

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gallbladder cancer (GBC) is a relatively rare disease that has been traditionally considered an incurable malignancy, owing to the advanced stage at diagnosis.12 Currently, radical surgery is the only curative option for GBC, but the extent of operation for T1/T2 GBC remains controversial. Generally, simple cholecystectomy alone (including laparoscopic cholecystectomy) is considered adequate for the pathologic stage of T1a GBC, as reflected by the current National Comprehensive Cancer Network guidelines (version 2017). However, for GBC of stage T1b or greater, radical cholecystectomy is recommended, which includes en bloc hepatic resection (segments IVB and V) and lymphadenectomy to clear all lymph nodes in the porta hepatis with/without bile duct resection. Nevertheless, the surgical extent for T1b and T2 GBC has been highly debated, and evidence of increased survival after radical cholecystectomy in patients with T1b GBC is lacking.3 Moreover, guidelines for surgical extent also vary greatly among institutions, and the global prevalence of GBC is imbalanced with high incidence rates reported in South America and Asia.4 However, the higher recurrence rate reported with simple cholecystectomy in cases with stage T1b suggests that more radical operations should be considered.5
With regard to the extent of radical cholecystectomy, the policy for T1/T2 GBC at Severance Hospital traditionally included liver resection. However, our earlier experiences showed that recurrences in the liver rarely occur, and we opted not to resect the liver during radical cholecystectomy.6 We encountered recurrences in distant lymph nodes, especially para-aortic lymph nodes after radical cholecystectomy; therefore, beginning in 2005, we routinely extended lymphadenectomies to include the para-aortic lymph nodes in patients with T1/T2 GBC. Moreover, our experiences with complications in the common bile duct after radical cholecystectomy have led us to include the insertion of a T-tube as the final step of operation. The present study analyzes the oncologic outcomes of patients at Severance Hospital undergoing these treatments with extended lymphadenectomy and without liver resection.
Go to : 
MATERIALS AND METHODS
Patients and study design
From January 2005 to December 2017, 164 patients with GBC underwent operation by a single surgeon (WJL) at Severance Hospital. We retrospectively reviewed the cases of 113 patients who underwent extended cholecystectomy without hepatectomy and were pathologically determined to be at stages T1 and T2. Pathological results, including T and N stages, were defined according to the American Joint Committee on Cancer (AJCC) cancer staging manual, 7th edition. Patients who underwent additional hepatectomy under the suspicion of T3 tumor were excluded as they were not within our treatment algorithm. Four patients who underwent palliative operations without radical cholecystectomy were also excluded. This study was reviewed and approved by the Institutional Review Board of Yonsei University College of Medicine, Seoul, Republic of Korea (IRB: 4-2017-0262).
Preoperative evaluation
Patients with suspected GBC from abdominal ultrasonography and/or computed tomography underwent positron emission tomography to assess distant metastases. Endoscopic ultrasonography was used to assess tumor invasion depth. In cases with incidentally diagnosed GBC, positron emission tomography was performed after laparoscopic cholecystectomy to evaluate possible metastatic lesions. Carbohydrate antigen 19-9 was evaluated as the tumor marker.
Operative strategy and adjuvant treatment
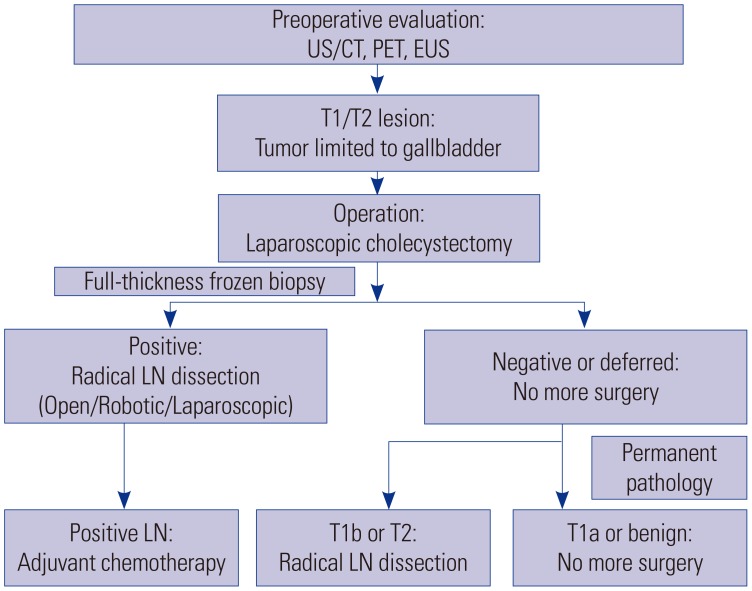
A schematic detailing the treatment algorithm is shown in Fig. 1. Three different approaches to radical cholecystectomy were employed: open or minimally invasive (laparoscopic and robotic). If preoperative evaluation suggested a T2 lesion with suspicious lymph node metastasis, the operation was performed using an open approach. For T1 and T2 lesions without suspicious lymph node metastasis, laparoscopic cholecystectomy was performed initially. During cholecystectomy, the cystic plate was completely removed with the gallbladder to avoid exposing the subserosal layer. If the results of a full-thickness frozen biopsy were positive for malignancy, radical lymph node dissection was performed. The extents of lymphadenectomy were hepatoduodenal (#12), common hepatic artery (#8), retropancreatic (#13), and para-aortic (#16). T-tubes were routinely inserted into the common bile duct. As noted above, liver resection was not performed for all T1 and T2 lesions. If the frozen biopsy results were negative or indeterminate, no further operation was performed until the pathology was confirmed. If the results confirmed a T1b or T2 lesion, radical lymph node dissection was subsequently performed. Cases with T1b and T2 lesions referred from other hospitals after laparoscopic cholecystectomy underwent reoperation via an open approach.
The role of adjuvant chemotherapy remains unclear, with some reports of benefit in node-positive GBC or R1 disease.78 Therefore, adjuvant chemotherapy was only considered in cases of lymph node metastasis or gallbladder perforation during operation. Postoperative complications were graded according to Clavien–Dindo classifications.9
Statistical analysis
All statistical analyses were performed using Statistical Package for Social Sciences version 20 (IBM Corp., Armonk, NY, USA). For each quantitative variable, Shapiro–Wilk test was used as a test of normality. Disease-specific survival and disease- free survival were analyzed using Kaplan–Meier method and compared by log-rank tests. Cox proportional hazards model was used for multivariate survival analysis. Statistical significance was set as p value <0.05.
Go to :
RESULTS
Clinicopathologic characteristics
For the 109 patients included in our analysis, the mean age was 65±9 years, and 47 patients (43%) were male. Forty-five patients (41%) were diagnosed with incidental GBC. Among them, 11 patients (24%) were diagnosed with T1a GBC and did not undergo further operations. The mean level of carbohydrate antigen 19-9 was 13.0±16.8 U/mL. The median follow-up was 50 months (range, 5–145 months). The mean number of retrieved lymph nodes was 14±9 lymph nodes. Node-positive GBC was found in 14 patients (13%). Among them, 12 patients underwent adjuvant chemotherapy and two patients refused adjuvant therapy.
Comparison of clinicopathologic outcomes between T stages
Clinicopathologic characteristics according to T stage are shown in Table 1. Clinical characteristics did not differ among T stages. There were no differences in terms of the locations of tumors, i.e., hepatic vs. peritoneal sides (p=0.805); however, tumors involving hepatic side were more frequent (n=63, 58%). With regard to histologic differentiation, higher T stages were significantly associated with poorly differentiated GBC (p=0.004). Two patients in T2 group with poorly differentiated GBC showed combined neuroendocrine features in the pathologic report. Significantly higher lymph node metastasis was noted in T2 group than those in T1b and T1a groups (21% vs. 4% and 0%, respectively, p<0.001). The numbers of retrieved lymph nodes were higher for T1b and T2 groups than for T1a group (p<0.001) (Table 1). In T1a group, six patients who were diagnosed with incidental GBC did not undergo lymph node dissection, whereas 15 patients did as a higher T stage was suspected.
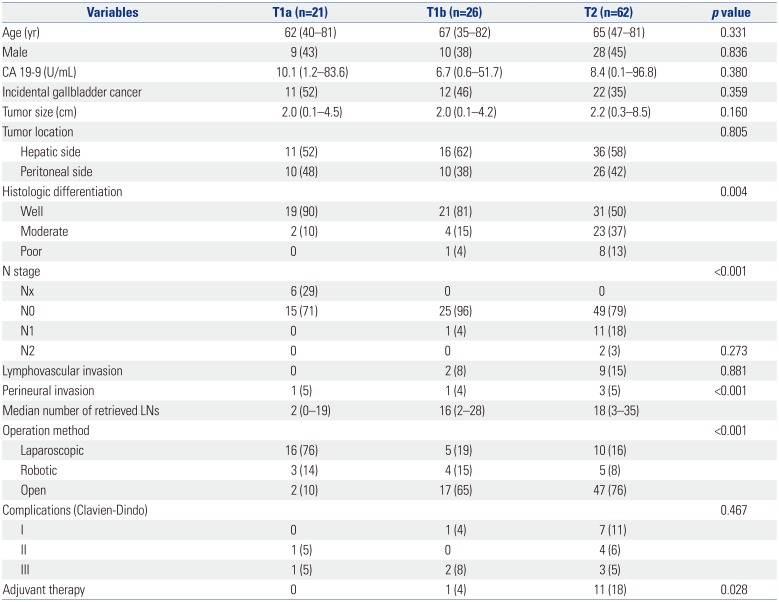
Table 1
Clinicopathologic Characteristics according to T Stage
![]()
There were no significant differences between stages in terms of complications (p=0.467). All grade I complications were either fever or wound seroma. Grade II complications were chylous leakage (two cases), which were medically managed, and abscess formation (three cases), which were managed with antibiotics. Grade III complications were postoperative bile leakage requiring endoscopic retrograde biliary drainage (five cases), and intra-abdominal abscess formation requiring percutaneous catheter drainage (one case).
Operative technique and postoperative complications
Open radical cholecystectomies were performed in 66 patients (61%), whereas the approaches were laparoscopic for 31 patients (28%) and robotic for 12 patients (11%). The median (range) operation times for open, laparoscope, and robotic radical cholecystectomies were 183 (95–340), 73 (30–173), and 231 (172–278) min, respectively (p<0.001). There were three cases of open conversion during minimally invasive approaches: one from phrenic artery injury (laparoscopic approach) and two from renal vein injury and aortic wall bleeding (robotic approach).
There were no significant differences in complications between operative techniques (p=0.066). For minimally invasive approaches, there were no complications in laparoscopic group, but three complications (24%) were observed in robotic group: grade I for fever, which was treated conservatively; grade II for intra-abdominal abscess formation requiring antibiotics; and grade IIIA requiring endoscopic retrograde biliary drainage due to postoperative bile leakage. There were 13 complications (21%) in patients undergoing an open approach: six cases were grade I for fever and wound seroma, four in grade II (including two cases of postoperative chylous leakage and two cases of intra-abdominal abscess formation requiring pharmacologic treatments), and three in grade IIIA (including two cases of endoscopic retrograde biliary drainage due to postoperative bile leakage and one case of percutaneous catheter drainage for intra-abdominal abscess formation).
Oncologic outcomes
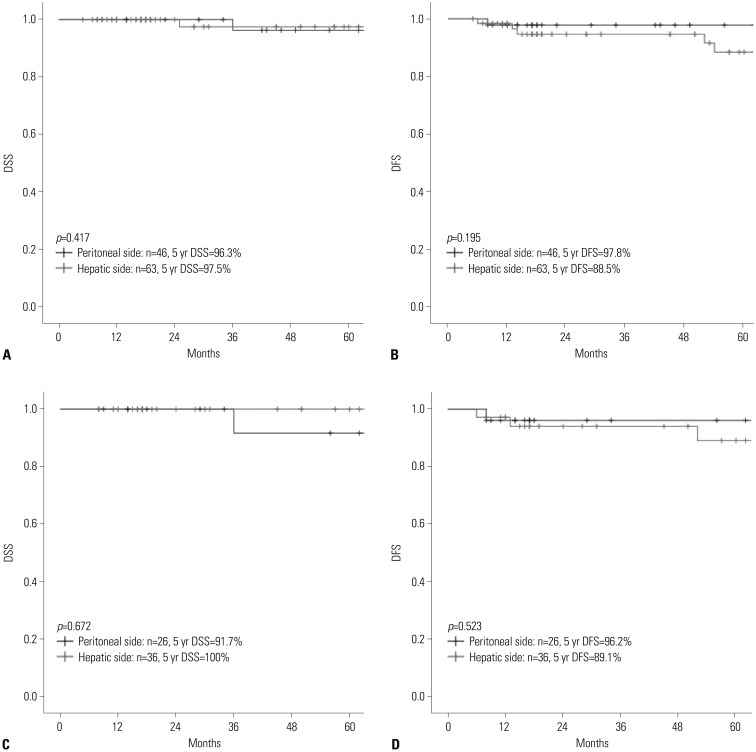
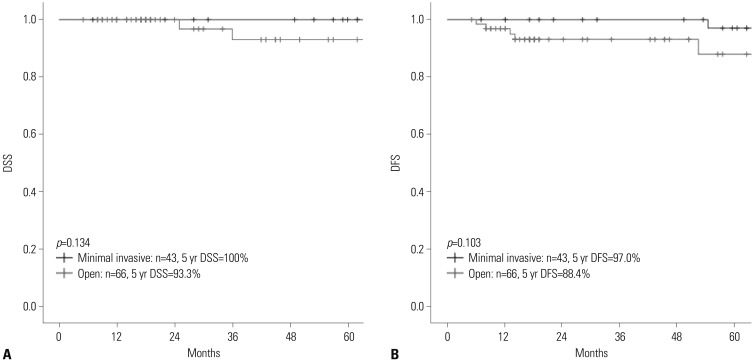
There were four GBC-related mortalities during the study period, and the 5-year disease-specific survival rate was 97%. There were no significant differences according to T stage in disease-specific survival (p=0.366; Fig. 2A) or disease-free survival (p=0.457; Fig. 2B). In all T stages, the median survival was not reached for analysis. In N2 disease, significantly poor oncologic outcomes (5-year disease-specific survival: 50%, 5-year disease-free survival: 0%; Fig. 3) were observed. Oncologic outcomes were not associated with the tumor location (Fig. 4) nor the type of surgical approach (Fig. 5).
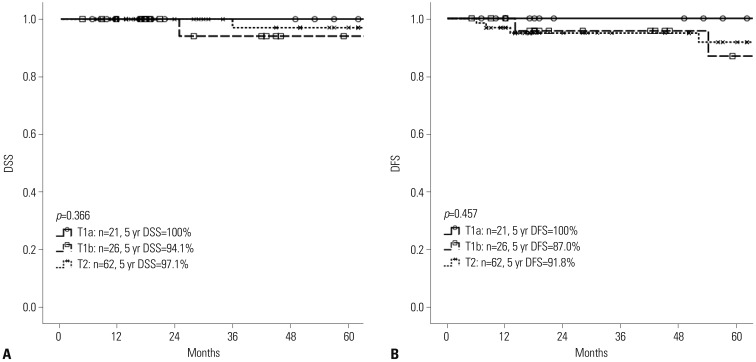 | Fig. 2Oncologic outcomes according to T stage. (A) Disease-specific survival (DSS). (B) Disease-free survival (DFS).
|
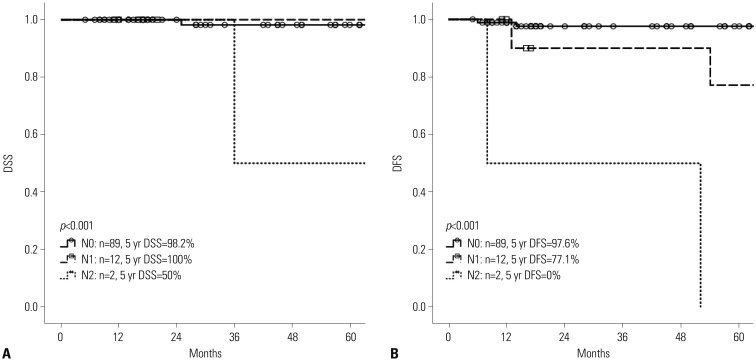 | Fig. 3Oncologic outcomes according to N stage. (A) Disease-specific survival (DSS). (B) Disease-free survival (DFS).
|
Recurrence pattern
The details on recurrence for each GBC stage are shown in Table 2. Overall, there were six cases of recurrence, with a 5-year disease-free survival rate of 92.4%. In cases with T1a GBC, no lymph node metastasis was found in 15 patients who underwent lymph node dissection. Among the 26 patients with T1b lesions, there was only one patient (4%) with lymph node metastasis, and two patients (8%) had recurrence. For T2 GBC, 13 patients (22%) had lymph node metastasis, two of whom were staged N2: one patient had only single lymph node metastasis in retropancreatic lymph nodes from total of 26 lymph nodes investigated, and the other patient had one metastatic paraaortic lymph node and four metastatic hepatoduodenal lymph nodes from a total of 20 lymph nodes investigated. These patients with N2 staging showed recurrences. Two patients showing poorly differentiated adenocarcinoma with neuroendocrine features had recurrence within 1 year after the operation.
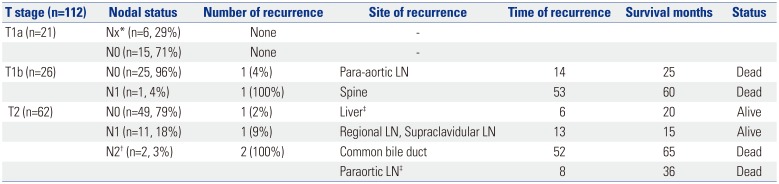
Table 2
Lymph Node Status and Recurrence Patterns according to T Stage
![]()
Go to :
DISCUSSION
Historically, GBC has been associated with pessimistic oncologic outcomes. In 1924, Blalock10 wrote that “in malignancy of the gallbladder, when a diagnosis can be made without exploration, no operation should be performed, in as much as it only shortens the patient's life.” With improvements in radiology and the invention of laparoscopic operations, early diagnoses of GBC have become more frequent. However, the curative options are limited to radical operations, as GBC has a propensity for early dissemination and is proximal to the liver and major vasculature. Recently, favorable outcomes after less radical cholecystectomies have been reported in patients with T1/T2 GBC, with some reports on the safety and non-inferior oncologic outcomes of laparoscopic approach.11121314 However, there is no consensus on the extent of surgery during radical cholecystectomy except for T1a GBC, in which laparoscopic simple cholecystectomy is adequate. Further lymph node dissection may still be indicated, as frozen biopsies during operations cannot always discriminate between T1 and T2 GBC.
Clarification of the oncologic outcomes for GBC is difficult due to the heterogeneity of operative techniques. For example, the extent of surgery differs among surgeons and institutions. Therefore, to compare oncologic outcomes based on the extent of surgery, we analyzed cases involving a single surgeon (WJL) at Severance Hospital, where laparoscopic operations for GBC have been performed since 1993. At that time, if a patient was diagnosed with incidental T1a GBC, routine follow-up was scheduled. For those with T1b GBC or higher, open radical cholecystectomies were performed, unless the patients refused for personal reasons. Our previous reports on patients who did not undergo further radical cholecystectomy due to personal reasons or the patients' general condition showed that the 5-year survival rates of GBC patients with T1a, T1b, and T2 lesions were 100%, 75%, and 56.2%, respectively.15 Two cases of recurrences in para-aortic lymph nodes were noted after radical cholecystectomy, including only regional lymphadenectomy, in patients with T2 GBC at 1 month and 5 months. There was no recurrence in the liver bed, which extends from the cystic plate, in any of the patients. Starting in 2005, with the introduction of robotic system at Severance Hospital, minimally invasive radical cholecystectomies, including the robotic approach, were also performed. Our results have shown no differences in oncologic outcomes among different surgical approaches. Therefore, for T1/T2 GBC, having a consistent and reasonable operative principle is more important than the mode of surgical approach.
Our anecdotal experiences have indicated that the dissection of regional lymph nodes along with para-aortic lymph nodes may reduce recurrence. Para-aortic lymph nodes are the final destination in the abdominal lymphatic route from the gallbladder via the cholecysto-retropancreatic pathway and the retroportal node.16 However, evidence on the role of extensive lymphadenectomy is lacking. Tsukada, et al.17 reported that in T2 GBC, metastases in para-aortic lymph nodes were discovered in 12% of cases, whereas Ogura, et al.18 reported lymph node metastases in 44.3%, with 2.5% of T1a and 15.6% of T1b cases also showing metastases. Nevertheless, para-aortic lymphadenectomy did not seem to provide any survival benefit.19 In contrast, our findings suggest a benefit of extensive lymphadenectomy on the oncologic outcomes of GBC patients without pre-existing lymph node metastases.
One recent meta-analysis of T1 GBC found comparable survival outcomes between simple and extended cholecystectomies,20 whereas another meta-analysis reported conflicting results and suggested an improved prognosis associated with liver resection and lymph node resection for stage T1b GBC or higher.21 However, the authors of both meta-analyses noted that a lack of essential data for comparison and a lack of standardization in operative extent and definition can limit the interpretation of the results. Additionally, since liver parenchyme is not involved in T1/T2 GBC, the complete excision of the cystic plate along with the gallbladder may be sufficient. Indeed, our experiences after the implementation of these principles in 2005 have indicated better oncologic outcomes for GBC, especially for T2 tumors. The 5-year disease-specific survival rate was 97.1% at Severance Hospital, compared to rates ranging from 69.4% to 90.2% in previous studies.61422 Although this study found one recurrence in the liver, it was bi-lobular and distant from the cystic plate. Horiguchi, et al.23 also reported no difference in disease-free survival rates between patients receiving cystic bed resection only and those also undergoing liver resection. Therefore, the complete excision of the cystic plate should be adequate for T1/T2 GBC.
Nortably, the percentage of incidental GBC cases following cholecystectomy in the present report was higher than those reported for laparoscopic cholecystectomies, which ranged from 0.2% to 1.1%.24 This may be due to the fact that Severance Hospital is a tertiary referral hospital. Additionally, our results indicate that the location of the tumor, whether on the hepatic or peritoneal side, does not influence the oncologic outcome, even though the current 8th AJCC staging system further divides T2 stage accordingly.
In terms of recurrence, six incidences were observed in our study group. Two cases of recurrence showed that GBC was poorly differentiated with neuroendocrine features, which is known to behave more aggressively.25 Among the remaining four cases, one patient was initially diagnosed with T1b lesion without lymph node metastasis, and had recurrence at the paraaortic lymph node 14 months later. This may have resulted from an incomplete para-aortic lymph node dissection; therefore, radical cholecystectomy in T1b should be sought more actively.
Regarding postoperative complications, some patients showed postoperative bile leakage. These complications may have resulted from complete and radical dissections of hepatoduodenal lymph nodes, which completely expose the common bile duct and disrupt its blood supply. We now routinely insert T-tubes to prevent such postoperative biliary complications.
The limitations of the present study include the limited number of patients analyzed, as well as the inherent selection bias resulting from the retrospective design and selection criteria of the study. Five patients who underwent additional hepatectomy under the suspicion of T3 tumor were excluded from this study. The operative finding showed that the possibility of acute inflammation and liver invasion could not be completely excluded. Therefore, the current treatment algorithm should be applied with discretion in patients with acute inflammation. Furthermore, these results were based on the experience of a single surgeon (WJL). Nevertheless, the preventive role of extensive lymphadenectomy, including para-aortic lymph node dissection, should be given further attention, and more surgeons should consider our operative principle to enable a large-scale cohort study.
A complete R0 resection in GBC is the standard of care in patients with localized disease. However, there is no consensus on the extent of radical cholecystectomy for T1/T2 GBC, partly due to the low incidence of GBC that impedes randomized controlled trials to establish optimal treatment modalities. Here, we report on our experiences with an operative principle at Severance Hospital, which indicates that extended lymphadenectomy with para-aortic lymph node dissection without liver resection for T1/T2 GBC produces favorable oncologic outcomes.
Go to :
 XML Download
XML Download