

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Dens invaginatus (DI), also known as dens in dente, is a dental anomaly in which a tooth-like structure is found within a tooth [1]. This developmental anomaly is thought to result from invagination of the enamel organ into the dental papilla before calcification [1].
The widespread classification of DI was described by Oehlers in 1957 [2]. In type I cases, partial invagination is confined to the crown of the affected tooth. In type II cases, partial invagination extends into the root, beyond the cementoenamel junction. These lesions remain within the anatomy of the root without communication with the periodontal ligament (PDL). In type III cases, complete invagination extends through the root and communicates with the PDL. Complete debridement of the root canal space is hindered by the invaginated structure in patients with type II and III DI [2].
Combinations of DI and other anatomical variations, such as gemination, fusion, talon cusp, peg lateralis, macrodontia or microdontia, taurodontism, and dens evaginatus have been reported [3456789]. In addition, DI has been reported in association with hypodontia, dentinogenesis imperfecta, ameloblastoma, odontome, and supernumerary teeth [10111213].
The prevalence of DI has been reported from 0.3% to 10% [14]. DI is most frequently seen in permanent maxillary lateral incisors, followed by maxillary central incisors [14]. However, this anomaly is rare in the mandibular area. One study using cone-beam computed tomography (CBCT) in a Turkish population reported that a 1.0% prevalence of DI in mandibular teeth, while that of maxillary teeth was 9.67% [15]. This article presents a case of bilateral DI involving the maxillary incisors along with canal calcification of general dentition.
CASE REPORT
A 24-year-old female patient visited the Department of Conservative Dentistry with the complaints of swelling, recurrent pus discharge, and discoloration of the upper left incisor. A local dental clinic referred her to our specialist clinic due to a root anomaly. Clinical examination of the maxillary left lateral incisor showed grayish discoloration, insensitivity to percussion, and no mobility. The palato-gingival groove was examined, and the periodontal probing depth was within the normal range. Six days before presentation, a coronal access cavity into the pulp chamber had been prepared and sealed with temporary material at the local clinic (Figure 1A). Periapical X-ray of tooth #22 showed a periapical lesion with a diameter of approximately 8 mm and Oehlers' type II DI (Figure 1B). The patient had no history of trauma, and her medical history was noncontributory. Tooth #22 was diagnosed with pulp necrosis and chronic apical abscess. In addition, a periapical x-ray revealed DI of the maxillary central and lateral incisors bilaterally (Figure 2A). The anatomic form of tooth #22 was similar to that of tooth #12. Whereas both maxillary lateral incisors had lingual pits, the maxillary central incisors had no anatomic variations (Figure 1A). Generalized pulp stones were identified in the bilateral maxillary canines, first and second premolars, and in the bilateral mandibular incisors, canines, and first premolars by panoramic and periapical X-rays (Figure 2). Tooth #46, which was previously treated with a root canal and restored with a full-coverage gold crown, was diagnosed with chronic apical periodontitis. Except for teeth #22 and #46, all teeth responded to an electrical pulp test and showed normal periapical status. Root canal treatment of tooth #22 was planned, followed by non-vital tooth bleaching.
 | Figure 1Maxillary anterior teeth at the initial examination. (A) A clinical photograph of the maxillary anterior teeth, (B) a periapical X-ray shows dens invaginatus of teeth #11, #21, and #22 as well as periapical radiolucency around the root apex of tooth #22.
|
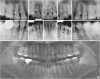 | Figure 2Periapical and panoramic X-rays of maxillary and mandibular teeth. (A) Dens invaginatus, in the maxillary incisors and the maxillary canines and premolars present root canal calcification and/or pulp stones (arrows), (B) 6 anterior teeth and the first premolars in the mandibular arch show root canal calcification and/or pulp stones (arrows), (C) a panoramic X-ray reveals that generalized root canal calcification and pulp stones.
|
The temporary filling material in the access cavity was removed, revealing a foul odor from the pulp chamber. After cleaning the coronal access, a DG-16 endodontic explorer (Hu-Friedy Mfg Co., Chicago, IL, USA) was used to locate the orifices. An intracanal-invaginated mass was removed with ultrasonic tips (ProUltra Endo tip, Dentsply Tulsa Dental, Tulsa, OK, USA) (Figure 3A) under an operating microscope. Thereafter, patency of the root canal was achieved, and working length was determined using a size 15 K-file (Mani, Tochigi, Japan) (Figure 3B). The root canal was enlarged to an apical size of #50 and copiously irrigated with 3.5% NaOCl via a side-vented 27G needle. Calcium hydroxide dressing was used during the 1-week inter-appointment period (Figure 3C). The root canal was obturated with gutta-percha and AH 26 sealer (Dentsply DeTrey GmbH, Konstanz, Germany) using the continuous wave of condensation technique (Figure 4A). After resin-modified glass ionomer was applied upon the root canal filling material, non-vital bleaching was performed using 3% hydrogen peroxide and sodium perborate (Figure 5A). The patient returned every week to change the bleaching agent. After 2 visits, there was a drastic change in the tooth color. The cavity was irrigated, and the bleaching agent was washed out. At 10 days later, the cavity was restored with composite resin. The patient was regularly followed to check for color stability and complications (Figures 4B–4D and 5B). After 13 months of follow up, a periapical radiograph showed that the periapical lesion in tooth #22 had decreased in size and showed no sign of external cervical resorption (Figure 4D).
 | Figure 3Periapical radiographs during root canal shaping of tooth #22: (A) the intracanal-invaginated structure was removed using ultrasonic tips, (B) determination of working length, (C) placement of the inter-appointment dressing.
|


DISCUSSION
In the present case, non-surgical endodontic treatment was used to faultlessly manage a root canal anomaly with chronic apical abscess on tooth #22. An ultrasonic instrument was used to gain straight line access to the apex with the aid of magnification. Removal of an invaginated structure during root canal shaping of a tooth with type II DI has been described in previous case reports [1617]. Although we used intraoral radiography for root canal treatment, CBCT is recommended when managing severe types of DI [18].
In the present case, the bilateral upper incisors had DI. According to previous case reports, important clinical clues to detect DI include dilated or larger crown morphology than the contralateral tooth, a deep pit at the lingual or occlusal surface, pronounced cingulum for the maxillary canines, and talon cusp for the mandibular incisors [81920212223]. However, in the present case, DI of the maxillary central incisors was incidentally identified on periapical x-rays; the pulpal status was healthy, and no abnormality was found in the external crown, except that the maxillary lateral incisors had lingual pits.
Management of DI varies depending on the pulpal and periapical status and the complexity of the anatomy. For Oehlers' type I or II cases with healthy pulp, appropriate prophylactic procedures should be performed. An invagination at the lingual or occlusal surface of the tooth should be treated by acid-etching, followed by sealing of the pit using flowable composite [724]. If pulpal necrosis is evident, a root canal treatment should be performed. Prior studies have reported removal of an invaginated mass during root canal treatment [1617]. Management of Oehlers' type III lesions is more complex. Peri-invaginatus periodontitis is a condition in which the tissue within an invagination becomes infected [212526]. Treatment of a tooth with peri-invaginatus periodontitis requires root canal treatment of the invagination. Schwartz and Schindler [22] reported a case in which invagination was treated with a root canal separate from the main canal. Other cases in which invagination had close proximity to the main canal used root canal treatment of the whole root canal system even when the tooth showed a positive response to a vitality test [212627]. If the invagination communicates with the PDL space or the blunderbuss opening to the PDL space, root canal filling with mineral trioxide aggregate can be useful [2023282930]. Surgical endodontics were used to seal the invagination apically in several cases [28313233]. Chaniotis et al. [34] reported a case of a mandibular lateral incisor with DI in which the malformed root was removed using a diamond bur after root canal treatment.
CONCLUSIONS
In conclusion, the exact etiology of DI remains uncertain, and the prevalence of DI varies depending on the studied subject and region. Because teeth with DI are prone to pulpal disease, regular clinical and radiographic examinations in at-risk patients are advisable. Clinicians should understand the anatomy and apply modern endodontic technologies such as an operating microscope and ultrasonic instrument.
 XML Download
XML Download