnography, her OSA symptoms relieved and the airway volume increased from 9.4 to 15.8 mL on the CT images (Figure 11).
Follow-up results
Class I canine and molar relationships and normal overbite/overjet were well maintained at the one-year follow-up visit (Figure 12).
This case report was reviewed and approved by the institutional review board at Seoul National University Dental Hospital (ERI18012). The patient gave us a written informed consent for publication of her data.
DISCUSSION
In the present report, the longitudinal management of recurrent TMJ ankylosis from infancy to adulthood via orthodontic and surgical approach was described (Figure 13, Table 2).
Functional and esthetic rehabilitation of patients with TMJ ankylosis is challenging because of technical difficulties and a high incidence of recurrence. Surgical skills and post-operative management including early mouth opening exercise, appropriate physiotherapy, and close follow-ups are important factors for achieving successful outcomes.47
Henry and Wolford11 evaluated patients who underwent multiple TMJ surgeries and reported a higher success rate with custom-made total joint prostheses than with various autogenous grafts (88% vs. 13–31%). Wolford et al.20 demonstrated adequate function of artificial TMJ prostheses during a follow-up period of 5 to 8 years. However, such prostheses are also associated with problems such as wear, mobility or fracture of the implant, hypersensitivity, a foreign body reaction, and heterotropic bone formation.1221
On the basis of the findings from this case, we would like to suggest a treatment flow-chart for the management of TMJ ankylosis according to the growth stage (Figure 14). Primarily, the flowchart shows that the treatment-involved area increases with the duration of ankylosis, patient's age, and degree of deformity.
First, when TMJ ankylosis is detected in early childhood, high condylectomy and interpositional arthroplasty are recommended to remove the ankylosed portion, to achieve functional rehabilitation, and to provide the opportunity for normal growth of the mandible.
Second, when TMJ ankylosis is detected or recurs in early adolescence, high or low condylectomy, interpositional or gap arthroplasty, coronoidectomy, or MDO and pre- and post-MDO orthodontic treatment are recommended to correct mandibular retrusion and/or facial asymmetry, to achieve Class I occlusion, and/or to relieve the OSA symptoms. Since the mandible is still growing at this stage, there is a possibility of aggravation of facial asymmetry and/or mandibular retrusion. Therefore, when progressive TMJ ankylotic change in adolescent patients cannot be arrested despite a series of surgical interventions, further surgical approaches including TMJ reconstruction using artificial prostheses should be delayed until completion of growth.
Finally, in adult patients, two-jaw or one-jaw surgery, TMJ reconstruction using artificial prostheses along with counterclockwise rotation of the maxillomandibular complex, genioglossus advancement procedure, and pre- and post-TMJ-reconstruction orthodontic treatment can be performed to exterminate the ankylosis, to correct mandibular retrusion and/or facial asymmetry, to achieve Class I occlusion, and/or to relieve the OSA symptoms.
The findings from this case suggest that it is necessary to consider the diverse factors of individual patients and meticulously observe the treatment outcomes and prognosis.
CONCLUSION
Since the treatment modalities for TMJ ankylosis differ according to the duration of ankylosis, patient age, and degree of deformity, the treatment flowchart suggested in this report could be used as an effective guideline for determining the appropriate timing and methods for the treatment of TMJ ankylosis.














 XML Download
XML Download