

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Advances in imaging techniques have led to the recognition of a transitional state of prostate cancer (PCa) in which the disease has limited metastasis beyond the prostate. In 1995, Hellman and Weichselbaum first identified and termed this entity as oligometastasis.1 Uppal, et al.2 suggested that metastatic disease between oligometastatic and polymetastatic patients have a separate regulation process, suggesting that the diseases mentioned above are distinct entities rather than different points along a development continuum. Other researchers indicated that definitive directed treatments for PCa with limited metastases may confer survival benefits for a select population.3
Androgen deprivation therapy (ADT) remains a cornerstone of systemic therapy through which to delay disease progression and to alleviate cancer-related symptoms in patients with metastatic hormone-sensitive prostate cancer (mHSPC).4 Many have regarded ADT as the treatment of choice for this population; however, recent evidence-based guidelines recommend concurrent aggressive treatment options, including local therapy or upfront chemotherapy.5 This recommendation is based on emerging data that suggest treatments targeted at the primary tumor and metastatic lesions in patients with limited metastases may prevent or delay the need for palliative treatments and confer survival benefits.6
The risks of cerebrovascular disease (CVD) and PCa increase with age, and 16% of patients with ischemic stroke have been found to harbor PCa.7 While an association between PCa and CVD has not been elucidated, cancers have been shown to be associated with an increased risk of CVD through various biological mechanisms, including direct tumor effects or coagulation disorders.89 Meanwhile, treatment decisions for PCa should be made based on a patient's comorbidities and functional status, which can affect overall survival (OS). Therefore, the risk of mortality from mHSPC and its treatment should be weighed carefully against the risk of mortality from existing significant comorbidities, such as CVD or cardiovascular disease, when making treatment decisions.10 Multiple comorbidities are frequently noted at the time of biopsy-proven mHSPC. Unfortunately, there is no consensus on which subgroup of patients for whom local treatment of the primary tumor may confer a survival benefit.
The primary endpoint of this study was the prognostic value of local treatment of primary tumors on OS outcomes in patients with de novo mHSPC. The secondary outcome was the confounding effect of comorbidities, such as CVD, at the time of mHSPC diagnosis on the prognostic impact of local treatment.
Go to : 
MATERIALS AND METHODS
Study population and data collection
Clinicopathological data for 1017 consecutive patients with newly diagnosed mHSPC between August 2003 and November 2016 were retrospectively collected from two institutions, Severance Hospital and Gangnam Severance Hospital (Yonsei University Health System). After stratifying patients by a history of CVD, baseline characteristics, including age, body mass index, prostate-specific antigen (PSA) level, TNM stage, Gleason score, Eastern Cooperative Oncology Group performance status, site of metastasis, preexisting medical conditions, such as hypertension and diabetes mellitus, and treatment types were reviewed. CVD was defined as previous radiological evidence of infarction on computed tomography brain scan identified by corresponding focal neurological deficit. Patients were excluded from the analysis if they had incomplete clinical data (n=56), were lost during follow up (n=42), or had an unknown cause of death (n=40). In result, 879 (86.4%) patients were included in the final analysis.
Patient survival and causes of death were investigated using the National Cancer Registry Database or institutional electronic medical records. The OS interval was defined as the time interval from PCa diagnosis to the date of all-cause death. Cancer- specific survival interval was defined as the time interval from PCa diagnosis to the date of death due to PCa. This retrospective study was approved by the Gangnam Severance Hospital Institutional Ethics Committee (2017-0186-001), which waived the requirement for informed consent. All study procedures complied with the principles of the 1946 Declaration of Helsinki and its 2008 update.
Treatments administered
Decisions on the type of initial treatment were determined based on physician discretion and patient preference. All patients received long-term ADT with or without local treatment [radical prostatectomy (RP) or radiation therapy (RT)]. RP was performed by a retropubic or robotic approach, with the extent of pelvic lymph node dissection based on risk category. RT consisted of intensity-modulated external beam RT, with a median RT dose of 7000 cGy (interquartile range: 7000–7000). Metastasis-directed local treatments, including RT and/or metastasectomy, were offered for patients with symptomatic disease or those with a limited metastatic burden.
The diagnosis of castration-resistant PCa (CRPC) was based on consecutive rises in serum PSA levels, new symptom development, or radiological progression despite a castrate serum testosterone level <50 ng/dL during ADT. Systemic treatments targeted against CRPC were performed according to contemporary guidelines.
Statistical analyses
The study groups were compared using the two-sided Mann–Whitney U-test for the analysis of continuous variables and the chi-square test for the analysis of categorical variables. Variables considered potential predictors for multivariate modeling were selected by univariate analyses using the Cox proportional hazards regression model.
To compare the OS outcomes of each patient group, Kaplan-Meier survival analysis was performed according to prior CVD history and the type initial treatment (ADT alone vs. local treatment). All statistical analyses were performed using IBM SPSS software (version 21.0; IBM Corporation, Armonk, NY, USA). Differences with a p value<0.05 were considered statistically significant.
Go to :
RESULTS
Baseline characteristics
Baseline features of the patients included in the analysis, stratified by prior CVD history and the type initial treatment, are described in Table 1. Of 879 patients, 660 (75.1%) underwent ADT alone, 90 (10.2%) underwent RT with ADT with or without metastasis- directed therapy, and 129 (14.7%) underwent RP with ADT with or without metastasis-directed therapy.
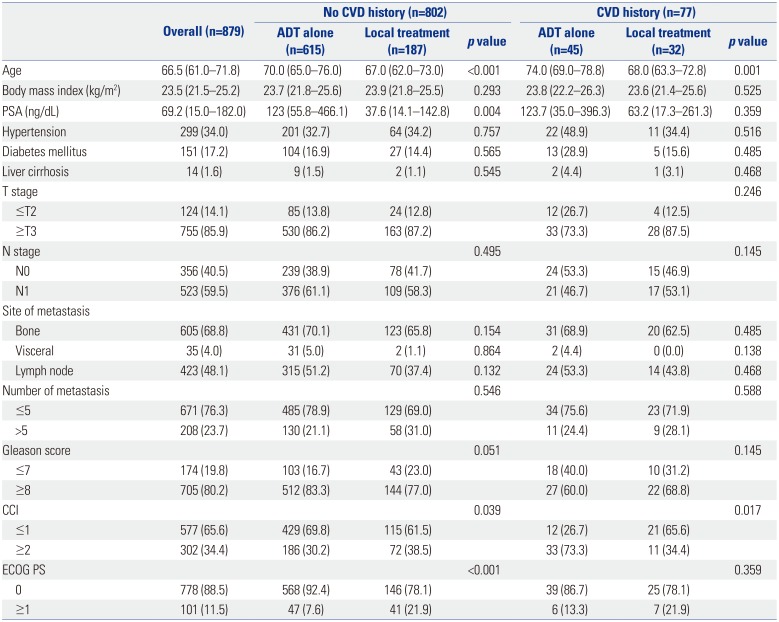
Table 1
Clinicopathological Characteristics of Patients with Metastatic Prostate Cancer Stratified by Cerebrovascular Disease History and Initial Treatment Category
![]()
Within all CVD history subgroups, patients who received ADT alone were older and exhibited higher Charlson Comorbidity Index (CCI) values than men who received local treatment. In the subgroup without a history of CVD, patients who received ADT alone had higher serum PSA levels than men who received local treatment. However, the two treatment subgroups were comparable in their distributions of all other classic PCa survival prognosticators. Moreover, there was no significant difference in the number or sites of metastasis between the ADT alone and ADT with local treatment groups (p=0.521, data not presented).
Systemic treatments administered following CRPC diagnosis are shown in Table 2. In the subgroup with CVD history, patients who received local treatment were more likely to have received a greater number of docetaxel cycles than men who received ADT alone. However, there were no differences in the proportions of androgen receptor axis-targeted agents, cabazitaxel usage, enrollment in clinical trials, and secondary hormonal manipulations.
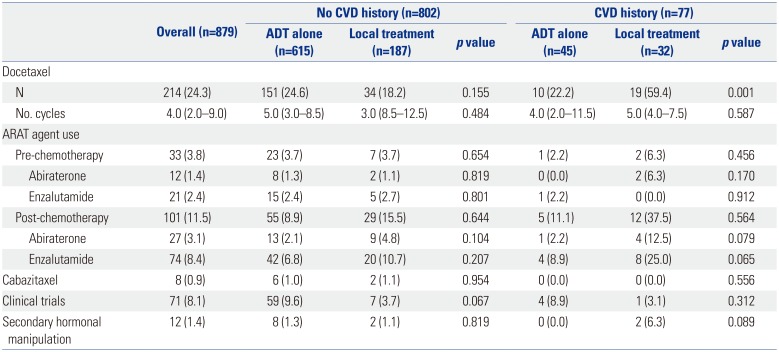
Table 2
Systemic Treatments Administered Following Progression to Castration-Resistant Prostate Cancer
![]()
Survival outcomes
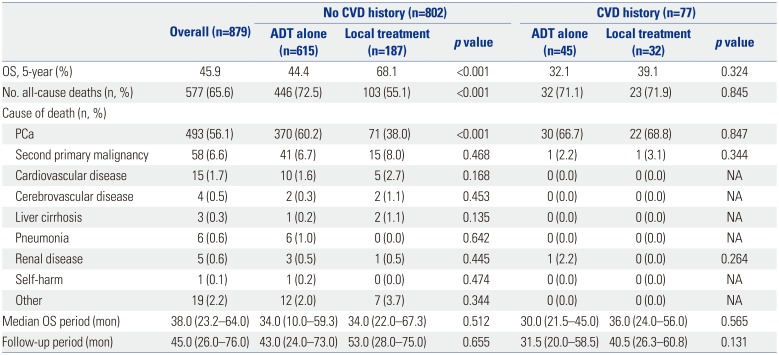
Table 3 and Fig. 1 show the OS outcomes of the overall cohort and the subgroups stratified according to prior CVD history and the type of initial treatment. In the overall group (Fig. 1A) and in patients without a history of CVD (Fig. 1B), men who received local treatment exhibited higher OS than men who received ADT alone (all p<0.001). However, the survival benefit of local treatment was not seen in the subgroup of patients with a history of CVD (p=0.324) (Fig. 1C). OS outcomes were comparable between patients who received RP and RT (p=0.521, data not presented). The leading causes of death were attributable to PCa, followed by second primary malignancy and cardiovascular disease (Table 3).
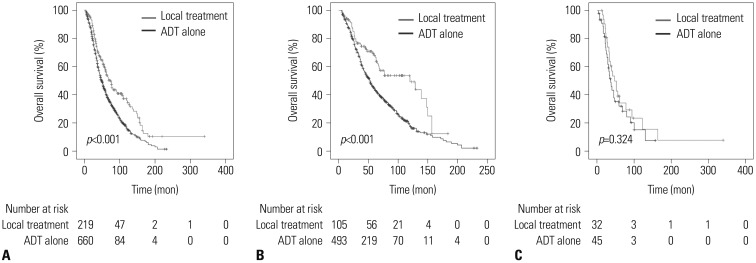 | Fig. 1Kaplan-Meier curves showing overall survival in patients stratified by a history of cerebrovascular disease (CVD). (A) Overall group, (B) patients without a history of CVD, and (C) patients with a history of CVD. ADT, androgen-deprivation therapy.
|
Table 3
Survival Outcomes in Patients with Metastatic Prostate Cancer Stratified according to Cerebrovascular Disease History and Initial Treatment Category
![]()
Predictors of survival
Univariate and multivariate models of predictors of overall mortality (OM) are shown in Tables 4, 5, and 6. In the overall group and the subgroup without a history of CVD, multivariate analysis showed local treatment to be associated with a lower risk of OM, whereas this was not seen in the subgroup with a history of CVD.

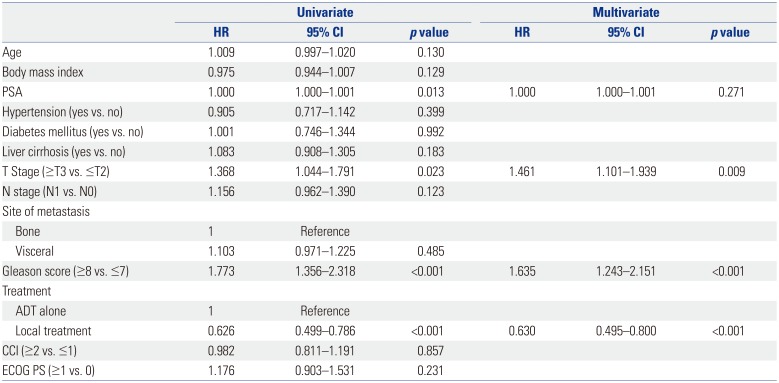
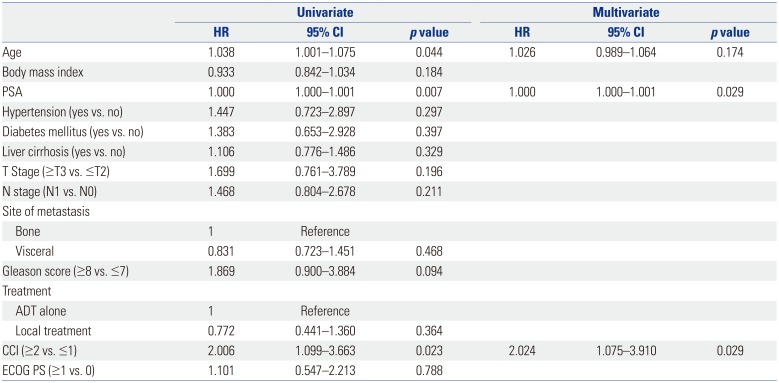
Table 4
Cox Regression Models for Risk Factors associated with Overall Mortality in the Overall Cohort
![]()
Table 5
Cox Regression Models for Risk Factors associated with Overall Mortality in Patients without a History of Cerebrovascular Disease
![]()
Table 6
Cox Regression Models for Risk Factors associated with Overall Mortality in Patients with a History of Cerebrovascular Disease
![]()
In the overall group, serum PSA level, history of CVD, stage ≥T3, and Gleason score ≥8 were significant prognosticators of OM (Table 4). In the subgroup without a history of CVD, stage ≥T3 and Gleason score ≥8 were associated with a higher risk of OM (Table 5). In the subgroup with a history of CVD, serum PSA level and CCI were associated with a higher risk of OM (Table 6).
Univariate and multivariate models of predictors for cancer-specific mortality in the overall group are shown in Table 7. Age, stage ≥T3, Gleason score ≥8, and prior local treatment were significant prognosticators (Table 7).
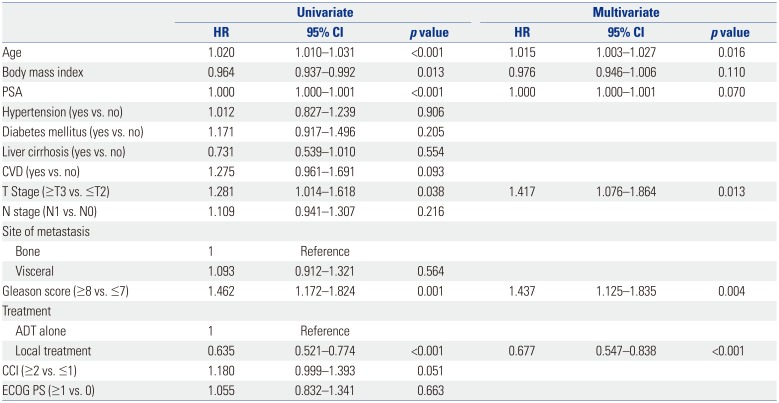
Table 7
Cox Regression Models for Risk Factors associated with Cancer-Specific Mortality in the Overall Cohort
![]()
Go to :
DISCUSSION
There has been a paradigm shift in considering local treatments targeted at both the primary tumor and metastatic lesions in patients with mHSPC and limited metastatic burden.6 However, there is no guideline on which subgroup of patients for whom such aggressive treatments may confer a survival benefit. We observed an OS benefit with local treatment of the primary tumor in patients regardless of the metastatic burden. However, the survival benefit with local treatment was not seen in patients with a prior history of CVD. These findings suggest that comorbidities are crucial factors that affect the survival benefit of local treatment in patients with mHSPC.
The biological definition of oligometastatic PCa remains debatable, and advances in imaging techniques are shifting the treatment paradigm of this disease entity. Various studies have proposed different definitions regarding the number and sites of metastatic lesions to define oligometastatic PCa based on oncological outcomes.1112 The definition regarding the cut-off number of metastatic lesions is yet controversial, and for now, this disease entity should only be interpreted as a disease state between the presence of intravascular circulating tumor cells and disseminated metastasis.1314 Existing studies regarding oligometastatic PCa exclude patients with underlying comorbidities, such as CVD.1516171819 Our study cohort included patients with initially diagnosed mHSPC regardless of the number of metastatic lesions and comorbidities, and there was no significant difference in metastatic burden between the ADT alone and ADT with local treatment groups. In an attempt to identify a subset of patients who would benefit from local treatment of mHSPC, our study suggests that the number of metastatic lesions may not be the most significant indicator for predicting a survival benefit with local treatment.
Our study showed that CVD, followed by Gleason score, was the strongest prognosticator of OS. Several hypotheses can be offered. First, the detrimental effect of CVD on OS may have offset the beneficial effect of local treatment, in addition to well-known prognostic factors, such as Gleason score and tumor stage. CVD is known to be significantly associated with survival, with a 0.15-year loss of life expectancy in the aged population.20 It has been reported that the risk of thromboembolic disease increases as cancer stage increases.21 Babiker, et al.22 showed that the early release of prostasomes originating from PCa cells into the bloodstream evokes coagulation effects resulting in an increased risk of thromboembolism. Brain injury resulting from vascular pathology can also activate the coagulation cascade, causing a state of hypercoagulability with the release of thromboplastin-like factors from the central nervous system.23 In summary, a history of CVD, which indicates pathological hemostatic changes, may contribute to the disease course and OS outcomes. Future studies are warranted to identify the underlying pathophysiology of CVD in the PCa microenvironment. Second, the administration of continuous ADT may exacerbate CVD and its disease course. ADT increases coagulation disorders that are related to a complex interplay of factors, including procoagulant factors released by tumor and/or host blood vessels.22 Hypercoagulability is common in cancer patients, and hence, it is reasonable to consider that ADT serves as an aggravator of CVD and inferior OS outcomes. Our results imply that comorbidities, especially CVD, are potential risk factors to be accounted for when considering local treatments in addition to ADT for patients with mHSPC.
The strengths of our study are the inclusion of detailed clinicopathologic data, treatment information, comorbidities, and performance status that were available from each patient. At the same time, some limitations exist. First, due to the observational nature of the study, the results should only be interpreted within the limitation of a retrospective design. Diagnosis and ascertainment of CVD were dependent on chart reviews. While it is likely that there are undiagnosed cases, the use of medical records is a well-established method to consistently identify CVD outcomes within structured data. Second, the heterogeneity of the study cohort and the lack of a standard therapeutic approach, due to the strong patient and physician preference regarding the implementation of specific treatment modalities, were also limitations of this study. Nevertheless, we believe that such bias would be inherent in any retrospective study and may reflect the reality of clinical practice in which the application of sequential therapies for mHSPC is not standardized. Third, in the majority (87.3%) of patients, the presence of metastasis was determined from imaging studies and was not pathologically confirmed. Therefore, a proportion of our cohort might have harbored non-metastatic disease. Fourth, the possibility of unidentified imbalance in baseline patients and tumor characteristics cannot be overlooked, along with the absence of a formal follow-up protocol, which may potentially confound the results of this study. Lastly, while cancer-specific survival may be considered as the most robust survival endpoint, we chose to use OS as the endpoint, since our study population included patients who were relatively older in age and had multiple comorbidities, in which 34% of the patients had CCI values ≥2. Indeed, as OS is affected by competing risks, we considered that OS may reliably reflect the impact of CVD on survival in real-life cancer care.
A variety of factors influence outcomes in patient with CVD in the setting of underlying cancer. Local treatment with or without metastasis-directed therapy may provide an OS advantage for de novo mHSPC patients without a history of CVD. While this association requires confirmation in a prospectively designed study, patients with PCa with a prior history of CVD may be offered less aggressive treatment options.
Go to :
 XML Download
XML Download