

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Japanese Society of Hypertension (JSH) has published ‘The JSH Guidelines for the Management of Hypertension in 2019,1) aiming for more effective prevention of hypertension-related organ damage and cardiovascular events for Japanese patients with hypertension.
The prevalence of hypertension in most Asian countries has been increasing because of social and Westernized lifestyle changes. The population in Japan is aging faster than anywhere else in the world. According to the National Health and Nutrition Survey 2016,2) the prevalence of hypertension is 60% for men and 41% for women for those aged 40–74 years, and 74% for men and 77% for women in those aged ≥75 years. For most Asian populations, the risk of stroke is higher than that of coronary artery disease (CAD). Hypertension is one of the most widespread and powerful risk factors for cardiovascular disease (CVD) events and age-related diseases such as vascular dementia, heart failure (HF), and chronic kidney disease (CKD),3)4)5) and its role in global health and that of the Japanese is of great interest. Furthermore, the public health concerns regarding these diseases are urgent matters that must be understood and addressed immediately.
The new JSH 2019 guidelines were prepared considering the current background and conditions for the aging population in Japan. Although there are some discrepancies between the JSH 2019 guidelines and those from other countries, the background and conditions in each country are different, and these need to be discussed and understood.
JAPANESE SOCIETY OF HYPERTENSION 2019 GUIDELINE DEVELOPMENT
The JSH 2019 guidelines were compiled by 44 writing members and 74 document reviewers who were officials of the JSH and specialists in stroke, pregnancy-induced hypertension, endocrinology, dementia, dialysis, and medical economics. Systemic review members were recommended by the writing members, and 43 members were selected. In addition, 22 liaison members were selected based on recommendations from 22 affiliated societies, and evaluation was performed according to Appraisal of Guidelines for Research and Evaluation II criteria.6) Five advisors were chosen.
The JSH 2019 guidelines evaluated 17 clinical questions for systemic reviews and made recommendations based on evidence level and recommendation grade. If there was not enough evidence, 9 questions were evaluated and answers were determined from recent materials. Data on clinical questions and questions in the literature were collected by searching on PubMed, EMBASE, the Cochrane library and Ichushi-Web, based on publication dates up to the end of 2017. Final recommendations were determined after repeated rounds of voting by e-mail (the Delphi method).
BLOOD PRESSURE MEASUREMENT
There is no change to the methods of measurement from the 2014 JSH guidelines. Recent studies reported that automated office blood pressure (AOBP) might be able to eliminate the white-coat effect.7) Therefore, AOBP was discussed and the possibility of its use was evaluated among the JSH 2019 guidelines team.
AOBP for blood pressure (BP) measurement was first recommended by Canadian hypertension guidelines in 2011.8) Data from the systolic BP intervention trial (SPRINT) study showed that achievement of strict systolic BP (SBP) control (<120 mmHg) based on AOBP measurement reduced the incidence of cardiovascular events and total mortality.9)10) However, recent studies reported discrepancies between AOBP and 24-hour ambulatory BP monitoring (ABPM).11)12) A recent JSH working group conducted a comparison study of office BP, unattended AOBP, and home BP, and showed low correlations between these methods and a wide range of differences. This suggests that AOBP cannot be used as an alternative to home BP.13) Thus, the JSH 2019 guidelines did not recommended AOBP due to concerns about its clinical feasibility and the relationship between AOBP and home and ABPM. In addition, the JSH 2019 guidelines decided against recommendation of mercury sphygmomanometers because the manufacture and export/import of mercury sphygmomanometers will be prohibited from 2021 under the Minamata Convention on Mercury.14)
BLOOD PRESSURE CATEGORIES
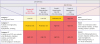
Comparison of BP categories between the JSH 2014 and 2019 guidelines are shown in Table 1.1)15) The definition of ‘normal BP’ in adults was changed. The terms ‘optimal,’ ‘normal,’ and ‘high-normal BP’ in the 2014 guidelines were replaced with ‘normal,’ ‘high-normal,’ and ‘elevated BP’ in the 2019 guidelines. In addition, diastolic BP (DBP) cut-off values for high-normal and elevated BP were chosen as <80 and 80–90 mmHg, respectively. These changes were based on data from observational studies in Japan16)17)18) and Europe, or the United States (US),19) which showed that the incidence of CVD in individuals with office BP of 120–129/80–89 mmHg was higher than in those of with office BP of 120/80 mmHg.
Table 1
BP classification in adults based on the JSH 2014 and 2019 guidelines

Changes from 2014 to 2019 are shown in red. Source: Generated from Umemura et al.1) and Shimamoto et al.15)
BP = blood pressure; DBP = diastolic blood pressure; GL = guideline; JSH = Japanese Society of Hypertension; SBP = systolic blood pressure.
![]()
In the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines,20) stage I hypertension was defined as BP 130–139/80–89 mmHg. Based on data from studies in Japanese patients21)22) it was decided to make no changes to stages of hypertension based on office and home BP values.
RISK STRATIFICATION FOR PROGNOSIS ASSESSMENT
Hypertension is a primary risk factor for CVD. Stroke mortality rates in Japan have markedly decreased over the past 50 years, but stroke-related mortality and morbidity are still more common than those due to acute myocardial infarction.23)24) In contrast, CVD risk recommendations in the European and US guidelines are based on the absolute risk of CAD in cohort studies.25)26) As shown in Figure 1, the risk of stroke and CVD in the JSH 2019 guidelines was assessed based on studies in Japanese patients. Recent Japanese cohort studies have indicated increased rates of CVD, CVD history and CVD risk factors, organ damage, and/or elevated BP (130–139/80–89 mmHg).27)28)29)30) The risk factors were male sex, smoking, diabetes mellitus, dyslipidemia, CKD, and obesity. In addition, the presence of atrial fibrillation (AF) as a comorbidity contributes greatly to the onset of stroke.31) The existence of AF as a related disease has been adopted by the JSH 2019 guidelines because AF contributes greatly to the onset of stroke.
 | Figure 1Cerebro- and CVD risk stratification based on clinic BP based on the JSH 2014 and 2019 guidelines.Changes from 2014 to 2019 are shown in red.
BP = blood pressure; CKD = chronic kidney disease; CVD = cardiovascular disease; GL = guideline; JSH = Japanese Society of Hypertension.
*The prognostic factors used for stratification are BP, age (≥65), sex (man), dyslipidemia, smoking, history of cardiovascular diseases (cerebral hemorrhage, cerebral infarction, myocardial infarction), non-valvular atrial fibrillation, diabetes mellitus and CKD with proteinuria.
|
TARGET BLOOD PRESSURE
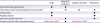
The target threshold in the JSH 2019 guidelines was lowered by 10 mmHg (Table 2). Briefly, target office and home SBP/DBP for adults aged <75 years are now <130/80 and <125/75 mmHg, respectively. Corresponding targets in those aged ≥75 years are 140/90 and 135/85 mmHg, respectively. In older patients with concomitant diseases, the target is <130/80 mmHg, if tolerated by the patient. The same target is also recommended in the presence of CAD. The updated target office BP for adults aged <75 years is based on new evidence from the SPRINT study,9) Cardio-Sis,32) Heart Outcomes Prevention Evaluation-3 (HOPE-3),33) and a systematic review/meta-analysis.34) In elderly patients aged ≥75 years who can visit outpatient clinics without any assistance, target office BP is <140/90 mmHg due to the risk of adverse events such as renal dysfunction when SBP is <130 mmHg.
Table 2
Target SBP and DBP in the JSH 2014 and 2019 guidelines

CKD = chronic kidney disease; DBP = diastolic blood pressure; JSH = Japanese Society of Hypertension; SBP = systolic blood pressure.
*Among treatment-naïve individuals with office blood pressure 130–139/80–89 mmHg, lifestyle modification is started or reinforced for low-risk or moderate-risk cases, and measures including start of antihypertensive treatment are taken for high-risk cases (if their blood pressure is not reduced by lifestyle modification lasting for approximately 1 month or longer) with a final target set at less than 130/80mmHg. If antihypertensive treatment has already been started and blood pressure is 130–139/80–89mmHg, lifestyle modification is reinforced for low-risk or moderate-risk cases and measures including reinforced antihypertensive treatment are taken for high-risk cases, with a final target set at less than 130/80 mmHg. †Proteinuria is judged as positive if protein level in random urine sample is 0.15 g/gCr or more. ‡In case where the goal of antihypertensive treatment is usually set at less than 130/80 mmHg considering comorbidities or other factors, achieving the goal of less than 130/80 mmHg should be attempted even in older patients (aged 75 and over) if tolerable. Care needs to be taken of the risk for excessive hypotensive effects both during and after the process of achieving the goal of antihypertensive treatment. The judgment of excessive hypotensive effects should take into account the features of individual cases since it can vary depending on not only the achieved level of blood pressure but also the magnitude or rate of blood pressure reduction and the condition of individual cases.
![]()
The target home SBP/DBP was set by lowering values by 5 mmHg compared with office BP based on the results of Ohasama35) and HOMED-BP36) studies. From our recent prospective trial, the HONEST study,37)38)39)40) morning home SBP of <125 mmHg was associated with minimum CVD risk, as determined regression analysis, suggested that further reductions in BP might be beneficial.
ANTIHYPERTENSIVE DRUG SELECTION
Lifestyle modifications should be recommended at a BP threshold of 130/80 mmHg because these are important for preventing hypertension, before and after antihypertensive drug therapy, in individuals with high-normal BP or above.41) For high-risk patients with hypertension, antihypertensive treatment should be started early. Five classes of antihypertensive drugs, including calcium channel blockers (CCBs), angiotensin receptor blockers (ARBs), angiotensin converting enzyme (ACE) inhibitors, diuretics and β-blockers, have been shown to prevent the occurrence of CVD.28)42)43) Appropriate antihypertensive drugs should be selected considering compelling indications, contraindications, conditions that require the careful use of drugs, and the presence or absence of complications. The compelling indications for antihypertensive agents were updated in the JSH 2019 guidelines compared with the 2014 version (Table 3).1)15) Briefly, in HF patients with decreases left ventricular systolic function, low-dose ARB or ACE inhibitor, β-blocker or thiazide diuretic are recommended. In patients with CKD, and ARB or ACE inhibitor is recommended as first-line therapy rather than a CCB or thiazide diuretic.
Table 3
Conditions for which major antihypertensive drugs are indicated
Changes from 2014 to 2019 are shown in red. Source: generated from Umemura et al.1) and Shimamoto et al.15)
ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker; CCBs = calcium channel blockers; CKD = chronic kidney disease; LVEF = left ventricular ejection fraction.
*Administration should be started at a low dose, and the dose should be gradually increased carefully; †Caution is needed in patients with coronary spastic angina; ‡Non-dihydropyridine agents.
![]()
Contraindications and requirements for careful administration were also updated in the JSH 2019 guidelines (Table 4).1) New contraindications include bradycardia for CCBs, pregnancy for ARBs/ACE inhibitors, and asthma and severe bradycardia for β-blockers. New criteria for careful administration are obstructive pulmonary disease and peripheral arterial disease for β-blockers.
Table 4
Contraindications and conditions requiring careful drug administration

Source: Umemura et al.1)
ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker; CCB = calcium channel blocker.
*As a rule, ARBs/ACE inhibitors are contraindicated for patients with bilateral renal artery stenosis.
![]()
PERSPECTIVES FOR ASIAN MANAGEMENT OF HYPERTENSION
Asian characteristics
The diagnostic definition of hypertension in new ACC/AHA guideline had a large impact in other countries. However, the Japanese, Korean and European guidelines have not updated their definition (Table 5). The 2017 ACC/AHA guidelines gave substantial weight to the SPRINT study findings.9) However, we felt that the evidence for the change was insufficient, and that more evidence is required in patients with BP 130–139/80–89 mmHg to inform future guidelines. In addition, not enough Asian patients were included in SPRINT study to make these data applicable to the specific local population. Given that the characteristics of Asian hypertensive patients are different to those of Westerners,44) Asian evidence is required on which to base Asia-focused guidelines.
Table 5
Classification of office BP levels and definition of hypertension in the Japanese, Korean, European, and United States guidelines

ACC = American College of Cardiology; AHA = American Heart Association; BP = blood pressure; DBP = diastolic blood pressure; ESH = European Society of Hypertension; JSH = Japanese Society of Hypertension; KSH = Korean Society of Hypertension; SBP = systolic blood pressure.
![]()
To improve the management of hypertension and organ protection for “zero” CVD events in Asia, we have initiated the Hypertension Prevention and Cardiovascular Outcomes in Asia (HOPE Asia) Network, with 3 initiatives as follows: 1) To know the evidence up until now, 2) To achieve consensus, and 3) To conduct clinical studies on hypertension and its management.45)46)47)48)49)50)51)52)
Home blood pressure-guided approach
There is a growing body of evidence that home BP is a better predictor of CVD events than office BP.37)38)39)40)53)54) In particular, morning home BP is more important than evening home BP in determining CVD risk. A home BP monitoring (HBPM)-guided approach is an important recommendation, and use of this out-of-office BP monitoring (BPM) tool could be disseminated and facilitated using health information technology.55)56)
The Asia BP@Home study investigated the characteristics of hypertension and CVD using HBPM in Asian populations (NCT03096119).57)58) The Asia BP@Home is a prospective, multicenter, non-interventional study designed to collect home BP data in patients with hypertension. We enrolled 1,443 treated patients from 15 Asian specialist centers in 11 countries/regions between April 2017 and March 2018. The findings showed that home BP is relatively well-controlled at hypertension specialist centers in Asia. However, almost half of all patients remained uncontrolled for morning BP according to new guidelines, with significant country/regional differences.58) Strict home BP control should be beneficial in Asian populations. Therefore, the Asia BP@Home study findings are important to facilitate development of health policies focused on reducing cardiovascular complications in Asia. We hope the results of this study will contribute to future Asian guidelines.
New blood pressure monitoring technology
There has been ongoing research and development of various BPM devices over the last 10 years. Due to the fact that masked hypertension is associated with a similar or worse prognosis to sustained hypertension, the detection and management of masked hypertension are residual unmet needs.59)60)61) We have developed nocturnal HBPM, and J-HOP study data showed that uncontrolled nocturnal hypertension detected using nocturnal HBPM predicts risk for future CVD events independently of office, morning and evening home BP.62)63)
Wrist-type HBPM and wearable BPM devices are also being developed and studied, and have been shown to be of sufficient quality for use in clinical practice based on validation studies.64)65)66) These devices could be used to detect masked daytime and nocturnal hypertension without sleep disturbance. Hypoxia-trigger nocturnal BPM and beat-by-beat continuous BPM devices are still the subject of research.67)68)69)
BP variability, including morning BP surge and abnormal nocturnal BP dipping status, is a risk factor for CVD independently of 24-hour BP.70)71) As a result, we have developed ABPM technology equipped with an actigraph, thermometer and barometer to evaluate the BP variability response to physical activity, temperature, atmospheric pressure triggers.72)73)74) Using this technology, we can calculate the new indicators such as actisensitivity and thermosensitivity, etc, which could be detected using an information and communication technology (ICT)-based system that collects serial home and ambulatory BP data from individuals along with information on environmental factors such as room temperature, humidity, and pressure. It is well-known that there is significant seasonal variation of BP, especially morning BP, and CVD events.75)76) Actisensitivity is exaggerated in winter compared with summer,73) which may be a contributing factor to increased winter rates of CVD.
Other potential blood pressure-lowering therapies
Sodium-glucose co-transporter-2 inhibitors reduce home and 24-hour ambulatory BP values in diabetic patients with nocturnal hypertension77)78) and an orexin receptor antagonist may modulate BP variability in hypertensive patients with insomnia.79) Renal denervation is also a promising treatment for the hypertensive patients to reduce 24-hour BP, including nocturnal and morning BP.80)81) Due to the fact that nocturnal and morning hypertension are more common in Asians than in the Westerners,82)83) these treatments might be particularly relevant for Asian patients with hypertension.
CONCLUSION
Several decades of review and guidelines in Japan, Korea, Europe, the US and elsewhere have contributed to clear improvements in CVD. However, there are many challenges and little evidence for personalized medicine. In the future, we believe that further progress and development of guidelines will be facilitated by the analysis of clinical big data, including real world data and individual serial data using the ICT platform to facilitate “anticipation medicine” for the management of hypertension.80)84)
 XML Download
XML Download