

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The natural history of asthma includes episodes of acute exacerbation which impose a considerable morbidity on patients and may lead to an impaired long-term prognosis by accelerating lung function decline.1 Although infections with respiratory viruses are the major cause of bronchial asthma exacerbation, other environmental and host-related factors may be involved as well.2 Pathomechanisms associated with asthma exacerbation have not been elucidated and several mechanisms seem to operate including enhanced inflammation, increased mucus hypersecretion and bronchial hyperresponsiveness.34 Associations between T-cell-related immunological parameters and asthma exacerbations have been reported, suggesting that T cells play a significant role in controlling the inflammatory process.5 Although some clinical traits may help assess the risk of asthma deterioration in a given patient, it is important to develop new non-invasive biomarkers to predict asthma exacerbation.
MicroRNAs (miRNAs) are short non-coding RNAs, which regulate various cell functions by tuning specific target genes responsible for the production of cytokines orchestrating cell activity.6 The miRNAs can be effectively delivered to a target cell or a tissue from a host cell via extracellular vesicles, which are detected in blood, exhaled breath condensates or bronchoalveolar lavage fluid (BALF).7 Differential expression of several miRNAs in serum and biological fluids (BALF, induced sputum) from asthmatics as compared to healthy controls have been documented.891011 Although it has been proposed that miRNAs may serve as potential biomarkers and therapeutic targets in asthma, few studies have addressed the role of miRNA in asthma exacerbation.12
In order to study the potential involvement of miRNA in immunological dysregulation associated with asthma exacerbation, we selected 7 miRNAs, which have previously been associated with immunological and clinical traits of bronchial asthma in either experimental or clinical models of the disease.1314151617 We hypothesized that asthma exacerbation is associated with dysregulated serum miRNA expression, which in turn may affect the immune profile of peripheral blood T cells and the development of airway inflammation.
MATERIALS AND METHODS
Patients and study design
In a prospective observational study, 25 patients with asthma, diagnosed according to the Global Initiative for the Asthma (GINA) criteria,18 were admitted for an unplanned visit due to exacerbation defined in line with the European Respiratory Society/American Thoracic Society (ERS/ATS) recommendations.19 At the exacerbation visit (EV), the evaluation included the Asthma Control Test (ACT) and modified Medical Research Council (mMRC) score recording. Moreover, spirometry, fractional exhaled nitric oxide (FeNO) measurement, blood withdrawal and nasopharyngeal swab collection were performed. Six to 8 weeks later, when patients recovered from exacerbation, they were readmitted for the follow-up assessment (FV), during which the same parameters were recorded. A diagnosis of atopy was based on the presence of at least 1 positive prick skin test out of 10 inhalant allergens. The study was approved by the local Bioethics Committee and all study subjects provided their informed consent. The clinical and demographic characteristics of the patients are presented in Table 1. Details on patient recruitment and their clinical assessment are described in Supplementary Data S1.
Table 1
Demographic and clinical characteristics of the patients
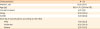
Data are shown as mean ± standard deviation or number (%).
N-ERD, non-steroidal anti-inflammatory drugs Exacerbated Respiratory Disease; GINA, Global Initiative for Asthma.
![]()
Analysis of miRNA expression in serum
In this study, miRNA was isolated from serum with an miRCURY RNA Isolation Kit-Biofluids (Exiqon, Vedbaek, Denmark) according to the manufacturer's protocol, and quantitative polymerase chain reaction (PCR) was performed (StepOne Plus; Applied Biosystems, Foster City, CA, USA; ThermoFisher Scientific, Inc., Waltham, MA, USA) with miRNA-93 as a reference gene. Serum expression levels were evaluated for miRNA-146a, -126a, -29a, -29b, -29c, -21 and -16 with real-time PCR (RT-PCR).
Immuno-phenotyping and intracellular cytokine staining
Peripheral blood mononuclear cells (PBMCs) isolated from whole blood were phenotyped using a mixture of antibodies (anti-cluster of differentiation (CD)4, anti-CD279, anti-CD45RA, anti-CD45RO, anti-interleukin (IL)-21R, anti-CXC chemokine receptors (CXCR)-5 and anti-CD27 in order to obtain the number of Th-follicular, T-naïve, Th-memory and Th- regulatory cells. For Th17/Treg assessment, a Th17/Treg Phenotyping Kit was used. The number of eosinophil progenitors expressing toll-like receptor (TLR)-2 and TLR-4 in whole blood samples was determined with a cocktail of anti-CD45, anti-CD34, anti-CD125, anti-TLR2 and anti-TLR4 antibodies. For intracellular cytokine staining, PBMCs were suspended in Roswell Park Memorial Institute medium with 10% fetal bovine serum or stimulated with phorbol myristate acetate plus ionomycin, and incubated with the mixture of antibodies directed against intracellular antigens (anti-interferon gamma [INFγ], anti-IL-4, anti-IL-17A, anti-IL-9 and anti-IL-22). All samples were measured on a BD™ LSR Fortessa flow cytometer and the results were analyzed with BD FACSDIVA™ software.
Details on miRNA expression analysis and flow cytometry immunophenotyping are depicted in Supplementary Data S2.
Pathogen detection in nasopharyngeal fluid (NPF)
In NPF, mRNAs for 16 viruses were assayed with RT-PCR, and bacteria were detected by standard microbiology culture (Supplementary Data S3).
Statistical analysis
Comparisons between groups were made with the non-parametric Mann-Whitney U test. The Wilcoxon signed-rank test was used to compare results at the first and second visits. The Spearman rank correlation was used to evaluate the correlation between variables. The results are expressed as median and 25th to 75th percentiles. All statistical analyses were performed using Statistica (Statsoft, Inc., Tulsa, OK, USA). P values of <0.05 were considered statistically significant.
RESULTS
Clinical characteristics of the exacerbations
Out of 25 patients with asthma exacerbation recruited for the study, 21 were evaluated at the FV (3 patients did not show at this visit, 1 subject did not show any clinical improvement). Fourteen patients (66.7%) were diagnosed as having moderate to severe exacerbation according to the GINA criteria. At the FV, patients reported improvement in asthma control expressed by overall increase in ACT, lower mMRC score, significantly higher first second of forced expiration ratio (FEV1%) predicted and forced vital capacity ratio (FVC%) predicted than at the EV. The overall FeNO level was not changed; in 5 patients, however, a significant decrease in FeNO was observed according to the ATS/ERS criteria (Table 2).
Table 2
Comparison of asthma control, spirometry and airway inflammation at the EV and the FV
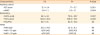
Data are shown as mean ± standard deviation or number (%).
EV, exacerbation visit; FV, follow-up visit; ACT, Asthma Control Test; mMRC, modified Medical Research Council; FEV1, first second of forced expiration; FVC, forced vital capacity; FeNO, fractional exhaled nitric oxide; NS, not significant.
![]()
Serum miRNA expression is related to airway inflammation and respiratory function during asthma exacerbation
The mean expression of serum miRNA-126a, miRNA-16 and miRNA-21 was significantly higher at the EV than at the FV (Fig. 1), while the remaining 4 miRNAs tested were unchanged. The serum expression of miRNA-29b positively correlated with FeNO (r = 0.44, P < 0.05), and in patients with FeNO levels > 25 parts per billion (ppb), expressions of miRNA-29a, miRNA-29b, miRNA-29c and miRNA-21 in serum were significantly higher as compared to patients with lower FeNO levels (Fig. 2). Patients with a significant decrease in FeNO at the FV had higher miRNA-126a (2.15 ± 1.44 vs. 0.71 ± 0.72, P = 0.02).
 | Fig. 1Significant decreases in the expression level of 3 miRNAs at the FV as compared to the EV. Differences were analyzed using the Wilcoxon signed rank test.EV, exacerbation visit; FV, follow-up visit; miRNA, microRNA.
|
 | Fig. 2(A) Positive correlations between miRNA-29b expression in serum and FeNO (ppb). (B) Decreases in serum miRNA expression in patients with low (FeNO < 25 ppb) as compared to patients with high (FeNO > 25 ppb) levels of airway inflammation at the EV. Differences were analyzed using the Mann-Whitney U test.miRNA, microRNA; FeNO, fractional exhaled nitric oxide; ppb, parts per billion.
|
At the EV, but not at the FV, positive correlations were observed between FEV1/FVC and the serum expression of 5 out of 7 miRNAs tested: miRNA-146a (r = 0.47, P < 0.05), miRNA-126a (r = 0.6, P < 0.05), miRNA-29a (r = 0.56, P < 0.05), miRNA-29b (r = 0.49, P < 0.05), miRNA-21 (r = 0.6, P < 0.05) and 2 miRNAs (miRNA-126a and miRNA-21) additionally correlated with FEV1% predicted (Fig. 3). Furthermore, the expression of miRNA-21 was significantly lower in patients with FEV1 below 60% of the predicted value as compared to those with higher FEV1 (0.42 ± 0.27 vs. 1.98 ± 2.36, P = 0.046).
 | Fig. 3Positive correlations between serum levels of miRNA-21 and miRNA-126a and respiratory function (FEV1% of predicted value) at the exacerbation visit.miRNA, microRNA; FEV1, first second of forced expiration.
|
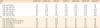
Interestingly, the mean expression of miRNA-29a, miRNA-29b, miRNA-29c and miRNA-21 in the serum of atopic patients was significantly higher as compared to non-atopic patients at both visits (Table 3).
Table 3
Differences in serum miRNA expression between atopic and non-atopic asthmatics at the EV and the FV

Differences were analyzed using Mann-Whitney U test.
miRNA, micro RNA; EV, exacerbation visit; FV, follow-up visit; NS, not significant.
![]()
T-cell-related immunological parameters in asthma exacerbation and control
Out of 19 T-cell-related parameters tested in isolated PBMCs, only the number of CD45+CD4+IL4+ (expressed as % of CD4+) cells was significantly larger) at the EV than at the FV (12.5 ± 16.2 vs. 4.5 ± 7.2, P = 0.01). Severe exacerbations were associated with a higher number of CD8+INFγ+ cells (% of CD8+) (4.5 ± 2.98 vs. 0.81 ± 1.39, P = 0.024). The remaining parameters were not affected by asthma exacerbation.
The mean number of CD4+Foxp3+ cells (% of CD4+) correlated positively with ACT (r = 0.53; P < 0.05) at the EV and at the FV, which significantly increased (from 12.37 ± 3.87 to 19.28 9.71, P = 0.021) in patients with improvement in ACT score (>20%). At the FV, the mean number of Th IL-17 cells correlated positively with ACT score and FVC %predicted. (r = 0.53, P < 0.05 and r = 0.45, P < 0.05, respectively) and negatively with mMRC (r = −0.53, P < 0.05). CD45+CD4+INFγ+ cells correlated positively with mMRC (r = 0.49, P < 0.05). The number of eosinophil progenitor cells (CD45+CD34+CD125+) correlated positively with ACT (r = 0.5, P < 0.05) and negatively with mMRC (r = −0.55, P < 0.05) at the EV.
IL-22 expression in T cells and eosinophil progenitors is associated with asthma phenotypes
Atopic patients at the EV had on average 33-fold lower number of CD8+ cells expressing IL-22 (expressed as % of CD8+) (0.15 ± 0.18 vs. 5 ± 9.18, P = 0.037) and 8 -fold lower number of CD4+ IL-22+ cells (expressed as % of CD4+) (0.43 ± 0.7 vs. 3.38 ± 4.1, P = 0.014) than non-atopic subjects. Patients with non-steroidal anti-inflammatory drug (NSAID)-exacerbated respiratory disease at the EV had on average 3-fold lower number of eosinophil progenitor cells (% of CD 45+) (0.014 ± 0.011 vs. 0.047 ± 0.064, P = 0.048) than NSAID-tolerant patients.
Differential correlation between the T-cell cytokine expression and circulating miRNA levels during asthma exacerbation and convalescence
During exacerbation, most consistent were negative correlations of the number of T cells (both CD4+ and CD8+) expressing IL-22 and IL-4 with serum levels of miRNA (each expression of the 2 cytokines correlated with 1-6 miRNAs tested) (Table 4). In addition, the mean number of CD4+ cells expressing interferon gamma (IFN-γ) negatively correlated with 6 out of 7 miRNAs and the number of CD4+ cells expressing IL-17 correlated with 4 serum miRNAs.
Table 4
Correlations between the number of T-cell subsets and serum miRNA expression (2^-DCt) at the EV and the FV (all P < 0.05)
miRNA, micro RNA; EV, exacerbation visit; FV, follow-up visit; NS, not significant; CD, cluster of differentiation; IL, interleukin; INF, interferon; CXCR, CXC chemokine receptors; PD, programmed death.
![]()
At the FV, CD8+ cells expressing IL-9 positively correlated with 3 of 7 miRNAs tested (miRNA-21, miRNA-29b and miRNA-29c). The percentage of Tfh (CD4+CXCR5high/programmed death-1+) cells correlated positively with miRNA-146a and miRNA-16, while the number of naïve CD4 cells (CD4+CD45RA+/CD45RO−) correlated with the expression of miRNA-16. Negative associations were found between the number of CD4+IL-4+ cells and miRNA-146a expression, and between CD4+CD25+ cells and miRNA-16.
Viral and bacterial detection rates in NPF were similar at the EV and the FV (Supplementary Data S3), and were not associated with any clinical, functional or immunological parameters.
DISCUSSION
In this study, we documented that asthma exacerbation is associated with epigenetic dysregulation expressed by changes in circulating miRNA. Furthermore, miRNA expression correlated with the clinical/inflammatory characteristics of asthma patients and patterns of T-cell cytokine expression.
The miRNAs play a well-documented regulatory role in controlling functions of cells associated with airway inflammation and are strongly modulated by viral infections, which suggests their potential contribution to the pathogenesis of asthma exacerbation.20 In our patients, the expression of circulating miRNAs during asthma exacerbation was associated with the objective parameters of disease severity: subjects with low FEV1 (below 60% of the predicted value) exhibited 5-fold lower expression of miRNA-21 than those with better respiratory function, while those with FeNO levels > 25 ppb had significantly increased expressions of miRNA-29a, miRNA-29b, miRNA-29c and miRNA-21. Interestingly, a different pattern of correlation was observed at the FV. Furthermore, the expression of miRNA-126a, miRNA-16 and miRNA-21 significantly decreased in parallel to improvement in clinical symptoms at the FV, and patients with a significant decrease in FeNO level demonstrated 3-fold higher expression of miRNA-126a, suggesting its role in the modulation of airway inflammation. An interesting observation is that 5 miRNAs, which during exacerbation negatively correlated with FeNO, showed a positive correlation with respiratory function assessed by spirometry: higher serum expression of miRNA-21, miRNA-29a, miRNA-29b (but not miRNA-29c), miRNA-126a and miRNA-146a predicted less airway obstruction, suggesting the differential regulation of airway obstruction and inflammation by miRNA.
The miRNAs, whose expression in our study demonstrated associations with various traits of asthma exacerbation, could be potentially involved in asthma pathogenesis as documented by experimental and/or clinical studies.21 For example, miRNA-21, which has been shown to regulate immune polarization, directly targets IL-12p35 reducing the production of Th1 cytokines and increasing signaling through the Th2 pathway.22 The miRNA-21 and miRNA-126a are overexpressed in bronchial epithelial cells obtained from asthmatic airways, and non-treated asthma patients express miRNA-21 to a significantly greater extent than those using inhaled corticosteroids.23 Hammad Mahmoud Hammad et al.24 found significant up-regulation of plasma miRNA-21 and miRNA-146a levels in children with asthma as compared to controls, and demonstrated that both miRNA levels were positively correlated with blood eosinophilia, miRNA-21 and IL-13 levels. Elbehidy et al.25 reported that serum miRNA-21 expression levels were negatively correlated with serum IL-12p35 levels and FEV1, while they were positively correlated with both sputum and blood eosinophils. The miRNA-21 was not associated with asthma exacerbation in our study, but showed a positive correlation with respiratory function.
The members of the miR-29 family, which in our study were associated with the levels of FeNO, a ventilatory parameter, may have multiple functions related to the pathogenesis of asthma exacerbation. The miRNA-29 is involved in controlling innate and acquired immune responses and can be activated by IFN signaling, which suggests its role in response to viral infections typical for asthma exacerbation.26 Furthermore, the overexpression of miRNA-29 may induce the expression of COX2 and increase generation of prostaglandin E2.27 The study of Zhang et al.28 assessing miRNA expression during asthma exacerbation in children found significantly decreased levels of miRNA-29c expression in PBMCs and documented its role in the regulation of Th2/Th17-cell differentiation.
More recently, Kho et al.12 identified, in the sera of children with asthma, 12 miRNAs which were significantly associated with asthma exacerbations in the subsequent year; doubling the expression of each miRNA was associated with 25%-67% increases in the risk of exacerbation. This data suggest that the assessment of the expression of these miRNAs in serum has the potential to identify reliable biomarkers for asthma exacerbation.
The inflammatory process in the airways during asthma exacerbation has a complicated nature, and multiple cells and secreted cytokines may be involved.2930 The dominant model of inflammation in asthmatics (Th1-, Th2- or Th17-dependent) can be temporarily modulated by reactions to infections or environmental exposure responsible for disease exacerbation. We found that among analyzed cells, only Th-secreting IL-4 levels were higher during the exacerbation. IL 4- is a key cytokine responsible for the differentiation of Th2 lymphocytes from naive T cells and helping maintain Th2-dependent inflammation.31 Indirectly, inhibition of both IL-4 and IL-13 signaling resulted in the reduction in the frequency of asthma exacerbation.32 From other cell subsets, we detected that CD4+Foxp3+ and Th17 lymphocytes were correlated with better asthma control (probably related to their regulatory activity) and CD8+INF-secreting cells were connected with severe asthma exacerbation and worsened asthma control (probably as a vivid proinflammatory response to viral infection). IL-22 is an IL-10-family cytokine produced by a variety of cells including Th17 cells, γδ T cells and ILC3.33 IL-22 seems to play an important role in the pathogenesis of airway inflammation by regulating epithelial function. We found that atopic subjects had a significantly decreased level of CD4+ cells expressing IL-22, which suggests that in allergic patients, it may be one of the most important regulatory mechanisms maintaining anti-inflammatory response and that loss of the function of those cells may result in exacerbation. These observations seem to confirm heterogeneity in inflammatory patterns during asthma exacerbation in patients with various disease phenotypes.3435
Importantly, the number of T cells expressing specific cytokines was significantly associated with circulating miRNA: during exacerbation, inverse correlations between miRNA expression and the number of T cells expressing specific cytokines were observed, while both positive and negative correlations were seen at the follow-up visits. Associations between the miRNA expression and T-cell cytokine expression observed by other authors us support the hypothesis that miRNA may contribute to the pathogenesis of asthma exacerbation by modulating the inflammatory process and transferring the signal from inflammatory cells (T cells) to structure cells.
We are aware that our data should be interpreted with caution, since the study has several limitations: 1) Patients were studied at various points of deterioration of asthma symptoms, thus it is possible that some changes have been missed due to different time points; 2) Before admission, some patients had received pharmacological treatment (including oral corticosteroids), which might have affected the immune parameters studied. However, 5 patients who had received oral corticosteroids before admission had miRNA expression and T-cell cytokines expression similar to those not receiving corticosteroids; at the first visit; and 3) Only selected miRNAs were studied, thus further extension of miRNA profiles may provide a better insight into epigenetic dysregulation associated with asthma exacerbation.
In conclusion, we have documented that circulating miRNA expression is modulated during asthma exacerbation and is associated with certain clinical, inflammatory and immunological parameters of asthma. Further studies may determine whether miRNA expression levels in plasma could be used as a marker of asthma activity and/or as a prognostic marker of exacerbation. The results suggest that miRNA mimics or antagomirs may be attractive candidates for preclinical studies as an anti-inflammatory treatment of asthma.
 XML Download
XML Download