

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF), the most common cardiac dysrhythmia, causes substantial morbidity.1234 AF affects millions of patients and increases one's risk of heart failure,56 stroke,78 and death.25 The prevalence of AF increases with advancing age, and the older adult population is increasing worldwide.91011121314 The prevalence of AF in Korea was 1.53% in 2015 and was reported as likely to increase to 5.81% by 2060.15 Given these findings, an increasing economic burden of AF on the health care system is anticipated, and it is important to estimate the cost and effectiveness of different therapeutic options.1016
Several studies recently compared the economic practicality of non-vitamin K antagonist oral anticoagulants to adjusteddose warfarin for the prevention of stroke in AF.17181920 It is known that rate-control and rhythm-control drugs do not show significant differences in mortality rates.2122 In a previous study in Korea, a rhythm-study strategy also showed no benefit on cardiovascular mortality, compared with a rate-control strategy.23 Meanwhile, economic studies comparing AF rate control versus rhythm control have revealed that rate control reduces costs, compared with rhythm control, which included electrical cardioversion in Western individuals: The study involved 4060 patient across 213 sites in Canada and the United States, with mean survival, resource use (hospital days, pacemaker procedures, cardioversions, percutaneous transluminal coronary angioplasties, coronary artery bypass graft procedures, valve surgery procedures, ablation, and short-stay and emergency department visits), costs, and cost-effectiveness compared as outcome indicators between rate-control and rhythm-control groups. Rate-control drugs included digoxin, atenolol, metoprolol, propranolol, diltiazem, and verapamil, and rhythm-control drugs included flecainide, propafenone, quinidine, disopyramide, moricizine, amiodarone, sotalol, and dofetilide. Rate-control costs were $5077 less per person than those for rhythm control.24 However, the cost-effectiveness of treating AF with ratecontrol and rhythm-control strategies has not been examined in Korea. The costs of drugs and hospitalization in Korea are different from those in Western countries. Moreover, recently, hospitalization for AF has increased by 420% from 767 to 3986 per 1 million Korean populations from 2006 to 2015 and hospitalization for AF control has increased compared with hospitalization for ischemic stroke and myocardial infarction (MI).16 Based on these results, cost-effectiveness analysis may play a substantial role in treatment selection. Therefore, we sought to compare the projected quality-adjusted survival and costs of different rate-control and rhythm-control drugs in Korean patients with AF.
MATERIALS AND METHODS
This study examined data from the National Health Insurance Service (NHIS) database. The NHIS is a single insurer controlled by the Korean government, and the majority (97.1%) of Korean residents are mandatory subscribers, with the remaining 3% being medical aid subjects. The sociodemographic information of patients, their use of inpatient and outpatient services, pharmacy dispensing claims, and mortality data were extracted. This study was approved by the Institutional Review Board of Yonsei University Health System (4-2019-0802), which waived the need for informed consent.
Study population
In the Korean NHIS database, a total of 268149 patients with prevalent AF who were aged 18 years or older were identified between January 1, 2013 and December 31, 2015. Those with valvular AF, such as moderate to severe mitral valve stenosis and prosthetic valve disease [International Classification of Disease 10th Revision (ICD)-I050, I052, I342] were excluded. Finally, this study included 212459 and 55690 patients who were taking rate-control and rhythm-control drugs, respectively. The rate-control drugs included digoxin, beta-adrenoceptor antagonists (atenolol, betaxolol, bevantolol, bisoprolol, carvedilol, propranolol), diltiazem, and verapamil, while the rhythm-control drugs included flecainide, propafenone, pilsicainide, amiodarone, sotalol, and dronedarone (Table 1).
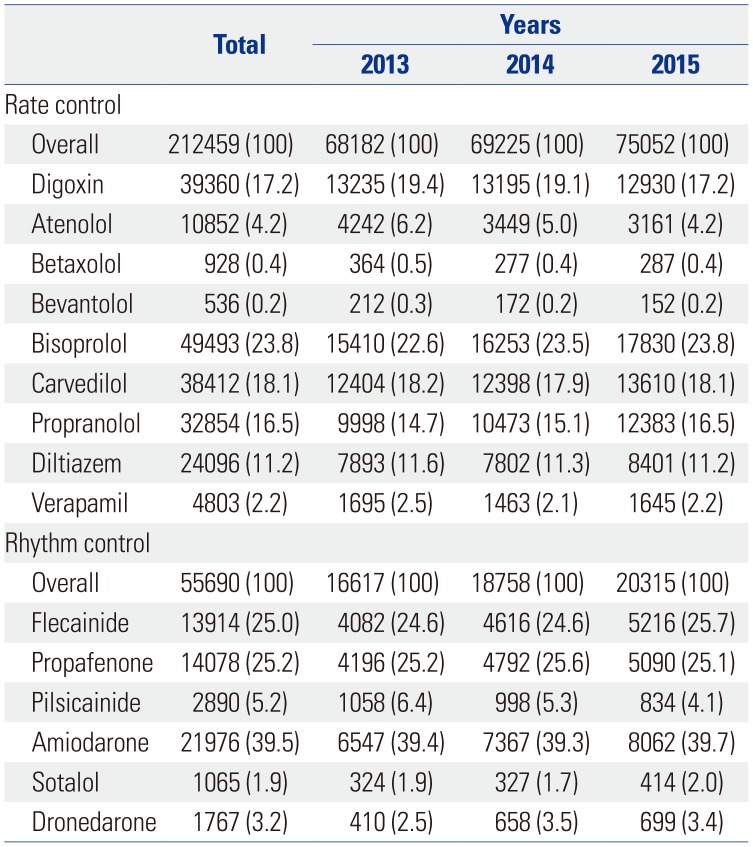
Table 1
Drugs Used to Treat Atrial Fibrillation in the Rate- and Rhythm-Control Groups among Patients Newly Diagnosed with Atrial Fibrillation between January 1, 2013 and December 31, 2015 in Korea
![]()
AF was diagnosed using ICD-10 codes I48 (AF and atrial flutter), I48.0 (AF), and I48.1 (atrial flutter). Moreover, patients were defined as having AF only when it was a discharge diagnosis or confirmed more than twice in the outpatient department to ensure diagnostic accuracy. The AF diagnosis was previously validated in the NHIS database with a positive predictive value of 94.1%. A validation study was performed in 628 randomly selected patients with the ICD-10 code I48 at two separate institutions. The patients' electrocardiograms (ECGs) were reviewed by two physicians. Patients were defined as AF if documented by ECG.162526
Decision model
We developed a Markov chain Monte Carlo model to evaluate the cost-effectiveness of the rate- and rhythm-control drugs. Health states modeled included healthy AF, congestive heart failure (CHF), MI, ischemic stroke, transient ischemic attack (TIA), intracranial hemorrhage (ICH), gastrointestinal bleeding (GI), and death. Cases of “fatal” CHF, MI, ischemic stroke, TIA, ICH, and GI bleeding were defined as transition to death. Non-fatal GI bleeding was assumed to be a transition to healthy AF. The health event was defined as newly diagnosed using ICD-10 codes for each event of CHF (I50.0, I11.0), MI (I21, I22), ischemic stroke (I63, I64), TIA (G45), ICH (I60, I61, I62), and GI bleeding (K92.2) within 1 year, considering that the transition cycle in the Markov model was 1 year in patients who had been on medication for more than 6 months after being newly diagnosed AF. We assumed that the healthy state transitioned annually based on the probability of an independent health event occurring within 1 year. The transition probabilities were estimated by cumulative incidence based on the data of the patients who were enrolled in this study between January 1, 2013 and December 31, 2015 (Table 2, Fig. 1; Supplementary Fig. 1, only online). Drug adherence rates were assumed to be similar in all groups, and efficacy was assumed to be relatively constant. To ensure patient follow-up for a lifetime, a cycle length of year and a time horizon of 20 years were used. Each year, the cohort accrued costs and quality-adjusted life years (QALY) depending on which health state they inhabited. The model was built in TreeAge Pro 2012 (TreeAge Software, Inc., Williamstown, MA, USA).
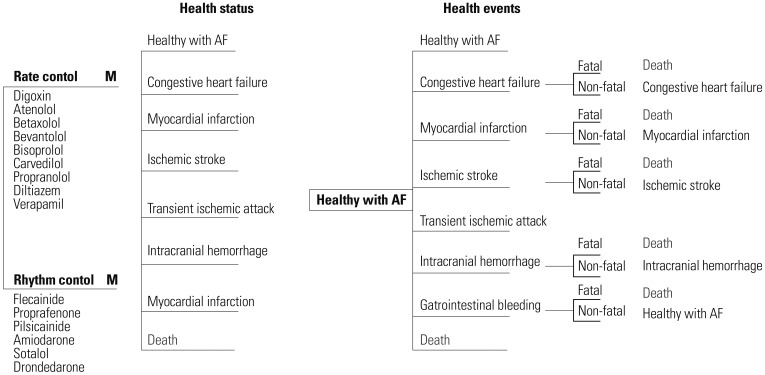
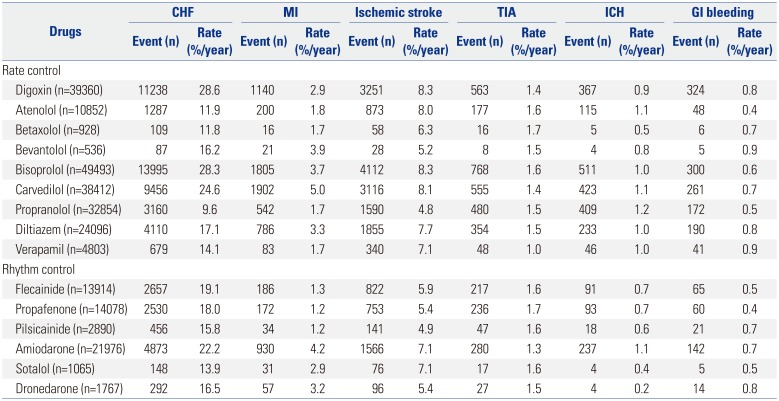
Fig. 1
Decision tree model. The treatment strategies are shown on the left in patients with newly diagnosed atrial fibrillation between January 1, 2013 and December 31, 2015 in Korea. Markov node (M) indicates a Markov process with eight health statuses and a cycle length of 1 year until death occurred or the 20-year time horizon was reached. Probabilities of health events depend on the treatment. Patients could die of ischemic stroke, intracranial hemorrhage, myocardial infarction, gastrointestinal bleeding, or other comorbidities. AF, atrial fibrillation.
![]()
Table 2
Base-Case Values Used in Sensitivity Analysis of Rate- and Rhythm-Control Drugs among Patients Newly Diagnosed with Atrial Fibrillation between January 1, 2013 and December 31, 2015 in Korea
![]()
Quality of life estimates
To measure quality-adjusted survival, QALY values were calculated by multiplying life years by utility scores derived from the medical literature.2728 By definition, death (from any cause) had a QALY of 0. The utility scores of CHF, MI, ischemic stroke, TIA, fatal GI bleeding, and ICH were 0.7, 0.9, 0.4, 0.8, 0.9, and 0.4, respectively. The discount rate was set at annual 3%, reflecting the annual inflation rate in Korea.29
Cost-effectiveness analysis
The net cost for each treatment drug by QALY was quantified over a period of 20 years using a societal perspective. The cost consisted of annual drug costs, maintenance costs, and single event costs. Annual drug costs were defined as the drug cost per day during 1 year based on the NHIS database (Supplementary Table 1, only online). The event-related cost was estimated as the average cost of hospitalization for the health event (Supplementary Table 2, only online). We estimated effectiveness (QALY) and the mean cost per tablet and year for the rate-control and rhythm-control groups. QALY and net costs were adjusted in each cycle related to the patients' health states. According to the amount of time a person spent in a health state, QALY and the costs accrued for each Markov state were weighted. Costs are expressed in US dollars, and the cost-effectiveness of individual drugs (rate control and rhythm control) was compared with atenolol through cost-effectiveness ratio (cost per QALY) and incremental cost-effectiveness ratio (ICER), which can be used for informed decision-making when resources are limited. Willing-to-pay was estimated at $30000 US/QALY, reflecting the GDP for Korea (US $29745 in 2017). Korean won (KRW) was converted to US dollars ($1 US=1000 KRW) in this analysis.
RESULTS
Number of prescriptions for each drug
During the study period, bisoprolol was the most commonly prescribed drug for rate control (23.8%), followed by carvedilol and digoxin (18.11% and 17.22%, respectively). Betaxolol and bevantolol had the lowest prescription rates (0.4% and 0.2%, respectively). Amiodarone was the most commonly prescribed rhythm control drug (39.7%), followed by flecainide and propafenone (25.7% and 25.1%, respectively). Sotalol had the lowest prescription rate (2.0%), followed by pilsicainide and dronedarone (4.1% and 3.4%, respectively).
Incidence of health events
In an integrated analysis involving all drugs, the number of ischemic strokes per year for bisoprolol was highest (8.3%), while that for pilsicainide was lowest (4.9%). The number of TIA, ICH, GI bleeding, MI, and CHF events per year was highest for betaxolol, propranolol, bevantolol, carvedilol, and digoxin (1.7%, 1.2%, 0.9%, 5.0%, and 28.6%, respectively), while that for verapamil, dronedarone, propafenone, pilsicainide, and propranolol was lowest (1.0%, 0.2%, 0.4%, 1.2%, and 9.6%, respectively).
Cost-effectiveness of rate control medications
Among the rate-control medications, the cost per QALY for propranolol was lowest ($487/QALY), while that for carvedilol was highest ($1363/QALY).
Based on base-case assumptions, the average lifetime treatments costs of rate-control drugs and QALY were $10443 and 13, respectively. The cost per QALY for atenolol was $714/QALY. Carvedilol had the highest cost per QALY ($1363/QALY), while propranolol had the lowest cost per QALY ($487/QALY). However, at a willingness-to-pay threshold of $30000 USD/QALY, all rate control drugs for treating AF were cost-effective. The incremental cost (−$1499) was lowest and incremental effectiveness (3 QALY) was highest with propranolol, which reflected a more valuable ICER (−$577/QALY) than that with atenolol (Table 3, Fig. 2, Supplementary Fig. 2, only online).
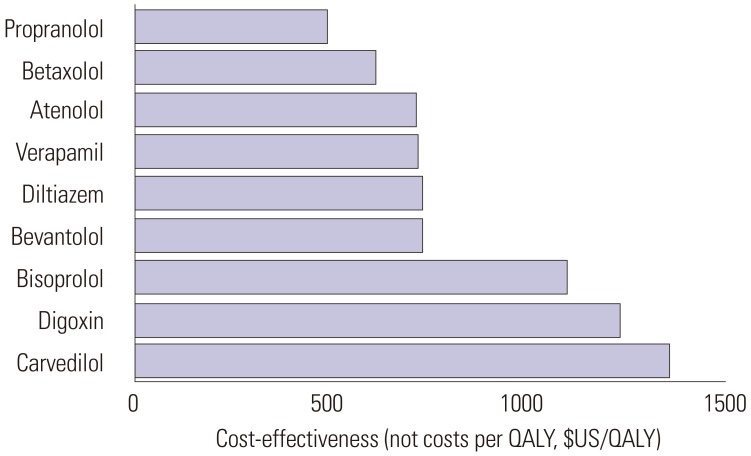
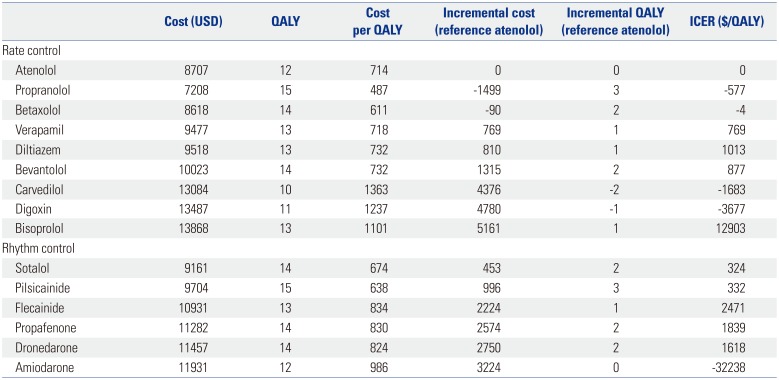
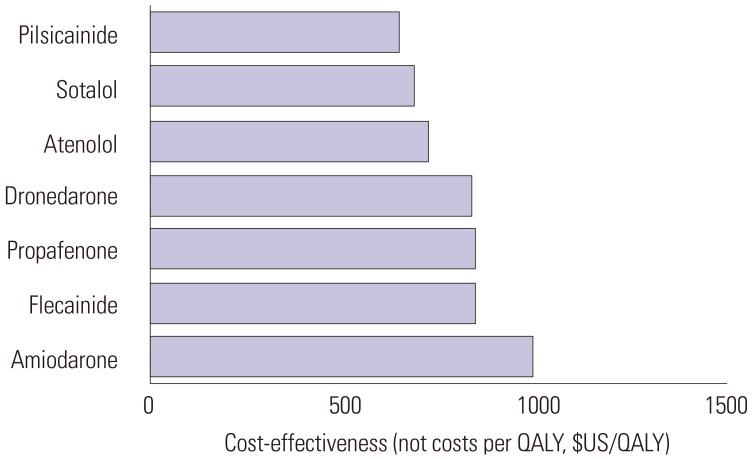
Fig. 2
Cost-effectiveness (bars) of rate-control drugs in patients with newly diagnosed atrial fibrillation between January 1, 2013 and December 31, 2015 in Korea. All drugs remained cost-effective at a willingness-to-pay threshold of $30000 per quality-adjusted life year (QALY).
![]()
Table 3
Projected Costs, QALYs, and ICERs for the Rate- and Rhythm-Control Drugs among Patients Newly Diagnosed with Atrial Fibrillation between January 1, 2013 and December 31, 2015 in Korea
![]()
Cost-effectiveness of rhythm control medications
Patients taking rhythm-control drugs lived an average of 14 QALY, with average lifetime treatments costs of $10745. Among the rhythm-control medications, the cost per QALY for pilsicainide was lowest ($638/QALY), while that for amiodarone was highest ($986/QALY). Flecainide, propafenone, and dronedarone had costs per QALY of $834, $830, and $824/QALY, respectively. Sotalol and pilsicainide had incremental cost ($453 and $996) and incremental effectiveness (2 and 3 QALY), demonstrating ICER values of $324/QALY and $332/QALY, respectively, compared with atenolol. Equivalent to rate-control drugs, the cost-effectiveness thresholds of the rhythm-control drugs in this analysis were lower than $30000 per QALY (Table 3, Fig. 3, Supplementary Figs. 3 and 4, only online).
Sensitivity analysis
Sensitivity analyses were performed to test uncertainty and to confirm the robustness of the results. The varying parameters in the analysis included discount rates of 5%, as well as 20% increases above previous assumptions for annual drug prices, annual maintenance costs, and costs of health incidents. The sensitivity analysis did not differ from the basic analysis despite changes in the discount rate and cost (Supplementary Tables 3 and 4, only online).
DISCUSSION
Our Markov chain Monte Carlo model showed that in patients treated with rate-control drugs, propranolol may be a cost-effective alternative to other agents in Korean patients with AF. Among rate-control drugs, propranolol showed the highest QALY and the lowest net cost, compared with atenolol. In patients taking rhythm-control drugs, sotalol and pilsicainide had lower net costs and increased QALYs, compared with atenolol. The present analysis demonstrated that propranolol, sotalol, and pilsicainide may be preferred alternatives based on costs among rate-control and rhythm-control drugs of use in Korea.
Previous studies have described a non-significant trend toward reduced survival in patients with AF who attempt rhythm control, compared with rate control.2122233031 Since economic factors may play a considerable role in selecting treatment options, several authors have investigated the cost-effectiveness of rhythm-versus rate-control strategies for treating AF.24323334 Eckman, et al.32 showed that cardioversion followed by the use of warfarin and amiodarone was the most effective strategy among several antiarrhythmic and antithrombotic treatment options. Catherwood, et al.33 found that cardioversion with or without antiarrhythmic drugs was more effective and less costly than rate-control drugs. Hagens, et al.34 demonstrated that treatment costs were higher for rhythm-control than rate-control drugs due to the higher costs of electrical cardioversion, hospital admission, and medication in patients with persistent AF. However, these studies were limited by the lack of randomized data on efficacy and resource use. Marshall, et al.24 performed an economic analysis of the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM)21 results and found non-significant differences in mean survival time, although treatment costs were always higher in the rhythm control group. In that study, the drug cost per day was greater for all of the rhythm-control drugs than the rate-control drugs. The authors compared resource use data, including medications, hospital visits, cardiac procedures, and short-stay and emergency department visits.
Here, we estimated the effectiveness (QALY) and mean net cost per year for individual rate- and rhythm-control drugs. Although bisoprolol and amiodarone were the most frequently prescribed drugs during the study period, we found that propranolol was the more cost-effective rate-control drug and that sotalol and pilsicainide were the most cost-effective rhythm-control drugs. These findings were based on a comprehensive calculation of net costs, incremental costs, QALY, and ICER.
Our study has several limitations. First, because details on the quantification and doses of the prescribed medications and treatment adherence were not available, we assumed that each medication was taken properly at standardized doses. Therefore, our data did not accurately reflect real life efficacy and safety because participants may exhibit superior medication adherence. Any misclassification would probably affect underor overestimation of the true difference in drugs costs. Second, we only analyzed health events of ischemic stroke, TIA, ICH, GI bleeding, MI, and CHF using Korean NHIS data for 3 years. These data do not fully reflect the analysis contents of the study in real world practice. According to limited data from the Korean NHIS, we did not further assess the association between treatment strategy and other resource events or procedures, such as cardioversion or pacemaker implantation. Third, patients who took two or more drugs were assigned to each drug. One patient could be included in a drug category more than twice. Because drug-based analysis was performed, it was not possible to estimate the overall medications costs for each patient. Fourth, with a mean age of 66 years, our patients were relatively old for patients with AF. Thus, while our results can be applied to AF patients in general, they probably cannot be generalized to younger patients with AF. Fifth, we assumed that any non-fatal GI bleeding would result in a healthy state. This may not always be the case and would likely be based on individual patient factors. Sixth, rhythm control strategies of guidelines in AF recommend specific class drugs depending on whether a patient has structural heart disease. However, we did an integrated analysis of rhythm-control drugs, regardless of the presence of cardiac structural abnormality. Therefore, direct comparison of cost-effectiveness among rhythm control drugs was not available in our study. Finally, much more work is needed to perform a cost-effectiveness analysis that can improve health outcomes and save system-wide costs.
In conclusion, propranolol and pilsicainide were found to be cost-effective in patients with AF in Korea, assuming that drug usage or compliance is the same. Notwithstanding, in addition to cost-effectiveness, drug selection ought to consider drug safety, patient preference, and side effects.
 XML Download
XML Download