

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Working status has been identified as a major risk factor of breastfeeding discontinuation and poor lactation practices among workers. Specific interventions to improve education and knowledge of health and lactation in a working mother population helps to improve the health behaviour and attitude. A study in Jordanian women showed that better level of knowledge, education and lactation promotion support at the workplace helps to improve the breastfeeding practices among workers.1 Several studies also found some socio-demographic variables, including education level and knowledge, strongly related to the practice of health behaviours, including lactation practice.234 Similar evidence from Duffy reported that age and education affected healthy life style behaviours among workers.5
Unfortunately, a study in Indonesia showed that only 21.5% of workers have access to proper lactation support at work and only 7.5% of workers benefit from adequate lactation education support/program provided by the employers, which was indicated by the poor support of knowledge improvement initiatives in workers.6 Hence, the prevalence of exclusive breastfeeding among blue-collar workers (manufacture labour) in Indonesia is only 19%, far below national prevalence which was 38%.7
Workers were defined as white-collar workers by the following 14 job titles: administration, management, accounting, business, planning, personnel affairs, human resources, marketing, distribution, inspection, customer service, sales, supporting and international sales. Blue-collar workers were defined as those with other than a white-collar job title.8 A study in Makassar, Indonesia reported that due to lower educational background, blue-collar workers tend to show a lack of knowledge and have improper health behaviour at work.9
This study aimed to evaluate the knowledge, attitude, and breastfeeding practice among white-collar and blue-collar workers in Indonesia and to identify factors associated with breastfeeding practice during working hours.
METHODS
A cross-sectional study was performed in two factories and three government offices in Jakarta, Indonesia from December 2015 to February 2016. Sample size was calculated using single proportion sample formula for a descriptive study that indicated a minimum of 160 subjects required. Inclusion criteria were women workers whose children were between 6 and 24 months old, actively working in the particular factory or office for the last 12 months and agreed to participate in the study by signing the informed consent.
Data collection and statistical analysis
A set of self-administered questionnaires was distributed to obtain data related to demographic, occupational, knowledge, attitude and lactating practices in the workplace. The questionnaire was modified from the Basrowi et al. study,6 after consultation with experts from Division of Occupational Medicine Faculty of Medicine Universitas Indonesia, with reliability test Cronbach's alpha 0.706.
Knowledge on breastfeeding was measured using 11 items of multiple-choice questions format, related to subject's understanding of the definition, perception, and benefits of exclusive breastfeeding to the infants and mothers based on World Health Organization standards, as well as the understanding on government regulation and company's policy related to lactation support and program in the workplace. Attitude was determined by a series of multiple-choice questions and a true/false format, indicating the subject's support, feelings, and responses toward breastfeeding in the workplace, including questions on supervisor and peer influences and supports received by the subject when they were breastfeeding or breast pumping during working hours. Knowledge and attitude scores were considered ‘good’ if the total score was ≥ 80 and ‘not good’ if the score was < 80. This cut-off score is consistent with a similar study which evaluated the health related knowledge level of workers in Indonesia.69
Lactation practice was defined as a breastfeeding behaviour of subject in the workplace during working hours, indicated as a ‘breastfeeding only’ if the subject only directly breastfed the infant at the workplace or went home to breastfeed; ‘breast pumping only’ indicated if the subjects only fed expressed breastmilk in any location in the workplace during working hours; ‘mixed breastfeeding and breast pumping’ indicated if the subject combined the lactating practice by breastfeeding the infant directly and also gave expressed breastmilk during working hours; ‘never breastfeed’ indicated if subject never breastfed nor gave expressed breastmilk during working hours. The location of breastfeeding and/or breast pumping was also identified.
A χ2 test was performed to analyse cross-tabulated data for bivariate analysis between knowledge, attitude, breastfeeding practice and occupation (white-collar and blue-collar worker). A logistic regression model was performed for multivariate analysis of demographic, occupational and outcomes variables related to breastfeeding practice. The statistical analyses were performed using SPSS version 20 (IBM Corp., Armonk, NY, USA). P values < 0.05 were considered to be statistically significant.
RESULTS
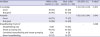
A total of 192 women workers participated in this study with an age range from 20 to 45 years (mean, 31.88 ± 4.39 years). Most of the subjects were blue-collar and factory-based workers (64.6%); the educational level was mainly (62.5%) graduation from junior and high school and 37.5% from university level (Table 1).
Table 1
Demographic and occupational characteristics of the workers

![]()
Breastfeeding knowledge and attitude
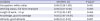
The majority (72%) of blue-collar workers had a lack of knowledge regarding breastfeeding definition, benefits and awareness of policy and regulation of breastfeeding at the workplace, hence indicating as a ‘not good’ of breastfeeding knowledge (Table 2). On the contrary, white-collar workers showed a significantly higher percentage of good knowledge about breastfeeding (55%). However, the level of knowledge in both groups of workers does not reflect the breastfeeding attitude in the workplace. The percentage of white-collar workers that had a good breastfeeding attitude was significantly higher than the blue-collar workers, 72% vs. 57% respectively (P = 0.045).
Table 2
Knowledge, attitude and breastfeeding practice based on subject's occupation
Values are presented as number (%).
OR = odds ratio, CI = confidence interval.
aP value: knowledge and attitude using Fisher's Exact Test; bBreastfeeding practice using Pearson χ2.
![]()
Breastfeeding practice
When the subjects were asked about their lactation practice during working hours, a higher percentage of subjects (72% white-collar and 65% blue-collar) mentioned that they were only breast pumping in the office/factory, while only 9% of the white-collar workers and 15% of the blue-collar workers directly breastfed their infants during working hours by bringing them to the office/factory during lunch-break or going back home if they lived nearby the workplace, although the results were not statistically significant. Nevertheless, more than 10% of subjects in both groups (15% of white-collar and 17% of blue-collar) mentioned that they never breastfed nor pumped breastmilk during working hours.
Table 3 shows that workers who never breastfed or pumped milk at the workplace felt uncomfortable and worried about leaving the job to feed the baby or express milk (44%). Other reasons reported were: inaccessible and inconvenient lactation room in the office/factory (19%), inadequate volume of breastmilk (10%) and not permitted to breastfeed/ breast-pump by their supervisor (6%).
Table 3
Reasons of workers never breastfeeding or breast-pumping in workplace

![]()
The subjects were also asked about the location where they could breastfeed/breast pump at the workplace: 50% mentioned that they were expressing milk in the toilet or bathroom and only 16% were using the lactation room provided in the office/factory. White-collar workers with a higher level of position, reported breast pumping in their own cubicle as this is much more convenient.
Factors associated to the breastfeeding practice
We performed a multivariate analysis to identify variables associated with subject's breastfeeding or lactation practice in the workplace. Table 4 shows that working as a full-timer (P = 0.005) and good knowledge (P = 0.002) were strongly correlated with the lactation behavior and practice among workers.
Table 4
Multivariate analysis of factors associated with subject's lactation practice in workplace
![]()
DISCUSSION
Our study showed that white-collar workers have a higher percentage of adequate/good knowledge about breastfeeding compared to blue-collar workers, and hence had higher percentage of ‘good attitude’ towards breastfeeding. This might be related to the higher education level of white-collar workers. Pender et al.10 found that white-collar workers enrolled in workplace promotion programs were more likely to report a healthy lifestyle. Galtry et al.11 found that being blue collar or lower income generally implies lower skill requirements, less flexibility and even less protective working rights hence affecting the health behavior. According to data from Korea, highly educated women more frequently decide to breastfeed.12 Particularly for the breastfeeding attitude, a study from Malaysia reported that there was a strong correlation between higher education and better knowledge of breastfeeding with the positive attitude and behaviour of breastfeeding among women workers.13 According to this study, the greatest incremental of breastfeeding and lactating practice occurred among women with at least some secondary education. Çiftçi et al.14 also mentioned that there is a positive effect of women who have an increased awareness and knowledge of the benefits of breastmilk, resulting in a higher frequency of breastfeeding. Data from Indonesia confirmed this finding.15
The relationship between knowledge and attitude towards breastfeeding are also reported in studies from Ethiopia,16 Nepal,17 Tunisia,18 and Tanzania,19 all indicating that mothers who have an adequate knowledge about breastfeeding have a higher likelihood or probability for exclusive breastfeeding.
However, this study also found that despite the high percentage of inadequate knowledge about breastfeeding among blue-collar workers, this group still had a high percentage of positive attitude towards breastfeeding. A study in Taiwan reported that intention or knowledge alone is not sufficient to overcome barriers to breastfeeding.20 A study in Nigeria founded that there was an average decrease in breast feeding duration of 3.2 and 6.6 months correlating with mother's education to primary and secondary levels, respectively, compared to mothers with no education.21 This finding is similar with the finding of our study that the level of education and knowledge will not necessarily determine the attitude of working women to breastfeed or breast pump in the workplace.
There were numerous influencing factors including the support of adequate lactation facilities and programs at workplace that potentially improve lactation practices among women workers. The Indonesian government issued a Joint Regulation between the Ministry of Women Empowerment, Ministry of Labour, and the Ministry of Health to promote and protect working mothers to breastfeed and pump milk at the workplace.22 The Government Regulation on Exclusive Breastfeeding from 2012 obliges every citizen, including the employers, to promote the success of exclusive breastfeeding. Every workplace mandatory has to provide a dedicated lactation room in the workplace with standardized facilities. The Ministry of Health issued in 2013 a technical guideline about the presence of a lactation room at the workplace.2324
Several studies in Indonesia have suggested that besides knowledge, a lactation counsellor at work, lactation facilities and support by peers would be critical and hence could help working mothers continue breastfeeding and have a positive breastfeeding attitude.252627 Family support also plays an important role.6 These factors are key to potentially help mothers to have positive attitude of breastfeeding despite the lower and inadequate knowledge of breastfeeding. Our study showed that employed mothers in a factory are living in a different environment, with inadequate access to health promotion support and information, including lactation support.
Another important finding of our study is the lactation or breastfeeding practice, the reasons to not breastfeed and the location of breastfeeding in the workplace. In this study, 15% of white-collar workers and 17% of blue-collar workers never breastfeed during working hours, for three main reasons; i.e., feel hesitant to take a break during work, an uncomfortable lactation room, and not allowed by the supervisors. Studies showed that a dual role of being a lactating mother and an employee at the very same time put them in a difficult situation and brings potential conflict in their daily life.28 In many situations, an employed mother tends to sacrifice the lactation/breastfeeding role in order to pursue career or to meet the job's target. This is definitely an unfortunate situation for working mothers with infants, because it will affect the health of both mothers and infants.
Although the Indonesian government had issued a series of breastfeeding protection policies at the workplace, such as the Joint Regulation on Promoting and Protecting Breastfeeding at Workplace year 2008 and the Ministry of Health Regulation Number 15/2013 with a technical guideline for a dedicated lactation room and facilities at the workplace, only 21.5% of the women workers had access to adequate lactation facilities in the workplace and only 7.5% of the workers benefitted from breastfeeding promotion support during working hours.6 New data on breastfeeding from 2017 are available, sowing the exclusive breastfeeding prevalence stratified by working/non-working mothers and by provinces, in which the percentage was not significantly different compare to previous Demographic Health Survey (DHS) - 2013–2014, without further analysis on the ‘reason why’ and other predisposed factors. We report novel findings regarding knowledge, attitude and lactation practice among Indonesian working mothers with a detailed comparison between blue-collar and white-collar workers, which was never reported for Indonesia. The impact of government policy provides much more support compared to 10 years ago, as reported in the DHS. However, the impact of this policy was not fully analyzed at the level of the work place (implementation at the workplace, perspective of the employer, and perspective of workers towards company supports).
In this study, we report the impact of this policy comparing labor and office workers. Hence, the information reported in this study is quite important because we provide evidence-based insights to employers and government, including a recommendation of potential breastfeeding promotion intervention and support in workplace, and future research.
A study from the USA reports that only 3% of the companies have written policies on breastfeeding at work, even though the majority of companies allow women to express breast milk at the workplace. Only 22% of the companies allowed breastfeeding in the company premises and only 32% provided a designated room solely for breastfeeding or breast pumping.29 Chen et al.20 in Taiwan also found that even if the employer provided a lactation room and allowed an hour break for breast milk pumping, workers found it difficult; and it also could take up to 10–15 minutes to travel between the worksite and the lactation room. This might explain the finding of our study why there is still a large number of workers that decided to not breastfeed during working hours and that 50% of the workers decided to pump at the toilet or bathroom instead of the lactation room.
The perception of workers, managers/supervisors and employers towards productivity is another aspect. In our study, 42% of the workers who decided to not breastfeed or pump during working hours mentioned that they felt hesitant to leave their work and 6% of the workers were not allowed by their supervisors. Tsai30 found that 51.1% of women workers assumed that taking a break for breast pumping two times during working hours could lower their work productivity.
From the employer point of view, managers and employers consider that breast pumping during working hours might hamper productivity and affect working performance. A survey found that most employers would be willing to institute breastfeeding support at work, although they saw no benefit to support breastfeeding.31 Blue-collar workers have their own difficult circumstances in participating in worksite health promotion programs due to the lack of social support by the supervisor. In order to keep the production lines moving, supervisors may refuse to allow workers to attend programs during company time.32 Group leader and the manufacturer's performance bonus systems may reduce the willingness of women to breastfeed at the workplace. If a group leader disagrees with breastfeeding but the worker continues to breast pump during work hours, it will affect her work performance and bonus.20 Overall, employers do not prioritize providing breastfeeding support at the workplace.33
Based on multivariate analysis, our study found that the working status and level of knowledge are key variables determining the subject's lactation practice. This was reported in the systematic review by Dinour et al.,34 suggesting that providing a lactation space was the most common employer-based support accommodation studied, followed by breastfeeding breaks and comprehensive lactation support programs targeting the knowledge improvement of lactating workers. Mothers report multiple barriers to breastfeeding upon return to work, such as work schedule flexibility and program support in workplace.35
Involvement of a policy maker in the company and a regular promotion program aimed to improve education and breastfeeding knowledge among women workers were put in place to increase lactation practice.36 A workplace-based lactation promotion model, i.e., policy and regulation, facility, education, and human resources are key components to achieve successful breastfeeding and lactation in the workplace.37
The findings related to the profile of breastfeeding knowledge and attitude between white-collar and blue-collar workers in Indonesia are considered as the strength of this study, as to our knowledge such data had never been reported. The reasons and preferred location of lactation during working hours were also a novel finding and provides significant insight for future improvement of breastfeeding policy. However, a major limitation of this study is that it was designed as a cross-sectional study with a self-administered questionnaire and no factor analysis. Therefore, the potential for bias cannot be excluded.
Breastfeeding education, knowledge related to its benefits and support to working mothers are key priority as they all strongly correlate to the breastfeeding attitude and practice in the workplace. The blue-collar workers would need more attention in such supports, as the complexity of job and education and/or knowledge level are factors associated with inadequate breastfeeding attitude and practice. However, advocacy about the role and understanding of employers, managers, and supervisors in providing breastfeeding facilitation and program support were also critical, not only because it is mandated by government regulation but it is also important to the health of workers.
 XML Download
XML Download