

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The number of revision hip arthroplasties has been increasing over the past 20 years12) with the increase in the incidence of primary total hip arthroplasty (THA).3) In some revisions, well-fixed femoral stems should be removed because of the incompatibility with bearing materials, periprosthetic joint infection, or damage of trunnion. The removal of a well-fixed stem is challenging, and thus several surgical techniques have been developed. Since introduced by Younger et al.,4) the extended trochanteric osteotomy (ETO) has been widely used to facilitate exposure and removal of the stem.5) However, this technique has been associated with several complications including intraoperative femoral fracture,6) weakness of the abductor mechanism, trochanteric fracture, and postoperative stem loosening.789)
In 2003, the anterior cortical window technique was introduced as a method that provides solutions to such problems.10) This technique allows for easy removal of a well-fixed femoral stem or cement mantle and stable fixation of a new stem. Moreover, the osteotomy can be easily fixed with several cerclage wires.11121314) Therefore, we hypothesized that the anterior cortical window technique would be an effective method that causes less damage to the host bone in revision surgery. In this study, we investigated intraoperative and postoperative complications, radiological and clinical results (such as patient-reported outcome and abductor deficiency), and survivorship of revision THA performed using an anterior cortical window at a minimum follow-up of 10 years.
METHODS
Patient Selection and Demographics
Sixty-nine consecutive patients (75 hips) underwent revision THA with use of the anterior cortical window technique at our institution from May 2003 to April 2006. Among the 69 patients, 14 patients (14 hips) were lost to follow-up, and five patients (five hips) died of causes unrelated to revision surgery before the minimum follow-up of 10 years. The remaining 50 patients (56 hips), who were followed up for 10 to 13 years (mean, 11.5 years), were included in this study (Fig. 1).
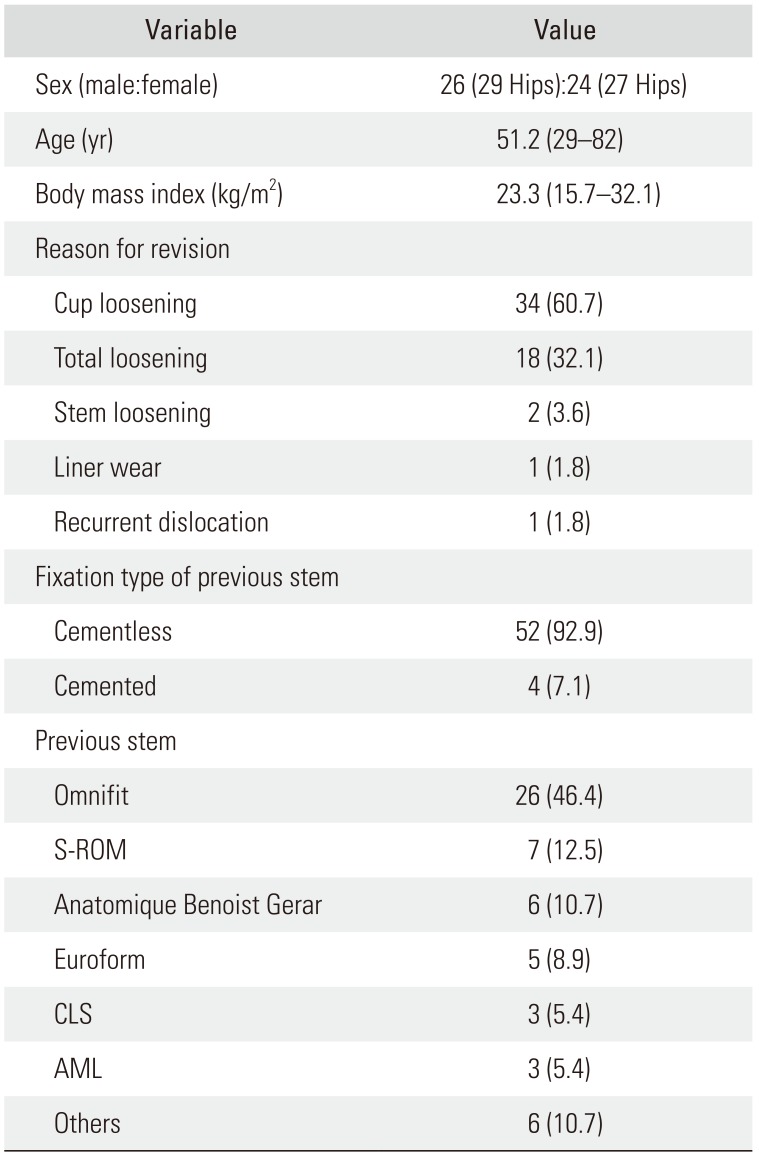
There were 26 men (29 hips) and 24 women (27 hips), and their mean age at the time of revision THA was 51.2 years (range, 29 to 82 years). Their mean body mass index was 23.3 kg/m2 (range, 15.7 to 32.1 kg/m2). Forty-six patients (52 hips) had cementless stems, and four patients (four hips) had cemented stems. Mean interval between previous hip arthroplasty and the revision THA was 10.8 years (range, 6.8 to 18.7 years). Reasons for revision surgery were cup loosening in 34 hips, loosening of cup and stem in 18 hips, stem loosening in two hips, liner wear in one hip, and recurrent dislocation after THA in one hip. Although the most common reason for revision was cup loosening, previous stems and femoral heads had to be revised as well as the acetabular cup and liner because scratches of the metallic femoral head were found during revision and new femoral heads were not compatible with previous stems (Table 1).
Surgical Technique
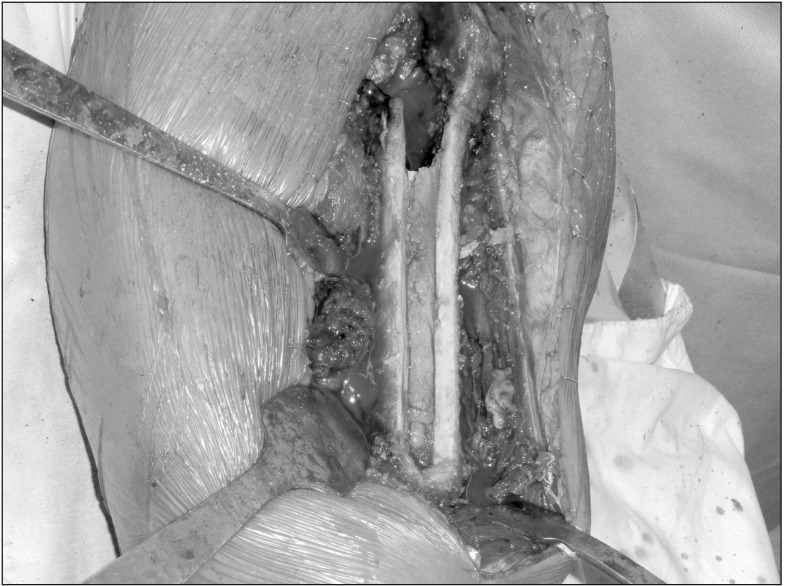
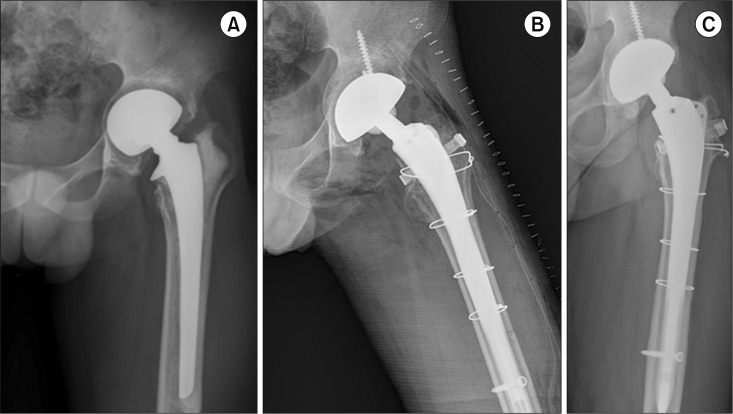
All operations were performed by two senior surgeons (KHK, YMK) via the direct lateral approach by using the anterior cortical window technique described by Kim et al.10) After deciding the range of window by the length of cement mantle or the porous coating on the previous stem, the surgeons made a longitudinal window with a thin osteotome and a sagittal saw. Then, the stem or cement mantle was removed with a thin osteotome and a curved sagittal saw (Fig. 2).
In all revisions, cementless prostheses (Plasmacup cup and Bicontact long stem; Aesculap, Tuttlingen, Germany) and alumina ceramic-on-ceramic bearing (Biolox forte; CeramTec, Plochingen, Germany) were used (Fig. 3). The stem had a distal interlocking screw. After insertion of a new stem, the widow fragment was fixed with cerclage wires (Smith & Nephew, London, UK). The diameter of femoral head was 28 mm in 53 hips and 32 mm in three hips. Patients were encouraged to walk with two crutches and toe-touch weight bearing for 2 months, and then weight-bearing was allowed as tolerated.
Follow-up Evaluations
Routine follow-up visits were scheduled at 6 weeks, 3, 6, and 12 months, and yearly thereafter. Patients who did not return for regularly scheduled visits were contacted by telephone. Clinical outcome was assessed by the modified Harris hip score, University of California at Los Angeles (UCLA) activity score, and Koval ambulation category at each visit.15) The abductor muscle strength was evaluated by the Medical Research Council scale.16) Cerclage wiring–related complications including wire breakage, wire bursitis, and trochanteric pain were recorded.
The radiographic evaluations were done by two independent observers (CHP, JY) who did not participate in the index revision. The 6-week postoperative radiographs were considered as the baseline radiographs for all comparisons. Subsidence of the femoral stem, union of the osteotomized fragment, and periprosthetic bone loss were assessed. Subsidence of the stem was defined as the change of 5 mm or more in the distance between the superolateral edge at the shoulder of the prosthesis and the tip of the greater trochanter on the anteroposterior radiograph.1718) Periprosthetic bone loss was evaluated according to the criteria by Capello et al.,19) and the location was recorded according to the seven zones described by Gruen et al.20)
Descriptive statistics were used to summarize patient demographics. Survival analysis was performed with the Kaplan-Meier method, and the 95% confidence interval (CI) was calculated. Statistical analysis was performed using IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA). We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Seoul National University Hospital (IRB No. B-1512-328-103). Informed consent was waived.
RESULTS
The median operation time was 350 minutes (range, 175 to 650 minutes), and the median blood loss was 1,250 mL (range, 500 to 4,000 mL). There was no statistically significant difference in the operation time and blood loss according to the stems used in primary THA (p = 0.67 and p = 0.461, respectively). Intraoperative femoral fractures occurred in two hips (2.6%) during creation of the anterior cortical window. The fractures occurred at the distal end of the anterior cortical window and in the cases where the anatomic medullary locking (AML; Depuy Synthes, Warsaw, IN, USA) stem was used previously. One fracture was successfully fixed with a plate during the index revision. The fracture healed and the stem was stable without subsidence at 11 years after the revision. The other fracture was fixed with cerclage bands during the index revision. However, nonunion occurred postoepratively and the stem progressively subsided. Thus, the stem was re-revised, and the nonunion was treated by plate fixation and autogenous bone graft.
Five hips dislocated after the revision. Four dislocations were successfully treated with manual reduction and a hip brace used for 2 months. The remaining one dislocation was caused by cup malposition and treated with repeated revision of the cup. Sciatic nerve palsy occurred in one hip, which was restored at 1 year after the revision.
Subsidence of the stem was observed in five hips (8.4%) during 1 year after the revision. There was no statistically significant difference in the incidence of subsidence according to the stems used in primary THA (p = 0.878). Subsidence was not progressive in three hips; it was progressive in the remaining two hips, which necessitated a repeated revision of the stem. One of these hips also had intraoperative femoral fracture and nonunion. Cortical porosis around the stem was seen in 14 hips (25%): in Gruen zones 1 and 7 in nine hips and in Gruen zone 1 in five hips. Breakage of the cerclage band was observed in 16 hips. Two of them were associated with symptomatic bursitis and underwent removal of the cerclage band.
There were two periprosthetic joint infections. One was a superficial infection, which was detected at postoperative 4 weeks. It was treated by incision and drainage, and there was no recurrence. The other infection occurred at postoperative 8 years and was treated by two-stage revision. One Vancouver type B1 periprosthetic femoral fracture occurred 2 years postoperatively and was successfully treated with open reduction and internal fixation using dual plates.
At the final follow-up, the mean Harris hip score was 82.5 (range, 31.9 to 100) and the mean UCLA activity score was 4.6 (range, 1 to 8). The mean abductor muscle strengh was 4.1 (range, 3 to 5) and the mean Koval category was 1.5 (range 1 to 7).
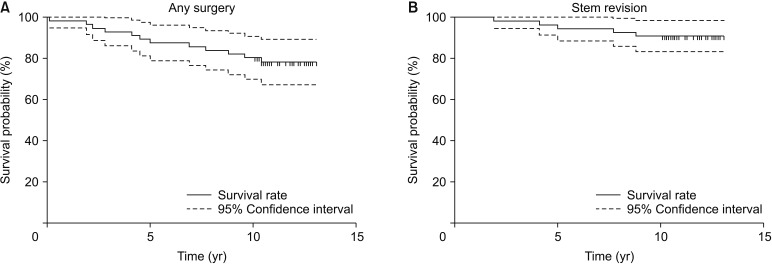
Twelve patients (12 hips, 21.4%) underwent repeated operation because of stem loosening (two hips), cerclage wire/band-related bursitis (two hips), cup loosening (four hips), periprosthetic femoral fracture (one hip), periprosthetic joint infection (one hip), removal of distal locking screw due to soft tissue irritation (one hip), or irrigation and debridement for superficial infection (one hip). Kaplan-Meier survivorship with any surgery as the end point was 80.4% (95% CI, 68.5% to 88.2%), and that with stem revision as the end point was 91.1% (95% CI, 83.6% to 98.6%) at 10 years after the index revision (Figs. 4 and 5).
DISCUSSION
This study showed a satisfactory long-term results and survivorship of revision THA using an anterior cortical window in a relatively large number of patients. In our patients, we used ceramic-on-ceramic bearing, which might have positively affected the survivorship.22) Removal of well-fixed cementless stem and cement mantle is challenging and ETO has been widely used for the removal. Charity et al.8) reported excellent results of ETO using a cemented stem at a mean follow-up of 123 months. However, the number of ETO cases was only 18. Otherwise, to the best of our knowledge, long-term results and survival rate of revision THA using ETO have not been reported yet.
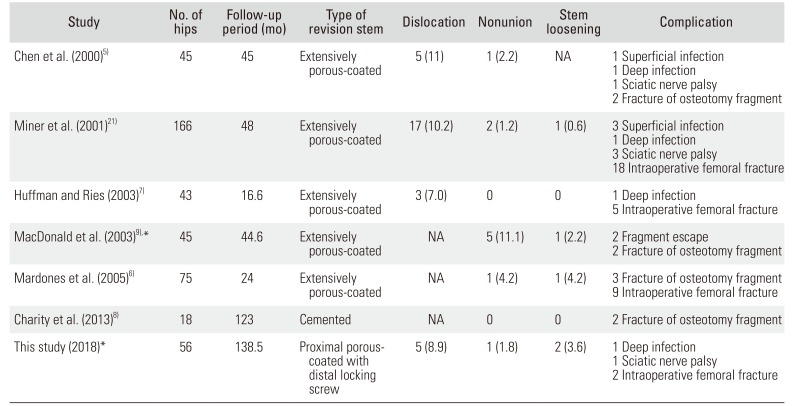
Nonunion is the most common concern after trochanteric osteotomy. Reportedly, the nonunion rate of standard trochanteric osteotomy (STO) ranged from 5% to 14%.2324) The nonunion rate has been decreased to 1% to 3% since the ETO was introduced.25) In our patients, nonunion occurred in one femur (1.8%) that had an intraoperative fracture. In our study of the anterior cortical window technique, the nonunion rate was lower than or comparable to that previously reported in STO and ETO studies (Table 2).5678921)
Because the osteotomized fragment in ETO is bigger than that in the anterior cortical window technique and the abductor muscle is attached onto the trochanteric fragment, ETO requires strong fixation of the greater trochanter. Various techniques and materials were introduced for the fixation ETO.72627) Although the fixation using a cable grip was excellent in a biomechanical study, cable grip–related complications appeared to be an issue.28) However, the osteotomy fragment of the anterior cortical window is small, does not damage the abductor mechanism, can be fixed firmly by cerclage wires or bands, and does not require cable grip (Fig. 5).
In ETO, it is not feasible to press-fit the new stem in the proximal femur, and it is necessary to use a distally fitting stem. Distally fitting modular stems with an extensive porous coating were recommended for ETO.25) However, modular stems are associated with fracture at the modular junction.29) In our study, all patients were operated with monolithic stems.
During osteotomy, the femur is vulnerable to intraoperative fractures. In our study, the incidence of intraoperative femoral fractures was 3.6% (2 / 56), whereas the incidence ranged from 4% to 30% in previous studies of ETO.2530) When making an anterior cortical window, the surgeon should take care not to cause intraoperative fractures especially at the distal end of the anterior cortical window and to avoid extensive removal of the porous-coated stem, such as the AML stem.
One of the limitations of our study was the retrospective design without a control group. Thus, we compared the results of the anterior cortical window technique with those of ETO. Another limitation was that all the operations were performed by two high-volume surgeons; the results might have been different if the operations were performed by other surgeons. Despite these limitations, this is the first study to report the long-term result of revision THA using an anterior cortical window, which provided satisfactory results and survivorship in the long term. We recommend using this technique instead of ETO for revision THA.
 XML Download
XML Download