

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is a heterogeneous disease, typically characterized by chronic airway inflammation. Inhaled corticosteroids (ICSs) are the most widely used anti-inflammatory drugs, and can be used at various doses to control symptoms of asthma.12 However, long-term use of high-dose ICS therapy can potentially cause systemic side effects, including impaired growth in children, decreased bone mineral density, skin thinning and bruising, and cataracts.34 Accordingly, current guidelines recommend the use of the lowest dose of ICS that can maintain disease control.156 However, most maintenance anti-asthmatic drugs, including ICS, do not affect the underlying immune response; therefore when these medications are discontinued, symptoms can recur.789
Allergen immunotherapy (AIT) is the only treatment modality that can change the natural course of allergic disease.710 Its immunological mechanisms of action involve the induction of allergen-specific immune tolerance.10 Thus, AIT is a potential therapeutic option in appropriately selected patients with allergic asthma.11 There is increasing evidence of the clinical efficacy of AIT in the treatment of allergic asthma. The Global Initiative for Asthma (GINA) guidelines on the management of asthma have recently been updated to include AIT as an additional option for the treatment of asthma.12 The majority of published reports have assessed the effects of AIT in patients with allergic rhinitis, and the results with respect to asthma primarily comprised secondary outcomes. Several studies have been conducted to evaluate the efficacy of AIT for asthma, but the optimal parameters for asthma control in clinical trials remain controversial.5713 In the present study, we investigated the efficacy of AIT with respect to changes in ICS dose in patients with allergic asthma by reducing the ICS dose while monitoring the asthma control status during the study period.
MATERIALS AND METHODS
Study design and population
This retrospective study included a total of 131 adult asthmatic patients at >18 years of age in Dong-A University Hospital (Busan, Korea) from 2000 to 2015. All of the subjects had positive results on skin prick test and/or ImmunoCAP to common inhalant allergens, and had used ICS for asthma control for more than 1 year. A diagnosis of asthma was based on clinical symptoms, spirometry with bronchodilator test, and airway hyperresponsiveness (AHR) to methacholine or mannitol.
We compared clinical parameters between the 2 groups: the AIT group (n = 56) and the non-AIT group (ICS treatment without AIT, n = 75). The AIT group had received subcutaneous AIT monthly as a maintenance treatment for more than 1 year; the non-AIT group had been treated with ICS without AIT for more than 1 year. There was no significant difference in the use of other maintenance anti-asthmatic drugs, such as leukotriene receptor antagonist and long-acting beta-agonist between the 2 groups. To minimize the effect of potential confounding factors including age, gender and lung function, we used an inverse probability of treatment weighting (IPTW) method. Finally, 48 patients in the AIT group and 69 patients in the non-AIT group were analyzed in this study (Fig. 1).

Assessment
The effect of AIT was assessed by monitoring changes in ICS dose from baseline. The changes in ICS dose were initially evaluated after 6 months of treatment, and were subsequently evaluated annually for 3 years. We defined the baseline ICS dose as low, moderate or high in accordance with the GINA guidelines.14 Changes in ICS dose were classified as increase, no change, decrease, or discontinuation of ICS. A decrease (or increase) in ICS dose was defined as a decrease (or increase) of the mean daily ICS dose, which was determined by calculating the beclomethasone dipropionate 100 µg equivalent dose over 6 months compared to the baseline ICS dose before treatment. At each visit (every 2 or 3 months), the ICS dose was adjusted according to the recommendations of 2 allergy specialists based on the symptoms, Asthma Control Test score, lung function, use of rescue medications, airway inflammation (sputum eosinophils or exhaled nitric oxide), and risk factors. Patients with discontinuation or a decrease in the ICS dose compared to the baseline were classified as responders, whereas patients with no changes or an increase in the ICS dose were classified as non-responders. AHR was measured by methacholine (20% decrease in the forced expiratory volume in 1 second [FEV1] from baseline ≤ 16 mg/mL) or mannitol bronchial provocation test (provocative dose to produce a 15% fall in FEV1 ≤ 635 mg).
Statistical analysis
Quantitative and qualitative results are means ± standard deviations and absolute numbers or frequencies, respectively. To balance the subjects between the AIT and non-AIT groups, an IPTW method was used. Using the weights calculated by propensity, we compared the efficacy between AIT and ICS. Statistical analysis was performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was assessed using the t test, paired t test or Mann-Whitney U test for continuous variables and Fisher's exact test for categorical variables. A P value of < 0.05 was considered statistically significant.
IPTW
IPTW methods enable observational studies to be designed similarly to randomized experiments. IPTW involves a weighted sample in which the distribution of the baseline covariates is similar between the treated and control subjects. The propensity score is the conditional probability of being treated given a set of observed potential confounders. In this way, all information from a large number of potential confounders is summarized into a unique balancing score variable. IPTW is calculated as the inverse of the conditional probability of receiving the exposure that a patient indeed received. The aim of IPTW is to reduce selection bias by creating a “pseudo-population” in which exposure is independent of the measured confounders so that the treatment effect estimate in a sample thus weighted will be less biased. IPTW analysis was performed using SPSS version 18.0 (SPSS Inc.).
RESULTS
Demographic and clinical characteristics of the subjects
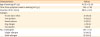
A total of 117 patients was included in the analysis; 48 in the AIT group, and 69 in the non-AIT group. There were no significant differences in sex, age, smoking status, body mass index (BMI), or AHR between the 2 groups. Patients in the AIT group had a significantly longer interval between symptom onset and ICS use than those in the non-AIT group (48.41 ± 72.51 months vs. 13.36 ± 31.73 months, P = 0.008). Allergic rhinitis was more common in the AIT group than in the non-AIT group (91.7% vs. 60.9%, P < 0.001), and pre-FEV1 and FEV1/forced vital capacity (FVC) at baseline were higher in the AIT group than in the non-AIT group (85.01% ± 15.40% vs. 80.69% ± 17.73%, P = 0.174 for pre-FEV1; 79.98% ± 6.50% vs. 75.48% ± 10.17%, P = 0.009 for FEV1/FVC), but the difference in pre-FEV1 was not statistically significant. The proportions of patients who had been treated with low, medium, and high doses of ICS did not differ significantly between the 2 groups (Table 1).
Table 1
Baseline demographic and clinical characteristics of study subjects

Values are presented as means ± standard deviations or number (%).
AIT, allergen immunotherapy; BMI, body mass index; ICS, inhaled corticosteroid; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; AHR, airway hyperresponsiveness.
![]()
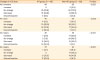
The clinical characteristics of the patients who received AIT are shown in Table 2. House dust mite (HDM, 72.9%) was the most common allergen for AIT, followed by tree pollens (33.3%), weed pollens (27.1%), dog dander (12.5%), and cat dander (6.2%). Single-allergen AIT (HDM alone) was administered to 45.5% of the patients, and multi-allergen AIT (HDM + pollens or animal dander) was administered to 54.5% of the patients. The mean duration of AIT was 28.19 ± 9.12 months and was not significantly different between the single- and multi-allergen treated groups.
Table 2
Clinical characteristics of the patients who received AIT (n = 48)
![]()
Treatment response in the AIT and non-AIT groups
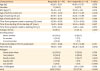
The changes in ICS dose differed significantly between the 2 groups throughout the study period (Table 3). After 6 months and 1 year of the treatment, the proportion of patients with no change in the ICS dose was significantly lower in the AIT group than in the non-AIT group (at 6 months, 47.9% vs. 72.5%; at 1 year, 20.8% vs. 55.1%); however, the proportion of patients with a decrease in ICS dose was significantly higher in the AIT group than in the non-AIT group after 6 months and 1 year of treatment (at 6 months, 43.8% vs. 20.3%; at 1 year, 47.9% vs. 24.6%). The percentages of responders in the 2 groups are shown in Fig. 2; the proportion of responders in the AIT group was significantly higher than that in the non-AIT group throughout the study period. Lung function after 1 year of treatment is shown in Fig. 3. There was no significant difference in pre-FEV1 between the 2 groups (80.10 ± 18.17% vs. 81.04 ± 17.32%, P =0.816). Also, no significant differences in changes in pre-FEV1 from baseline until 1 year of treatment were noted between the groups (Fig. 3).
Table 3
Changes in ICS dose from baseline
![]()
 | Fig. 2Comparison of responders who discontinued or decreased in the ICS dose compared with the baseline in the AIT and non-AIT groups during the 3-year study period.ICS, inhaled corticosteroid; AIT, allergen immunotherapy.
|
 | Fig. 3Changes in lung function after 1 year of treatment in the AIT and non-AIT groups.AIT, allergen immunotherapy; FEV1, forced expiratory volume in 1 second; SD, standard deviation.
|
We investigated the occurrence of acute exacerbation (AE) (Fig. 4). AE was defined as systemic steroid treatment for more than 3 days or receiving systemic steroids during an emergency department visit or hospitalization to reduce symptoms. The proportion of patients with AE was significantly lower in the AIT group than in the non-AIT group during the first year (8.3% vs. 27.9%, P = 0.010), and the time to reach the first AE was longer in the AIT group than in the non-AIT group (18.30 ± 12.13 months vs. 9.57 ±5.85 months, P = 0.053).

Clinical features of responders and non-responders
Among patients in the AIT group after 1 year of treatment, 34 (70.8%) were responders who discontinued or decreased the ICS dose compared with the baseline. We analyzed the clinical features between the responder group and non-responder groups after 1 year of treatment (Table 4). There were no significant differences in sex, age, BMI, allergen, or smoking status between the responder and non-responder groups. However, patients in the responder group showed earlier asthma onset than those in the non-responder group (31.36 ± 14.36 years vs. 38.37 ± 10.05 years, P = 0.046). There were no significant differences between the 2 groups in age when ICS or AIT was started, or the time from symptom onset to starting ICS or AIT. Although not statistically significant, the responder group had a higher prevalence of allergic rhinitis and higher baseline lung function than the non-responder group (97.1% vs. 71.4%, P = 0.059 for allergic rhinitis; 87.41% ± 12.88% vs. 79.12% ± 19.66%, P = 0.133 for pre-FEV1). Baseline AHR did not differ between the 2 groups (76.0% vs. 77.8%, P > 0.900). There was no significant difference in the type of allergen used for AIT between the groups. Regarding the treatment response between patients who received AIT for HDM alone and those administered AIT for multi-allergens (HDM + pollens or animal dander, Fig. 5), no significant difference was found in the proportion of responders between the 2 groups throughout the study period (at 6 months, 45.7% vs. 53.8%; at 1 year, 68.6% vs. 76.9%; at 2 years, 82.8% vs. 100.0%; and at 3 years, 100.0% vs. 88.9%).
Table 4
Clinical features of responders and non-responders after 1 year of AIT
Values are presented as means ± standard deviations or number (%).
AIT, allergen immunotherapy; BMI, body mass index; ICS, inhaled corticosteroid; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; AHR, airway hyperresponsiveness.
![]()

Safety of AIT
Of the 48 patients in the AIT group, 11 (22.9%) experienced systemic adverse events related to AIT. Eight patients (72.7%) had adverse events during rush immunotherapy. The severity of the systemic adverse events was evaluated according to the World Health Organization subcutaneous immunotherapy systemic reaction grading system15 as grade I in 4 patients (36.7%), grade II in 1 patient (9.1%) and grade III in 6 patients (54.5%). Life-threatening anaphylactic shock or death (grade IV or V) was not recorded.
DISCUSSION
AIT is the only disease-modifying treatment option for allergic diseases.71617 Since the first report of AIT approximately 100 years ago, many studies have reported the efficacy and safety of AIT in the treatment of allergic diseases including rhinoconjunctivitis and asthma.51118 However, there remain many opinions on evaluating the effectiveness of subcutaneous AIT on allergic asthma, as well as concerns about its side effects. In the present study, patients who received AIT required significantly lower ICS doses for asthma control than those who received ICS alone. After 6 months of treatment, the percentage of responders who had discontinued or had a decrease in the ICS dose, even with achieving asthma control was significantly higher in the AIT group than in the non-AIT group, and increased over time throughout the study. The ICS-sparing effect of AIT occurred earlier (even after 6 months), and further increased with increasing duration of AIT. When AIT was continued for 3 years, the proportion of responders was higher in the AIT group (96.3%): more than 63.0% of the subjects in the AIT group had discontinued ICS and maintained their control status. A recent study demonstrated that subcutaneous AIT had an ICS-sparing effect in 65 children with HDM-allergic asthma compared to the controls.5 In that study, a significant reduction in ICS dose was found at 2 years in the AIT compared to the non-AIT group (48.5% vs. 18.7%). There was also a significant decrease in serum specific immunoglobulin E (IgE) to HDM and a significant increase in specific IgG1/IgG4 to HDM.5 The clinical efficacy of AIT is supported by immunologic changes, although a specific mechanism has not yet been elucidated.19 Notably, the prior study was conducted in children at 6–17 years of age. However, the present study was conducted in adult asthmatic patients at >18 years of age, and enrolled patients with mono-sensitized to HDM and poly-sensitized to HDM and inhalant pollens (tree and weed) and animal dander (cat and dog dander). Moreover, the proportion of responders who discontinued ICS or reduced their ICS dose at 2 years after confirming control status was 86.0%, which was greater than that in the previous study. In addition, the AIT group showed a lower incidence of AEs in the first year of the study period, and the first AE was delayed, compared to the non-AIT group. A prior study reported the efficacy of sublingual AIT (in aspects of reduction of the ICS dose) in 604 HDM-sensitive adult asthmatic patients comorbid with rhinitis compared to placebo. The relative mean reduction in ICS dose was 42.0% in the sublingual AIT-treated group and 15.0% in the placebo group.16 These findings suggest that AIT has a remarkable ICS-sparing effect, and is beneficial to reduce AE to achieve better asthma control in adult asthmatic patients with the phenotype of allergic asthma.
There have been several studies of factors related to the effects of AIT in asthmatic patients.57111620 However, the condition of the subjects, type of allergen, method of AIT, follow-up period, and end point for efficacy assessment varied considerably among these studies. In the present study, we did not limit the disease severity or causal allergens of the enrolled subjects. Therefore, our results may reflect the efficacy of AIT in adult asthmatics in real-world clinical practice. In addition, we balanced the AIT and non-AIT groups in aspects of the baseline values of variables including age, sex, and lung function to adjust for observational differences. The patients in the AIT group had a significantly higher prevalence of allergic rhinitis and significantly longer duration from symptom onset to starting ICS treatment. The close relationship between allergic rhinitis and asthma is well known1821; control of allergic rhinitis is known to improve asthma control.2223 The present study showed that the proportion of patients with allergic rhinitis was higher in the responder group than in the non-responder group. Improved control of allergic rhinitis by AIT could enhance control of asthma. Furthermore, this study showed the long-term safety of subcutaneous AIT in adult patients with allergic asthma. Most adverse events were not serious and occurred during the build-up phase, particularly during rush immunotherapy. No patients discontinued AIT because of adverse events including anaphylactic shock.
There were several limitations to this study. First, it was a retrospective study; therefore, the ICS dose was assessed based on the medical records. Also, treatment compliance could not be evaluated. However, this was a real-world clinical study; most of the subjects visited our allergy clinic every 2 or 3 months, and their ICS dose was adjusted and prescribed by 2 allergy specialists after confirming the control status. Secondly, we could not use uniform sources of allergen extracts for AIT, as allergen extracts from 3 manufacturers were used according to the patients' conditions. However, there were no significant differences in treatment responses, such as changes in the ICS dose, AE rate, and lung function, among the products of the 3 manufacturers. Thirdly, the duration of AIT was not fixed; thus, further extended studies of the long-term effects of AIT are needed, as the maximum monitoring duration was 3 years in the present study.
In conclusion, irrespective of the type of allergen, AIT had a significant ICS-sparing effect and reduced AEs in patients with allergic asthma. Long-term maintenance AIT may help reduce the burden of ICS exposure in patients with allergic asthma in real-world clinical practice.
 XML Download
XML Download