

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The renin-angiotensin system (RAS) is a well-established therapeutic target in the treatment of acute myocardial infarction (AMI). Angiotensin-converting enzyme inhibitors (ACEIs) were the first clinically approved RAS inhibitors based on results from numerous clinical trials involving hundreds of thousands of patients with AMI in the 1990s.12 The current guidelines recommend that ACEIs should be the first choice of RAS inhibitors administered for high-risk AMI patients, including those with heart failure or left ventricular systolic dysfunction, and ACEIs should be considered in all patients in the absence of contraindications.345 However, in the real world, numerous patients may be intolerant to ACEIs, mainly due to having a cough, but also due to hypotensive symptoms, renal dysfunction, or angioneurotic edema.67 Angiotensin receptor blockers (ARBs) were developed to overcome non-ACE pathways and bradykinin breakdown, resulting in increased tolerance in patients with a cough.8 ARBs represent an alternative to ACEIs in patients with AMI who do not tolerate ACEIs.345
A few head-to-head comparison trials of ARBs versus ACEIs91011 and trials of ARBs versus placebo in patients intolerant to ACEIs612 support the alternative use of ARBs instead of ACEIs. However, there were some inconsistent results. Losartan did not satisfy the non-inferiority criterion compared with captopril in AMI with left ventricular systolic dysfunction,9 and telmisartan had no significant effect on the primary outcome compared with placebo in ACEI-intolerant vascular disease patients.6 Several recent studies from the registry also showed inconsistent results for the clinical effect of ARBs in patients with AMI.13141516 In addition, early head-to-head studies included one-third or half of the patients who underwent thrombolytic strategy treatment,910 whereas other studies enrolled less than half of patients who underwent revascularization.61112 Therefore, the objective of this study was to demonstrate the long-term prognosis for the alternative use of ARBs instead of ACEIs in patients with AMI undergoing percutaneous coronary intervention (PCI).
METHODS
Study population
The CardiOvascular Risk and idEntificAtion of potential high-risk population in AMI (COREA-AMI) registry has been described in previous studies.17 Briefly, this registry included patients who were diagnosed with AMI from January 2004 to December 2009, and all of the patients were treated with PCI using stents. The investigators defined AMI as the criteria for the universal definition of myocardial infarction.18
Physicians performed coronary angiography and stent implantation according to standard techniques and the type of the stent chosen was at the operator's discretion. Aspirin or clopidogrel-naïve patients received a loading dose of 250 to 500 mg aspirin and 300 to 600 mg clopidogrel. Periprocedural anticoagulation was administered according to standard regimens. Most of the patients maintained dual antiplatelet therapy at the time of PCI or discharge, and the duration of dual antiplatelet therapy was determined by the physicians. The decision to use glycoprotein IIb/IIIa inhibitors and to perform thrombus aspiration or intravascular ultrasonography was at the operator’s discretion.
Independent research personnel collected clinical and outcome data, and an independent interventional cardiologist assessed angiographic and procedural data. Each patient was followed up during an outpatient clinic visit or contacted by telephone conversation. All of the clinical events were confirmed by source documents and were determined centrally by a committee of the Cardiovascular Center of Seoul St. Mary's Hospital, Seoul, Korea. For the validation of complete follow-up data, information on censored survival data and the causes of death were obtained from the Office of Statistics Korea with the use of unique identification numbers.
Treatment groups and endpoints
The optimal medications, including ACEIs or ARBs, statins, or beta-blockers, were administered depending on the physician's preference. Dose titration and medication changes were performed during follow-up in the outpatient clinic after discharge according to the patient's condition. Independent research personnel collected data for prescription medications at discharge and follow-up. Of the patients enrolled in the registry, 3,667 had adequate prescription data both at discharge and follow-up period during the first year. We excluded patients who were taking ACEIs and ARBs together or who started taking ACEIs or ARBs after discharge. Included patients were divided into 1 of the following 4 groups: 1) the ACEI to ARB group, who received an ACEI at discharge, which was replaced by an ARB during the first year, 2) the ACEI group, who continued to use ACEIs during the first year, 3) the ARB group, who continued to use ARB during the first year, and 4) the no ACEI/ARB group, who did not receive ACEIs or ARBs at discharge or discontinued use during the first year after the index procedure (Fig. 1).
Fig. 1
Study flow chart and treatment groups.
ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker.

The primary endpoint was the composite of cardiovascular death, MI, stroke, or hospitalization due to heart failure. The secondary endpoint was all-cause death. Death by any cardiovascular mechanism, such as sudden death, MI, arrhythmia, heart failure, cerebrovascular, aorta, peripheral artery disease, pulmonary embolism, cardiovascular procedure, or other cardiovascular cause, was considered cardiovascular death.
Statistical analysis
All baseline characteristics are summarized as the mean ± standard deviation for continuous variables and number (%) for categorical variables. Differences between groups were analyzed by using the analysis of variance and Bonferroni test for continuous variables, and the χ2 or Fisher's exact test was used for discrete variables where appropriate. Cumulative incidence rates of clinical events were assessed by Kaplan-Meier estimates and compared using a log-rank test. Cox proportional hazard models were applied to analyze the hazard ratios (HR) and 95% confidence interval (CI) for endpoints.
We performed the multivariate cox model with use the inverse probability weighting (IPW) method. The variables that were significantly different at the baseline or had predictive value were used for the covariate. The propensity score was estimated with multiple logistic regression models. Covariates included in the model were as follows: age, gender, body mass index, hypertension, diabetes mellitus, hypercholesterolemia, smoking, family history of coronary artery disease, previous cerebrovascular accident, atrial fibrillation, clinical presentation, Killip classification, left ventricular ejection fraction, creatinine, renal insufficiency, multivessel coronary artery disease, final thrombolysis in myocardial infarction flow, use of intravascular ultrasound, use of intraaortic balloon pumping, type of stent, systolic blood pressure at admission, diastolic blood pressure at admission, heart rate at admission, statin at discharge, beta-blocker at discharge, and dual antiplatelet therapy at 1 year. To reduce the bias from different hospitals or the year of the index procedure, the participating centers and the year of the index procedure were used as strata (stratum variables).
All analyses were 2-tailed, with clinical significance defined as a P value less than 0.05. Statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) and SPSS software version 20.0 (IBM Co., Armonk, NY, USA).
Ethics statement
This study was conducted in compliance with the Declaration of Helsinki regarding investigations in humans, and the study protocol was reviewed and approved by the Institutional Review Board (IRB) of participating hospitals (Seoul St. Mary's Hospital, IRB No. XC13RIMI0060K). Written informed consent was obtained from each patient when they were enrolled. This registry has been registered on ClinicalTrials.gov (study ID: NCT02385682).
RESULTS
Of the 3,328 eligible patients, ACEIs were prescribed to 1,640 patients at discharge, 826 patients continued to use ARBs, and the other 862 patients did not receive ACEIs/ARBs at discharge or discontinued use during the first year after the index procedure. ACEIs were replaced by ARBs in 816 patients, while 824 patients continued to use ACEIs during follow-up. Among the ACEI to ARB group, 242 patients complained of a cough before the switch, 14 of hypotension, 14 of hypertension, 7 of dizziness, and 9 of other issues. The reason for the switch from ACEIs to ARBs could not be identified in 530 patients. The median time from the index procedure to the medication change from ACEI to ARB was 102 days (interquartile range [IQR], 33 to 226 days).
Table 1 presents the baseline characteristics according to the treatment group. The mean age at index admission was 61.0 ± 12.3 years. The age of ACEI to ARB group was significantly lower than that of the no ACEI/ARB group, and the age of ACEI group was significantly lower than that of the ARB group and no ACEI/ARB group. Three-quarters of patients in the whole population were men. Approximately 60% of included patients were STEMI, and the others were NSTEMI. More than 90% of patients received drug-eluting stents on the culprit lesion. Systolic and diastolic blood pressure during index admission were different between the groups. Blood pressure of the no ACEIs/ARBs group was significantly lower than the other 3 groups, and blood pressure of these 3 groups were not statistically different. More than 80% of patients were prescribed statins and beta-blockers. However, patients in the no ACEI/ARB group were less likely to be given these medications.
Table 1
Baseline characteristics in the crude population according to treatment groups

Data are presented as mean ± standard deviation for continuous variables and absolute numbers (percentage) for discrete variables.
ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker, NSTEMI = non-ST-segment elevation myocardial infarction, STEMI = ST-segment elevation myocardial infarction.
aTotal cholesterol ≥ 200mg/dL; bestimated glomerular filtration rate calculated by Chronic Kidney Disease Epidemiology Collaboration equation < 60 mL/min/1.73m2.
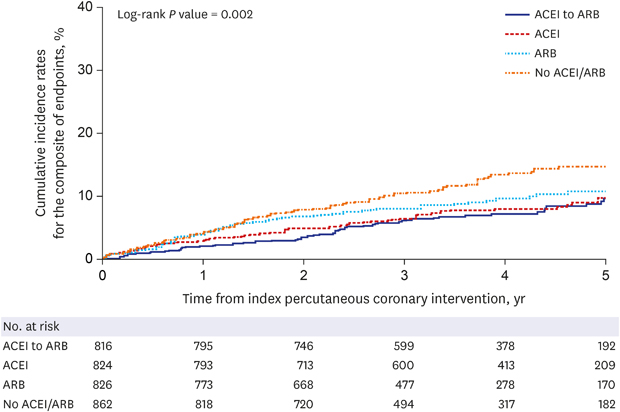
The median duration of follow-up was 1,335 days (IQR, 924 to 1,780 days) in the whole population. Table 2 shows the clinical outcomes according to the treatment groups. Primary composite endpoints were observed in 61 patients (7.5%) of the ACEI to ARB group, in 66 patients (8.0%) of the ACEI group, in 73 patients (8.8%) of the ARB group, and in 102 patients (11.8%) of the no ACEI/ARB group (log-rank P = 0.002). The composite clinical events of the ACEI to ARB group was lower than that of the no ACEI/ARB group and did not differ significantly to that of the ACEI group or that of the ARB group (Fig. 2). Unadjusted hazard ratio and adjusted hazard ratio by using IPW showed consistent results in terms of the primary composite outcome. Cardiovascular death and hospitalization due to heart failure of the ACEI to ARB group were significantly less frequent than that of the no ACEI/ARB group. Although all-cause death seemed to be different between the groups in the crude population, no significant difference in the incidence rate was observed after adjustment with IPW.
Table 2
Clinical outcomes according to treatment groups

Data are presented as absolute numbers (Kaplan-Meier estimates).
CI = confidence interval, ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker.
aFor ACEI to ARB versus each group; bcomposite of cardiovascular death, myocardial infarction, stroke, or hospitalization due to heart failure.
Fig. 2
Kaplan-Meier curves for the composite of cardiovascular death, myocardial infarction, stroke, or hospitalization for heart failure according to treatment groups.
ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker.
The clinical outcome of the ARB group was similar to that of the ACEI group after adjustment (HR, 1.05; 95% CI, 0.88–1.25; P = 0.625). Although the primary composite endpoints of ARB group seemed to be numerically lower than that of no ACEI/ARB group (log-rank P = 0.042), long-term outcomes were not statistically different after adjustment with IPW (HR, 0.90; 95% CI, 0.76–1.06; P = 0.200). Each component of the primary outcome or all-cause death were also not statistically different between the ARB and ACEI group or between the ARB and no ACEI/ARB group after the adjustment (Supplementary Table 1). Additional analysis for the primary outcomes was performed according to the timing of switch from ACEI to ARB. The investigators divided the ACEI to ARB group into 2 groups according to the timing of the medication change. Of the ACEI to ARB group, 332 patients changed medication before 3 months from the index procedure, and the other 484 patients changed medication after 3 months. Clinical events were similar between the groups (HR, 0.92; 95% CI, 0.56–1.53; P = 0.750). Landmark analysis at 1 year was performed to demonstrate the effect of ARBs after switching from ACEIs as most of the patients changed the medications within 1 year. After 1 year, the incidence rates of adverse clinical event were similar to the overall results (Log-rank P = 0.018). The ACEI to ARB group, the ACEI group, and the ARB group showed lower rates of primary endpoint than that of no ACEI/ARB group (HR, 0.62; 95% CI, 0.42–0.93; HR, 0.59; 95% CI, 0.39–0.88; HR, 0.65; 95% CI, 0.43–0.99, respectively), and adverse events of the 3 groups with any RAS inhibitors were not different (Supplementary Fig. 1).
Fig. 3 shows the subgroup analyses in the crude population. The calculated HRs in meaningful subgroups were consistent with the results observed in the overall population. Significant interactions were not discovered between the treatment groups, except for one borderline interaction. The borderline interaction was observed between the ACEI to ARB group and the ARB group in men and women patients (P = 0.049).
Fig. 3
Comparative unadjusted hazard ratios of the composite of cardiovascular death, myocardial infarction, stroke, or hospitalization due to heart failure for subgroups in the crude population according to treatment groups compared to an alternative use of angiotensin receptor blocker.
ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin receptor blocker, NSTEMI = non-ST-segment elevation myocardial infarction, STEMI = ST-segment elevation myocardial infarction.

DISCUSSION
The present study demonstrated that the alternative use of ARBs following initial treatment with ACEIs resulted in similar beneficial effects compared to the continued use of ACEIs. In addition, patients who alternatively used ARBs had a lower incidence rate for the composite of cardiovascular death, MI, stroke, and hospitalization due to heart failure compared to patients who did not use ACEIs/ARBs. On the other hand, the use of ARBs at discharge and thereafter resulted in similar clinical outcomes to the ACEI group, but was not significantly different to no ACEI/ARB group.
Although ACEIs reduce cardiovascular adverse events, ARBs were developed to block angiotensin II produced by non-ACE pathways and they do not inhibit bradykinin breakdown, resulting in increased tolerance for a cough or angioedema. However, in patients with AMI, the current guidelines recommend that ARBs should be considered as an alternative in patients intolerant to ACEIs. There are a number of reasons for the limited recommendation of ARBs in patients with AMI. ARBs could provide a non-inferior, not superior, beneficial effect to that of a proven ACEIs.1011 Moreover, inconsistent results have previously been observed, for example, losartan did not satisfy the non-inferiority criterion.9 ARBs are more expensive, tend to be more hypotensive and cause renal dysfunction according to randomized trials.19 For these reasons, ACEIs should be the first choice of RAS inhibitors, and the primary value of ARBs is in their use as an alternative for patients with AMI who cannot tolerate ACEIs.
In the real world, however, 5%–20% of patients treated with ACEIs have an intolerance to these drugs, frequently due to a dry cough, angioedema, hypotension, hyperkalemia, or renal dysfunction.720 Asians may be more susceptible (20%–50%) to adverse effects related to ACEIs.2122 Thus, in the antihypertensive market of Korea, ARBs are preferred by a factor of more than 10 compared with ACEIs.23 This situation is similar in Japan, but different from that in Western countries in which ACEIs are preferred to ARBs as antihypertensive medications or for patients with coronary artery disease.24252627 A higher frequency of adverse events and physicians' preference may influence the pattern of prescription after discharge in patients of this registry. Of the 1,640 patients who were prescribed ACEIs at discharge, approximately 50% received ARBs at follow-up. In total, 15% of patients complained of a cough resulting in the replacement of ACEIs with ARBs, while the cause of the alternative use of ARBs in 32% of patients could not be determined. Some of the unknown causes of this change from ACEIs to ARBs may be related to undescribed adverse effects, while some patients were likely prescribed an ARB based on the physician's preference of ARBs as an antihypertensive medication.
Data supporting the alternative use of ARBs in patients with AMI who were previously treated with ACEIs are lacking. A placebo-controlled randomized trial showed that candesartan reduced cardiovascular mortality and morbidity in patients with symptomatic chronic heart failure and intolerance to ACEIs.12 On the other hand, telmisartan had no significant effect on the primary outcome in vascular disease patients unable to tolerate ACEIs, although it modestly reduced the risk of secondary outcomes.6 In previous randomized studies, conducted before the early 2000s, approximately half of the patients enrolled were AMI patients, and less than half underwent revascularization. In contrast, all of the patients included in the present registry received revascularization with PCI. In addition, more than 99% of patients were taking dual-antiplatelet therapy at discharge, and statins or beta-blockers were prescribed in over 80% of patients in this study. Our results demonstrated that in this kind of population, the alternative use of ARBs following initial treatment with ACEIs showed a similar clinical impact compared to the continued use of ACEIs and resulted in better clinical outcomes when compared with no use of ACEIs/ARBs.
Data regarding beneficial effects of the alternative use of ARBs in low-risk patients with AMI are insufficient. Although ACEIs should be considered in all AMI patients, the class of recommendation for low-risk patients, such as in those with preserved left ventricular systolic function without hypertension or diabetes, is weaker than that in high-risk patients. Moreover, there has been a paucity of clinical data on AMI treatment with ARBs in low-risk patients or in a particular population. Several recent studies from a registry showed inconsistent results for the clinical effect of ARBs in patients with AMI.13141516 However, the present results may support the beneficial effects of the alternative use of ARBs after replacement of ACEIs in both high- and low-risk patients with AMI. On the other hand, the continued use of ARBs from the index admission demonstrated similar clinical outcomes to the continued use of ACEIs, but also was not significantly different to no use of ACEI/ARB after adjustment with IPW. The treatment of ARBs as the 1st choice of RAS inhibitor seems to be non-conclusive in the present results. Further large-scale nationwide data or randomized trials are required.
Nevertheless, this study had several limitations. First, the study was based on an observational registry, which has inherent limitations. Although the IPW method was performed to adjust for potential confounders, unmeasured variables could not be corrected in the observational database. The second limitation is the underestimation of major adverse cardiovascular events. As we focused on the alternative use of ARBs, the study was designed to analyze eligible patients who had adequate prescription data at discharge and at follow-up. Therefore, most patients who died within the acute period after index PCI may have been excluded. Third, reasons for the replacement of ACEIs with ARBs were obtained by medical records retrospectively, and thus were unknown in two-thirds of patients. In addition, reasons for patients no being prescribed either ACEIs or ARBs were also unknown. Unknown confounders might be associated with physicians’ discretion regarding the use of medications. Another limitation of this study is the class effect. Ramipril was used in most patients, and valsartan, candesartan, and telmisartan were used in more than two-thirds of patients taking ARBs. These results, therefore, may not be directly applicable to other labels of ACEIs or ARBs and should be interpreted with caution. Another limitation was that we could not analyze medication adherence or dose titration.
In conclusion, the alternative use of ARBs following initial treatment with ACEIs demonstrates comparable clinical outcomes to the continued use of ACEIs and is associated with an improved rate of composite cardiovascular events compared with no ACEI/ARB use in patients with AMI undergoing PCI. The alternative use of ARBs maintain the early beneficial effect of ACEIs. Further large-scale nationwide data or randomized trials are required to establish and validate the present results.
 XML Download
XML Download