

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Many patients with type 2 diabetes are at increased risk of cardiovascular disease (CVD) due to multiple concomitant factors.12 Diabetic dyslipidemia is one of the main modifiable risk factors for CVD. Therapy for diabetic dyslipidemia among patients with type 2 diabetes is primarily directed at lowering serum low-density lipoprotein (LDL) cholesterol levels (<2.6 mmol/L) using a statin.34 However, despite achieving their target goal for LDL cholesterol, statin-treated patients with diabetes can remain at risk because of persistent hypertriglyceridemia and elevated non-high-density lipoprotein (HDL) cholesterol.567 For patients with diabetes whose hypertriglyceridemia persists after their LDL cholesterol improves with statin treatment, a triglyceride (TG) lowering agent can be added to the treatment, along with lifestyle modifications.
Omega-3 fatty acids are polyunsaturated essential fatty acids, including eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Several epidemiological studies have reported that omega-3 fatty acids can lower CVD prevalence and mortality in the general population.8910 In patients with type 2 diabetes, omega-3 fatty acid supplements can also attenuate CVD risk factors such as dyslipidemia, inflammation, and thrombogenic issues without worsening glycemic control or insulin sensitivity, although the potential long-term benefit of omega-3 fatty acids in preventing major CVD outcomes is controversial.1112 In addition to monotherapy, recent studies have shown the possibility of incremental benefit in reducing CVD events from adding omega-3 fatty acids to conventional statin treatment.1314 In patients with persistent hypertriglyceridemia during statin therapy, the Combination of Prescription Omega-3 plus Simvastatin (COMBOS) trial showed that co-administering omega-3 fatty acids with a statin was associated with greater lipid profile improvements than treatment with a statin alone.15 In contrast to the potential adverse effects from combining statins with fibrate,16 combination therapy with omega-3 fatty acids and a statin showed few adverse events.
Those findings suggest that combination therapy with omega-3 fatty acids and a statin would be a reasonable option for patients with diabetes who do not achieve their goals for TGs and non-HDL cholesterol as secondary targets. However, few available clinical outcome data are available for patients with type 2 diabetes. In addition, several studies have shown that LDL cholesterol levels tended to rise with DHA intake.1718 Statin therapy was also associated with an increased risk of new-onset diabetes,1920 raising concerns that patients with type 2 diabetes on long-term combination therapy with omega-3 fatty acids and a statin might experience undesirable effects on their glycemic control and LDL cholesterol. We hypothesized that combining omega-3 fatty acids with a statin would be efficient in lowering TG levels without undesirable effects in type 2 diabetic patients who had hypertriglyceridemia despite well-controlled LDL cholesterol on stable statin therapy. To test this hypothesis, we compared the effects of combination therapy with those of statin monotherapy on TGs, non-HDL cholesterol, and other lipid levels and glycemic control status in patients with Korean type 2 diabetes who have persistent hypertriglyceridemia despite statin therapy. Also, we assessed the safety of combining omega-3 fatty acids with a statin.
MATERIALS AND METHODS
1. Study subjects
This study was a prospective, multicenter, open-label, placebo-controlled study. Eligibility criteria were listed as follows: men and women aged 18 to 80 years; diagnosed with type 2 diabetes; hemoglobin A1C (HbA1c) ≤10.0% upon initial examination; undergoing statin therapy for ≥6 weeks at the time of initial examination; and diagnosed with dyslipidemia, with TG levels of 1.7 to 5.6 mmol/L and an LDL cholesterol level of ≤2.6 mmol/L. Exclusion criteria were: diagnosed with type 1 diabetes; currently undergoing peroxisome proliferator-activated receptor-gamma agonist therapy; a serious CVD event such as acute myocardial infarction or unstable angina, in the past 6 months; taking medications known to affect lipid profiles, such as steroids (except constant maintenance dose), cyclosporine, erythromycin, and ketoconazole; hypersensitivity to medications used in the trial; muscular, hepatic, renal, pulmonary or gastrointestinal diseases, including myopathy (serum creatine kinase level >2-fold the upper normal limit), obstructive hepato-biliary disease, active liver disease (serum alanine aminotransferase, aspartate aminotransferase, or total bilirubin >2-fold the upper normal limit), nephritic syndrome or renal insufficiency (serum creatinine level >1.5 mg/dL), or chronic pancreatitis; a positive urine pregnancy test conducted during the initial examination or pregnancy; premenopausal women not practicing effective birth control or unwilling to practice effective birth control during the study; nursing mothers; active cancer treatment in the past 2 years; drastic changes in diabetes treatment; and other clinical trial medications taken in the past 3 months. This trial was conducted at 4 clinical research sites between February 2009 and February 2011 in Korea in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki (2000). The Institutional Review Boards (HC08MIMV0064) of each participating center approved the protocol before the study began, and informed consent was obtained from all subjects.
2. Study protocol
Subjects who were eligible and agreed to participate in the trial were randomly selected to receive omega-3 fatty acids or not concurrent with a statin for 16 weeks. Randomization was conducted using the block stratified randomization method. After randomization, the study processes were not blinded. Patients received either a statin plus 4 g of omega-3 fatty acids or a statin alone. The trial subjects visited the clinic 4, 8, and 16 weeks after registration. Any subject whose drug compliance was <80% at week 16 was dropped from the trial. All participants were co-administered oral hypoglycemic agents and statins and were asked to continue taking the medications at a constant dose. The statins used in the study included pravastatin, simvastatin, atorvastatin, and rosuvastatin. Detailed information about the statin prescriptions, including the types and doses used, is provided in Supplementary Table 1. The following medications were not permitted during the trial: additional oral hypoglycemic agents, newly administered corticosteroids, corticosteroids that could not be maintained at a constant dose during the trial, and all types of weight-loss medications.
After an overnight fast, plasma glucose, HbA1c, total cholesterol (TC), TG, and HDL cholesterol levels were measured. The serum samples collected from the trial centers were analyzed at a central laboratory. TC and TG levels were measured using an enzymatic colorimetric test. The serum levels of high-sensitivity C-reactive protein (hsCRP) and plasminogen activator inhibitor-1 (PAI-1) were measured using an enzyme-linked immunosorbent assay kit (Denka-Seiken Ltd., Tokyo, Japan), and the apolipoprotein (APO) A1 and B levels were determined using a turbidimetric immunoassay (Linco Research, St. Charles, MO, USA). We measured vital signs and body weight and assessed the occurrence of adverse events at each visit. Routine complete blood counts, blood chemistries, and urinalysis tests were also conducted to monitor drug safety.
The primary outcome evaluated was the ability of statin plus omega-3 fatty acid combination therapy to reduce TG levels in patients with type 2 diabetes who have persistent hypertriglyceridemia despite statin therapy. The secondary outcomes evaluated were the mean changes in TC, HDL cholesterol, LDL cholesterol, non-HDL cholesterol, APO A1 and B, hsCRP, PAI-1, and HbA1c levels. Safety evaluations included monitoring adverse events (including increased blood glucose), vital signs, a physical examination, and an evaluation of changes in clinical laboratory examination results. The targeted number of patients in the study was 70 (35 in each group), which was calculated based on a 10% difference in average changes in TG levels in the statin monotherapy group versus the combination therapy group, a 15% standard deviation, and a 20% dropout rate.
3. Statistical analysis
The outcomes data were analyzed using intention-to-treat (ITT) and per-protocol (PP) analyses. In the ITT analysis, all the data from subjects who had received at least 1 experimental treatment and clinical examination were included. The PP analysis included only data from those subjects who completed the study according to the clinical trial protocol. The ITT analysis was the main method of analysis, with the PP analysis used as an auxiliary method. We evaluated the differences between the combination therapy group and the statin monotherapy group using a t-test or Wilcoxon test for each continuous variable depending on data normality, and we tested the changes observed before and after the administration of omega-3 fatty acids or placebo within the groups using paired t-tests. Categorical variables are expressed as percentages, and the χ2 test or Fisher's exact test was used for comparison. The statistical analysis was performed using SAS 9.2 for Windows (SAS Institute Inc., Cary, NC, USA). The p-values <0.05 were considered statistically significant.
RESULTS
We screened 84 patients and randomized 62 of them. Three subjects from each group who did not undergo an efficacy evaluation were excluded. After the initial visit, a total of 56 patients (26 in the statin plus omega-3 fatty acids combination therapy group and 30 in the statin-only group) were included in the ITT analysis. The baseline characteristics of the study patients are shown in Table 1. There were no statistically significant differences in the baseline clinical and laboratory characteristics between the combination therapy group and the statin-only group.
Table 1
Baseline characteristics of the intention-to-treat population

Data are expressed as the mean±standard deviation or number (%).
BMI, body mass index; BP, blood pressure; HbA1c, hemoglobin A1C; TC, total cholesterol; TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein; APO, apolipoprotein; hsCRP, high-sensitivity C-reactive protein; PAI-1, plasminogen activator inhibitor-1.
*Log-transformed variables; †Unpaired t-test; ‡Wilcoxon rank sum test; §χ2 test.
As shown in Fig. 1, we analyzed the percentage change in the TG level as the primary efficacy outcome. In the ITT analysis of changes within the treatment groups, the TG level decreased by 34.8% at the end of the study in the combination therapy group, which was statistically significant. The statin-only group showed a 15.2% decrease, but that was not statistically significant. Comparing the 2 groups, the change in the TG level in the combination therapy group differed significantly from the change in the statin-only treatment group (p=0.0176). HDL cholesterol increased in both groups, but the changes between the groups did not differ significantly. The LDL cholesterol level decreased in the combination therapy group and increased in the statin-only group, but those changes were not statistically significant. Decreases in non-HDL cholesterol levels were observed in both groups, but there was no statistically significant difference between the groups.
Fig. 1
Changes from the baseline values for TGs, HDL, LDL, and non-HDL cholesterol at the end of the 16-week study.
TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein.

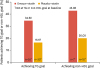
In the combination therapy group, 34.6% of the patients reached the goal of TGs ≤1.7 mmol/L; in the statin-only group, 16.6% of the patients reached that goal. A total of 19 patients in the combination therapy group and 20 in the statin-only group were at their non-HDL-cholesterol goal at baseline. In the subgroup of patients who were not at their non-HDL-cholesterol goal at baseline, 42.8% of patients in the combination therapy group attained it by the end of treatment, compared with 20% of those in the statin-only group (Fig. 2).
Fig. 2
Percentage of patients achieving their TG and non-HDL cholesterol goals at end of treatment.
TG, triglyceride; HDL, high-density lipoprotein.
As shown in Table 2, the absolute and percentage decreases in APO B and A1 were greater in the combination therapy group, but those changes were not statistically significant. In both groups, hsCRP and PAI-1 levels did not change significantly during the study period. Fasting plasma glucose and HbA1c levels increased more in the combination therapy group than in the statin-only group, but those changes were not statistically significant. The PP analysis showed no statistically significant differences within or between the treatment groups in the changes seen in the secondary efficacy variables.
Table 2
The percent change from the baseline values for the lipid profiles at the end of the 16-week study

Values are presented as mean±standard deviation or 95% confidence interval.
APO, apolipoprotein; TC, total cholesterol; HDL, high-density lipoprotein; hsCRP, high-sensitivity C-reactive protein; PAI-1, plasminogen activator inhibitor-1; HbA1c, hemoglobin A1C.
*Test for difference between the 2 intervention groups; †Test for difference between baseline and 16 weeks in each group; ‡Unpaired t-test; §Wilcoxon rank sum test; ‖Paired t-test; ¶Signed rank test.
A total of 56 subjects (26 in the combination therapy group and 30 in the statin-only group) were included in the safety evaluation (Supplementary Table 2). An analysis of adverse events after the administration of the clinical trial agents demonstrated that 16 (61.5%) subjects in the combination therapy group experienced 30 adverse events (mild, 22; moderate, 7; severe, 1). A total of 23 adverse events (mild, 13; moderate, 9; severe, 1) occurred in 10 (33.3%) subjects in the statin-only group. The difference between the 2 groups was statistically significant (p=0.0138), but there were no statistically significant differences in treatment-related adverse events, severe adverse events, or adverse events leading to trial dropout. In the combination therapy group, 3 adverse events in 3 patients (9.1%) were determined to be treatment related, with 1 case each of dyspepsia, diarrhea, and oral discomfort. Serious adverse events occurred in 4 patients (12.1%) in the combination therapy group and 2 patients (6.1%) in the statin-only group; the proportion in the combination therapy group was higher, but all serious adverse events were determined to be unrelated to the treatment. Of the 6 cases of adverse events that led to dropout from the clinical trial, 5 were unrelated to the treatment, and the 1 case of oral discomfort was a predicted adverse event. There were no statistically significant changes in vital signs or physical examination findings after the trial within each group compared to baseline or between the treatment groups.
DISCUSSION
In this study, we assessed the safety and efficacy of adding omega-3 fatty acid treatment to statin therapy to reduce the TG and non-HDL cholesterol levels of patients with type 2 diabetes and persistent hypertriglyceridemia despite statin therapy. The ITT analysis showed that the TG levels decreased significantly in the combination therapy group after treatment; the 34.8% decrease was 20% larger than the decrease in the statin-only group. These results are consistent with those of several prior studies that added 4 g of omega-3 fatty acids to simvastatin treatment (10–40 mg) for 6 to 24 weeks and found that the combination therapy was up to 45% more effective at reducing TGs than statin monotherapy. Our results confirm that combination therapy reduces TGs more effectively than statin monotherapy.
In our combination group, the LDL cholesterol levels decreased slightly, but those changes were not statistically significant. Previous studies have reported that omega-3 fatty acid monotherapy could increase LDL cholesterol,1721 possibly by changing the cholesterol composition from TG-rich lipoproteins to LDL particles.22 However, in our combination therapy group, the decrease in cholesterol biosynthesis caused by the statin might have limited the effect of omega-3 fatty acids on LDL cholesterol, so we observed no significant differences.
In the ITT analysis of this study, the combination therapy group showed non-significant increases in HbA1c and fasting plasma glucose levels after 16 weeks, but those changes did not differ significantly from those in the statin-only group. A PP analysis revealed no statistically significant differences within either group or between the 2 groups. It has been reported that excess (8 g/day) omega-3 fatty acid administration leads to decreased TGs and increased fasting plasma glucose and postprandial plasma glucose levels in patients with type 2 diabetes.23 In the COMBOS trial, combination therapy with omega-3 fatty acids (4 g) and simvastatin (40 mg) resulted in increased fasting plasma glucose levels. Their post-hoc analysis found no significant differences in fructosamine.15 However, that trial's limitations, such as a short observation period of only 8 weeks and the exclusion of subjects with insufficient glycemic control (HbA1c ≥8% at initial examination), must be considered. In our study, in which HbA1c was observed for 16 weeks, the combination therapy group did not show a statistically significant increase in HbA1c, which is in keeping with previous studies that reported that omega-3 fatty acid consumption minimally affects glycemic control in patients with type 2 diabetes. However, because we did not control for confounding factors such as the subjects' lifestyles, caloric intake, or physical activity and because the dose of hypoglycemic agents administered was not standardized across subjects, we cannot exclude the possibility that those factors affected the HbA1c changes. Based on our results, additional studies comparing the effects of combination therapy and statin monotherapy need to be performed in patients with type 2 diabetes and hypertriglyceridemia while controlling for factors that can affect glycemic control.
Regarding hsCRP, a representative surrogate marker for CVD, we found no statistically significant differences between the treatment groups or significant changes within either group. Additionally, PAI-1, which is another predictive indicator of CVD,24 increased slightly in the combination therapy group (12.3%, p=0.0523). Few studies have evaluated the effects of omega-3 fatty acids on PAI-1, and the results of those few are controversial. In a previous study of patients with type 2 diabetes, the group that received omega-3 fatty acids (3 g) demonstrated statistically significant increases in PAI-1 compared to the control group, which suggests that omega-3 fatty acids might directly affect fibrinolytic activity.25 However, in a study comparing EPA and DHA purified from fish oil, those 2 main omega-3 fatty acids did not significantly affect fibrinolytic functions such as PAI-1 concentration and platelet aggregation.26 In another recent study, the combination of pitavastatin and EPA effectively prevented vascular complications by significantly decreasing platelet-derived microparticles and significantly increasing adiponectin.27 In patients with type 2 diabetes, hyperglycemia, hyperinsulinemia, obesity, and hypertriglyceridemia can indirectly affect PAI-1 synthesis and secretion, and studies have reported that the PAI-1 level is significantly reduced in patients with type 2 diabetes whose hyperglycemia has been controlled.28 Therefore, in this study, the increases in PAI-1 seen in the combination therapy group might have been related to increases in HbA1c. Additional studies are needed in this area.
In our safety evaluation, we found no statistically significant differences between the 2 groups in terms of treatment-related adverse events, serious adverse events, or adverse events that led to dropout from the clinical trial. Of the 6 cases of adverse events that led to trial dropout, 5 were determined to be unrelated to the treatment, and the other was a case of oral discomfort. The limitations of this study are as follows. Because it was an open-label trial, biases cannot be excluded. Additionally, because the study duration was short, we were unable to assess long-term efficacy and tolerability. The causal relationship between statins and the development of diabetes is receiving more attention. Therefore, more precise, long-term, large, randomized, controlled trials evaluating whether combination therapies of omega-3 fatty acids and statins negatively affect glycemic control and whether they have synergistic protective effects for CVD compared with statin monotherapy are necessary. Furthermore, whether EPA and DHA have different effects on the risk of CVD should be assessed. Recent trials have shown that supplementation with EPA and DHA offered no benefits for the prevention of myocardial infarction, stroke, or cardiovascular death.29 On the other hand, supplementation with 2 g of highly purified ethyl-EPA twice daily lowered the risk of major ischemic events, including cardiovascular death, among patients with elevated TG levels who were receiving statin therapy.30
In conclusion, we have demonstrated that combining omega-3 fatty acids with a statin in patients with type 2 diabetes and dyslipidemia was more effective than statin monotherapy in decreasing TG levels. The safety and tolerability of the combination treatment were comparable to statin monotherapy. Although concerns about long-term glycemic control remain, statin plus omega-3 fatty acid combination therapy could be a reasonable way to decrease the risk of CVD in patients with type 2 diabetes and persistent hypertriglyceridemia despite statin therapy.
 XML Download
XML Download