

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Total elbow replacement was originally developed to manage end-stage rheumatoid arthritis (RA).1) Its indications have expanded to include unfixable comminuted fracture, osteoarthritis (OA), and posttraumatic arthritis.2345678910) Less commonly, it is indicated for hemophilic arthropathy, juvenile idiopathic arthritis, and primary or metastatic tumor. Despite the increasing use, however, long-term complications, such as infection, aseptic loosening, instability, and periprosthetic fracture, remain a challenge.111213141516) Because it is a relatively rare procedure, most surgeons have less experience with total elbow arthroplasty (TEA) than hip and knee arthroplasty, and few long-term outcome data are available. Therefore, to avoid iatrogenic errors, surgeons should carefully review the previous literature on TEA. In this review article, we summarize the prosthesis designs and outcomes of TEA and management of patients undergoing revision surgery.
TYPES OF IMPLANTS AND BIOMECHANICS
Implant designs for TEA have evolved in recent decades since 1972 when Dee1) first reported on the outcomes of TEA using a hinged implant in RA patients. According to a recent systematic review, 19 specific designs have been introduced.17) In the present study, we report on four popular implant systems among more than 10 types of implants.14)
Unlinked Design (Kudo Type 5 System)
The Kudo prosthesis was first reported in 199018) and is one of the most popular unlinked TEA designs used to treat end-stage RA of the elbow.19) Theoretically, unlinked TEA has no mechanical connection between the humeral and ulnar components and thus has advantages of near-normal elbow kinematics and preservation of bone stock. The unlinked design was established to overcome loosening of the hinge prosthesis. Unlinked TEA is appropriate only for patients with limited bone loss or limited deformity and good ligament function. Nonconstrained TEAs have low intrinsic stability and rely on soft-tissue balancing. The primary stabilizers of nonconstrained TEA are the medial and lateral collateral ligaments,20) and the posterior capsule and surrounding muscles function as secondary stabilizers. This is because postoperative instability is a major complication of unlinked prostheses. The concept and objective of unlinked TEA are to share the loading stress on the bone-implant interface with the surrounding tissues. Kodama et al.2122) reported survival rates of 87.8% at 5 years and 70.7% at 10 years, and the most common complication was aseptic loosening.
Linked Semiconstrained Design (Coonrad-Morrey)
The Coonrad-Morrey Total Elbow (Zimmer, Warsaw, IN, USA) is a second-generation linked semiconstrained design featuring a central cylindrical bearing and two side bearings. The linked semiconstrained implant is one of the most frequently used devices for TEA. It allows some varus-valgus motion, reducing stress concentration on the bone-cement interface.20232425) The implant permits 7°–10° of varus-valgus movement and 7°–10° of axial rotation of the knee. Adding an anterior flange to the humeral component also protects the bone-cement interface from stress forces. The central locking pin was redesigned in 1996. The ulnar component was modified from a beaded surface to a polymethylmethacrylate-precoated surface in 1992, but it was turned back to have a beaded surface in 2001.262728) This design has been used to treat conditions including RA, degenerative arthritis, and trauma reconstruction, and satisfactory outcomes have been reported with long-term follow-up.252930313233343536) However, aseptic loosening together with bushing wear is a leading complication of implant failure, and reducing the complication rate remains a challenge.13202437)
Semiconstrained Condylar-Bearing Design (Discovery Elbow System)
The Discovery Elbow System (Biomet LLC, Warsaw, IN, USA) is a hemispherical linked prosthesis designed to decrease complications associated with a semiconstrained prosthesis, especially bushing wear.26) Its minimally constrained design allows a close match of the articular surfaces, avoids the use of a true hinge, and anatomically reproduces the axis of elbow motion. Its floppy hinge allows for 6°–8° of varus-valgus and rotational motion; the increased contact area between the cobalt-chrome and ultra-high-molecular-weight polyethylene prevents the occurrence of edge loading and reduces stresses within the polyethylene TEA. Moreover, the design enables posterior access during bushing revision.383940)
Convertible Design (Latitude System)
More recently, convertible TEAs (Latitude Tornier implant system; Tornier, Montbonnot-Saint-Martin, France) allow surgeons to choose between a nonconstrained and semiconstrained prosthesis.4142) If the surgeon has concerns regarding collateral ligament insufficiency or implant stability, a semiconstrained hinge can be created by applying a modular component to the ulnar prosthesis. Two-year follow-up outcome of convertible TEA was comparable with that in historical controls; however, no long-term survival data have been reported.4142)
Go to : 
CLINICAL OUTCOMES
Overall Outcomes and Survival Rates
A recent systematic review reported promising overall clinical outcomes for pain relief, restoration of function, and range of motion. Welsink and the colleagues1743) systematically analyzed 73 articles and reported overall outcomes: the weighted mean American Shoulder and Elbow Surgeons score was 66.7 points, patients with RA had a weighted mean Mayo Elbow Performance Score (MEPS) of 85.3 points, and those with trauma or fracture had a weighted mean MEPS of 84.1 points. In addition, they found that approximately 60% of the patients were pain-free at the latest follow-up (mean, 6.3 years). The weighted mean difference of the flexion angle was 129°, and the weighted mean extension lag was 30°. The weighted mean supination was 66°, and the weighted mean pronation was 71°. The complication rate was 19.1% (at 5.9 years) for the linked prosthesis and 26.5% (at 8.2 years) for the unlinked prosthesis (Table 1).1743) Using data from the Norwegian Arthroplasty Register from 1994 to 2016, Krukhaug et al.44) reported that overall outcomes and survival rates of TEA demonstrated overall 5-, 10-, 15-, and 20-year survival rates of 92%, 81%, 71%, and 61%, respectively.
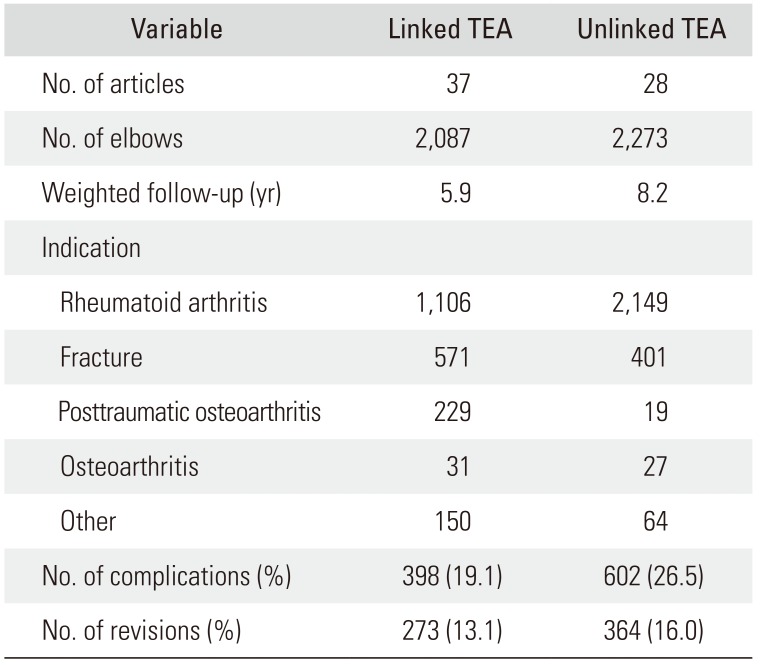
Table 1
Indication and Complication Rate of TEA
![]()
Rheumatoid Arthritis
The annual incidence of TEAs performed for inflammatory arthritis is decreasing, which is probably due to the efficacy of disease-modifying antirheumatic drugs.1417) Despite this progress in the medical treatment of RA, severe cases are still the most common indications for TEA after failed medical treatment. A mean patient satisfaction of 9.2 out of a possible 10 points was reported in a study by Hildebrand et al.45) on the functional outcome of patients with inflammatory arthritis who underwent TEA. A study by Mansat and the colleagues2933) demonstrated that treatment outcome after TEA for RA with a minimum 2-year follow-up had a 97% survival rate (95% confidence interval [CI], 83.6% to 99.6%) at 5 years and 85% (95% CI, 68.3% to 93.7%) at 10 years. At an average of 7 years of follow-up (range, 2–16 years), the mean MEPS was 91 points (range, 55–100 points), and the shortened version of the Disabilities of the Arm, Shoulder and Hand score was 34 points (range, 0–75 points). A significant improvement was seen in the MEPS and in all range of motion scores at the latest follow-up in comparison to preoperative values.
Distal Humerus Fracture
Because many surgeons currently select TEA to manage comminuted distal humerus fracture, the indications for TEA for trauma-related disease have expanded.57894647484950) However, the choice of treatment remains debatable in younger patients because long-term outcomes are not available owing to the paucity of data.4950) Rajaee et al.9) compared TEA with open reduction and internal fixation (ORIF) using data obtained from the Nationwide Inpatient Sample for 2002–2012.51) The data demonstrated that the annual frequency of TEA increased 2.6-fold in elderly patients with distal humerus fractures, and TEA is the preferred treatment alternative to ORIF in elderly patients with complex distal humerus fractures that are not amenable to stable fixation. In 44 TEAs after distal humeral fracture, Barco et al.52) reported that the mean visual analog scale score for pain was 0.6, the mean flexion was 123°, and the mean loss of extension was 24°. The mean MEPS was 90.5 points, with three patients scoring < 75 points.
Posttraumatic Arthritis
TEA could be a treatment option for advanced posttraumatic arthritis, but the outcome is not satisfactory when compared to other indications.91731535455) Patients typically have > 1 previous surgery with scars and severe limited range of motion due to soft-tissue contraction. This disadvantage leads to difficulty in approaching and managing the soft tissue. The worse prognosis was seen in patients who developed traumatic arthritis after fracture than in patients with inflammatory arthritis.445657) Hildebrand et al.45) also reported the functional outcome of TEA in patients with posttraumatic arthritis. The mean score (and standard deviation) on the Mayo Elbow Performance Index was significantly higher for the group with inflammatory arthritis (90 ± 11 points) than for the group with a traumatic or posttraumatic condition (78 ± 18 points) at the latest follow-up. Younger patients with advanced posttraumatic arthritis who are not well managed present a difficult dilemma. Celli and Morrey58) reported a series of 55 TEAs performed in patients aged < 40 years with a mean 7.5-year follow-up. Thirty-six patient (65%) were considered to be excellent and fifteen (27%) were good. Similarly, Park et al.59) reported a series of 23 TEAs performed in patients aged < 40 years with a mean follow-up of 10 years. Despite the reported favorable outcomes, however, 25% of elbows developed complications, with 22% requiring reoperation.
Primary OA
Because the elbow is not a weight-bearing joint, the incidence of primary OA is rarer than that in other joints. The incidence is higher in the overused upper extremities (in manual laborers, throwing athletes, wheelchair-assisted individuals). Patients with primary OA typically have higher functional demands and capabilities than those with inflammatory arthritis.60) Thus, it is critical to communicate with the patient regarding postoperative management, with the surgeon stressing that the risk of complications could increase if the patient continues to have the same habitual pattern of elbow use. Schoch et al.10) reported satisfactory outcomes; however, extension gain was not always achieved. Complications occurred in a large number of elbows, but the incidence of mechanical failure was low. The MEPS for 13 elbows without mechanical failure averaged 81.5 points (range, 60–100 points).
Go to :
COMPLICATIONS
The increase in complications of revision TEA parallels the increase in primary TEA.144449) It is well known that survival in TEA is substantially longer in patients with inflammatory arthritis than in those with trauma-related indications.4555) An increased risk of complications is also seen in patients with young age, obesity, smoking, and high comorbidity.43505861626364) Linked arthroplasties tend to require more revisions due to polyethylene wear, whereas more revisions are performed in cases with unlinked prostheses due to instability and dislocations.171923434465) Infection, aseptic loosening, and periprosthetic fracture are the most concerning common complications primarily requiring revision surgery.
Periprosthetic Joint Infection
Even with modern surgical techniques and antibiotic prophylaxis, infection remains one of the leading complications of TEA, with reported rates ranging from 1% to 12.5%.4361666768) While there is a consensus on and greater understanding of the management of hip and knee periprosthetic joint infection (PJI),6768697071) few studies have evaluated the management of elbow PJI after TEA because of its rarity. However, it is generally understood that the elbow is susceptible to infection owing to the lack of soft-tissue covering from skin to bone.6670727374) Therefore, the surgeon must take care in every step of the surgical process including patient selection, aseptic surgical conditioning, and frozen sectioning of suspicious tissue before performing the implantation procedure to reduce or prevent the risk of infection. In the patient selection stage, the surgeon should be aware of the risk of high comorbidity with diabetes.6273757677) Several studies have reported a strong correlation between infection and comorbidity with TEA.6166737879) Even after the surgery, preventing infection requires general control of the comorbidities. Although a consensus is not fully established, two-stage revision surgery is commonly recommended.798081) Zmistowski et al.82) reported that two-stage revision led to a decreased rate of recurrent PJI and a 50% success rate over 3 years, and they recommended a prosthesis-free interval of at least 3 months. The most common pathogen was Staphylococcus aureus.616870727483848586)
Aseptic Loosening
Aseptic loosening is one of the most common causes of revision surgery.1415161787) Stress shielding at the elbow is applied to determine the incidence of osteolysis around the implant and loosening. As Wolff's law states, bone will adapt to the loads under which it is placed. If loading on a bone increases, the bone will remodel over time and become stronger. Conversely, if loading decreases, the bone will become less dense and weaker due to the lack of stimulus required for continued remodeling. In TEA, the transmission of nonanatomic force results in stress shielding at the humeral condyles and olecranon, leading to progressive bone resorption (Fig. 1).26378889) This bone resorption increases the moment of force on the arm between the hinge and the site where the stem transfers most of its load, which not only predisposes to loosening of the stem but also increases the likelihood of arthroplasty failure due to polyethylene wear, mechanical failure, or periprosthetic fracture.11202637498889) Loose stems are amenable to revision TEA generally using a longer stem, with bone grafting performed if indicated.208890) King et al.91) reported a series of 31 patients who underwent revision TEA due to aseptic loosening with a mean 6-year follow-up. The mean MEPS was 87, and the mean flexion-extension arc was > 100°.

Periprosthetic Fracture
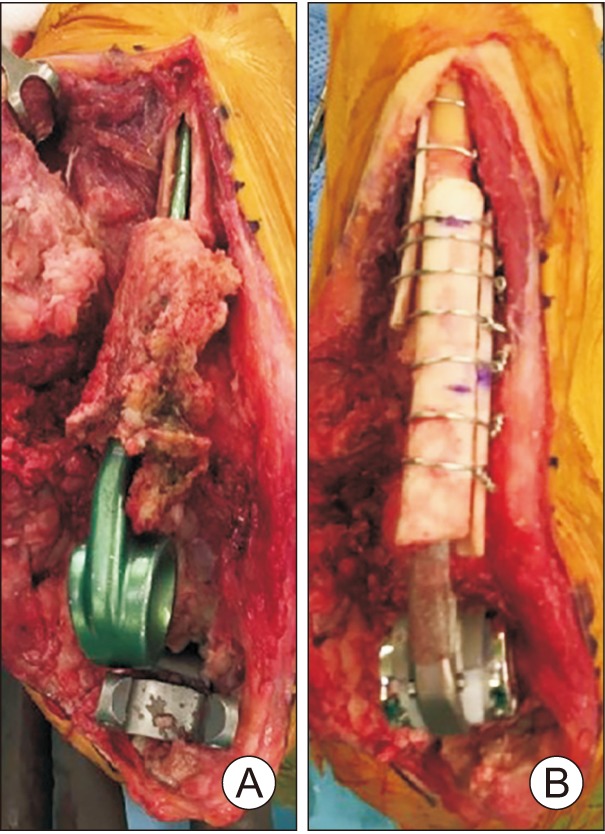
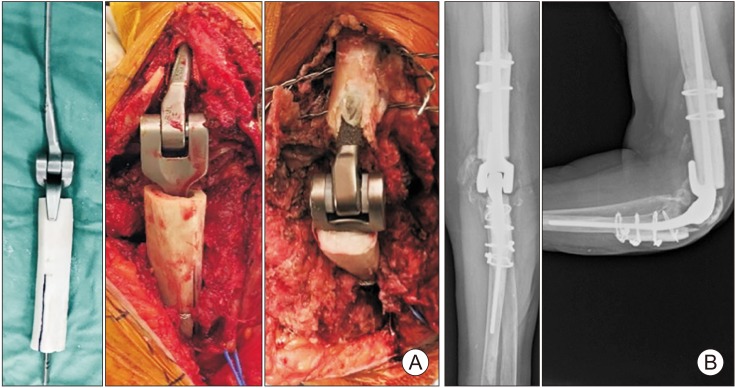
Periprosthetic fractures are the third most common cause of failure and pose difficulty for revision.65) Although some of the principles used in treating periprosthetic hip and knee fractures can be applied to the elbow, some differences must be considered to provide the best possible treatment.92) Because the upper extremity has smaller bones with less bone stock, management of bone defects is critical. Bone stock in both the ulna and the humerus is limited, and thus when fracture occurs, revision surgery can be challenging. Inadequate bone stock is a commonly encountered problem, particularly in patients with osteoporosis (Fig. 2). Cortical strut allograft augmentation is a recommended technique for revision in patients with poor or weak bone stock. A study has reported that periprosthetic humeral fractures associated with a loose humeral component can be effectively treated with revision elbow arthroplasty and strut allograft augmentation (Fig. 3).92)
 | Fig. 2Osteoporotic periprosthetic fracture due to a fall injury after unlinked total elbow arthroplasty.
|
 | Fig. 3(A, B) Strut graft augmentation is typically required after nonviable bone extraction. The graft must be long enough to span the fracture site and allow sufficient fixation of both the proximal and distal fragments. Cancellous bone from the humeral head allograft can be morselized for later use.
|
Triceps Insufficiency
Triceps insufficiency can commonly occur after a failed surgical reattachment, particularly when tendon quality is poor or a traumatic rupture of the tendon is present. In recent systematic reviews, the rate of triceps insufficiently was between 0.4% and 2.4% after TEA using various triceps-detaching approaches.9394) In an effort to reduce the risk of postoperative triceps weakness and rupture, a triceps-sparing approach has been applied for primary TEA. In the setting of primary TEA, several studies suggest that a triceps-sparing approach leads to fewer postoperative triceps ruptures as well as better postoperative range of motion and extension torque.1794) Dachs et al.95) compared triceps-sparing and triceps-detaching approaches for primary TEA: the rate of postoperative triceps rupture was 15.2% in the triceps-detaching group but the rupture was not observed in the triceps-sparing group. Solarz et al.96) compared the triceps-sparing with triceps-detaching approaches and reported that functional strength and Disabilities of the Arm, Shoulder and Hand scores were significantly higher in the triceps-sparing group. Arc of motion, visual analog scale, and MEPS were similar between the triceps-sparing and triceps-detaching groups.
Bushing Wear
Goldberg et al.89) reported that multimodal wear in total elbow replacements can lead to osteolysis, aseptic loosening, and prosthetic and periprosthetic fracture, necessitating revision surgery. Polyethylene wear and damage, as well as unintended metal-on-metal wear, contribute to the periprosthetic particulate burden, which is probably pathogenic in these processes. Lee et al.97) suggested that one of the reasons for a component stem fracture after TEA seems to be fatigue failure at or near the junction between an unsupported stem and well-fixed stem. This area of unsupported stem develops as a result of osteolysis caused by bushing wear. It was emphasized that the solution for component fractures requires a solution for bushing wear.
Other Complications
Other serious complications after TEA include wound breakage, especially round the olecranon. Rhee et al.88) reported that under unfavorable soft-tissue conditions, performing soft-tissue reconstruction with TEA provides satisfactory functional improvement and pain relief. The two-stage surgery provided a lower rate of wound complication and better elbow function than the one-stage surgery, which led to high patient satisfaction postoperatively. Development of ulnar nerve lesions is a significant complication after TEA, with potentially debilitating consequences. The outcomes of unlar nerve release with different techniques have been reported. Dachs et al.98) reported on transposition versus in situ release: of the four patients who underwent transposition, two had postoperative ulnar nerve symptoms; in the in situ release group, the incidence of postoperative ulnar nerve symptoms was 5% (4 / 78).
Go to :
REVISION TEA
Types of TEA failure can be classified as infected and non-infected based on serologic markers, imaging, and intraoperative histology.20236199) Therefore, revision TEA should be determined on the basis of the type of failure. In the infected type of failure, infectious foci should be surgically removed by extracting the implant, and this should be followed by reimplantation in addition to treatment with systemic antibiotics.2370727983) In contrast, the non-infected type should be treated by addressing the mechanical problems at the implant-bone or implant-implant interface.65819092100101102) Therefore, understanding the pathological mechanism of failure is critical when performing revision surgery and managing complications of TEA. Typically, two different surgical techniques are performed after the diagnosis. Two-stage revision surgery is usually indicated in patients with deep periprosthetic infection, whereas patients without signs suggesting infection, based on the Musculoskeletal Infection Society standards,6770) undergo single-stage revision surgery. If one of the components is stable, the type of implant that matches the original implant is chosen.
Single-Stage Revision Surgery for Non-Infectious Causes
After joint exposure, the remaining bone stock and the quality of the soft tissues are carefully inspected, which is followed by sharp subperiosteal release of the collateral ligament structures from the medial and lateral epicondyles. The preexisting components are meticulously removed to avoid further injury to the bones. Removing as much of the cement as possible from the medullary canal is required; however, tightly adhered cement can be left in place if it does not interfere with the implantation of the revision stem. Bone loss is managed with either cement or shortening of the humerus or ulna. In the case of epicondyle fractures, Kirschner-wires are used to temporarily fix the fragments before reimplanting the components and cerclage wire is used for longitudinal fractures of the humerus or ulna. The humeral and ulnar shafts undergo extensive saline irrigation before the cement is introduced by using a third-generation cementing technique. Fluoroscopy is performed if the intramedullary canal of the humerus or ulna is difficult to locate. A longer component is preferred in all patients.376592)
Two-Stage Revision Surgery for Infectious Causes
The first stage of surgery should focus on removing the infected tissues and the prosthesis. All cement and any tissue suspected of infection, including the synovial membrane, are completely and carefully removed. Samples of tissue surrounding the implants and joint fluid are cultured. The bones are windowed for well-fixed implants, and chlorhexidine solution diluted with 0.9% sodium chloride is used to irrigate the canals. In addition, an antibiotic cement spacer (5-g gentamicin, 1-g vancomycin, and 1-g ceftriaxone per 40-g cement) is introduced (Fig. 4). Patients receive the optimum dosage of intravenous antibiotics, on the basis of sensitivity tests, for > 6 weeks until complete normalization of all serologic markers (white blood cell counts, erythrocyte sedimentation rates, and C-reactive protein concentrations) has occurred.707983) The second stage of surgery centers on infection control and joint reconstruction with a new implant. After removal of the antibiotic cement spacer, tissue samples are acquired for follow-up sensitivity testing. All frozen intraoperative tissue samples are examined histologically to confirm the results from the real-time diagnostic tools. Acute inflammation is described as ≥ 5 neutrophils per high-powered field, with any positive result nullifying the reimplantation procedure.7985)
 | Fig. 4First stage of revision surgery. (A) Chronic deep infection. Partial absoprtion of the distal humerus and proximal ulna, caused by chronic infection and polyethylene wear. (B) Implant removal and insertion of an antibiotic cement spacer. The fracture occurred during removal of the cement (arrows).
|
Morrey et al.90) proposed three specific reconstruction techniques using allograft-prosthetic composite (APC) to manage bone defects. Type I reconstruction involves intussusception of the APC into the host bone (intussusception type) and is sometimes modified in a reverse fashion, such that the upper portion of the host bone is inserted by using the lower portion of the femur shaft as the allograft in case the host bone is too narrow to insert the allograft bone (Fig. 5A). Type II involves inserting the distal aspect of the stem into the host canal with a strutlike extension of the graft coadapted externally to the cortex while adapting a cortical strut graft. Type III comprises side-to-side contact between the cortices of the APC and the host bone. Wiring is frequently added to enhance the contact area and promote stable fixation between the host bones and the APC (Fig. 5B).
Go to :
CONCLUSIONS
Although the annual incidence of TEAs performed for inflammatory arthritis is decreasing, RA still has been the most common indication with favorable outcomes. The indications for TEA have expanded to include traumarelated problems such as posttraumatic arthritis and unreconstructable elbow fracture. The high complication rate is still a challenge, but various efforts have been made in revision surgery, such as development of devices with different designs and surgical techniques.
Go to :
 XML Download
XML Download