

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The effectiveness of statin therapy in secondary prevention has been clearly demonstrated, and trials have shown the benefits of intensive statin therapy in patients with acute coronary syndrome (ACS).12 Therefore, all patients with ACS are recommended to receive high-intensity statin therapy irrespective of baseline low-density lipoprotein (LDL) cholesterol level.3 The treatment goal is LDL cholesterol <70 mg/dL or at least 50% reduction in LDL cholesterol if the baseline level is 70–135 mg/dL.3 Statin therapy after ACS was also beneficial in patients with baseline LDL cholesterol level <70 mg/dL or even ≤50 mg/dL.45 However, for this ACS subset with very low LDL cholesterol level at presentation, data supporting a specific recommendation on the intensity of statin therapy are lacking. In the present study, we hypothesized that more intensive statin therapy would be beneficial in the patients with acute myocardial infarction (MI) even when the baseline LDL cholesterol level is very low. Therefore, we assessed the clinical effects of statin intensity in patients with acute MI and baseline LDL cholesterol <70 mg/dL using a large-scale, multi-center, nationwide, acute MI database in Korea. We hypothesized that more intensive statin therapy would be beneficial in the patients with acute MI even when the baseline LDL cholesterol level is very low.
MATERIALS AND METHODS
1. Study population and data collection
The study population was obtained from the Korea Acute Myocardial Infarction Registry-National Institutes of Health (KAMIR-NIH) database between November 2011 and December 2015. The KAMIR-NIH is a prospective, open, online, multi-center data collection registry from 20 tertiary university hospitals in Korea capable of percutaneous coronary intervention (PCI) and designed to capture real-world treatment practices and outcomes of patients with acute MI.6 Acute MI was diagnosed in the presence of an increase or decrease in cardiac biomarker value (troponin I/T or creatine kinase-MB with at least one value above the 99th percentile upper reference limit) and at least one of the following: symptoms of myocardial ischemia, changes on electrocardiogram (ECG) including new or presumed new significant ST-segment-T wave changes, new left bundle branch block or pathologic Q waves in two contiguous leads, and imaging evidence of new loss of viable myocardium or a new regional wall motion abnormality.7
We identified a total of 1,778 patients with acute MI and baseline LDL cholesterol <70 mg/dL. Patients who did not receive statin therapy, received lipid-lowering therapy other than statins, were lost to clinical follow-up, discontinued statin therapy, or whose statin doses were not available were excluded. The remaining 1,086 patients were included in the study and divided into two groups based on intensity of statin therapy initiated at admission. Among the study patients, 75% received moderate-intensity statins, 23% received high-intensity, and 2% received low-intensity statins. Most of the high-intensity statins consisted of atorvastatin 40 mg (12%) or rosuvastatin 20 mg (10%) rather than the maximum doses of atorvastatin 80 mg (1%) or rosuvastatin 40 mg (0%, unavailable in Korea).8 To determine if intensity-dependent efficacy of statins occurred, the study population was divided into less intensive statin (n=302) and more intensive statin (n=784) groups. Less intensive statins were defined as those expected to reduce LDL cholesterol by approximately <40% and include the following daily doses: atorvastatin 10 mg, pitavastatin 1–2 mg, simvastatin 20 mg, pravastatin 5–40 mg, and fluvastatin 20–80 mg. More intensive statins were defined as those lowering LDL cholesterol by approximately ≥ 40% and include daily doses of atorvastatin 20–80 mg, rosuvastatin 5–20 mg, pitavastatin 4 mg, and simvastatin 40 mg.89 The study flow diagram is shown in Fig. 1.
 | Fig. 1The study flow diagram of the patients.KAMIR-NIH, Korea Acute Myocardial Infarction Registry-National Institute of Health; LDL, low-density lipoprotein.
|
PCI was performed according to the standard guidelines.10 Patients received loading doses of aspirin (300 mg) and P2Y12 blocker (ticagrelor 180 mg, prasugrel 60 mg, or clopidogrel 300–600 mg) before PCI. Selection of vessels treated, devices used, and adjunctive drugs administered to support PCI were performed by the treating physician. After PCI, patients received maintenance doses of either ticagrelor (90 mg twice daily), prasugrel (10 mg daily), or clopidogrel (75 mg daily) for at least 12 months. Aspirin was given at a dose of 100 mg daily indefinitely. The present study was conducted according to the Declaration of Helsinki. The Institutional Review Boards of all participating centers approved the study protocol. The approval number was CNUH-2011-172 of Chonnam National University Hospital. Written informed consent was obtained from all participating patients.
2. Clinical endpoints and definitions
The primary endpoint was major adverse cardiac and cerebrovascular event (MACCE) at 12 months. MACCE was defined as a composite of cardiac death, nonfatal MI, coronary revascularization by PCI or coronary artery bypass graft (CABG) occurring at least 30 days after admission, and nonfatal stroke. The secondary endpoints were cardiac death, nonfatal MI, coronary revascularization either by PCI or CABG occurring at least 30 days after admission, stent thrombosis, nonfatal stroke, and Thrombolysis in Myocardial Infarction (TIMI) major bleeding event at 12 months.
MI was defined as recurrence of symptoms or new ischemic ECG changes associated with an increase in cardiac biomarker level above the upper limit of normal in patients whose biomarker level had returned to normal or a ≥20% increase of the value if the initially elevated value was stable or decreasing.7 Target-lesion revascularization was defined as a repeat PCI in the same coronary segment as the index procedure. Target-vessel revascularization was defined as a repeat PCI in any segment within the major coronary vessel proximal and distal to the target lesion, including the target lesion itself. Stroke was defined as an acute episode of focal dysfunction of the brain, retina, or spinal cord lasting >24 hours or any duration if imaging or autopsy showed focal infarction or hemorrhage relevant to the symptoms.11 Stent thrombosis was defined according to the Academic Research Consortium definitions.12 Bleeding events were classified as major and minor according to TIMI scales.13
3. Statistical analysis
Continuous variables were expressed as mean±standard deviation and were compared between the two groups using Student's t-test when normally distributed; values were expressed as median (interquartile range) and compared using the Mann-Whitney U test when the data did not fit a normal distribution. Categorical variables were reported as numbers and percentages and were compared using the χ2 test or Fisher's exact test. Hazard ratio (HR) and 95% confidence interval (CI) were calculated for outcome variables using Cox regression analysis.
To adjust for the bias inherent to the decision of choosing less intensive vs. more intensive statin therapy, propensity scores were used.14 The propensity scores were estimated for the likelihood of receiving less intensive statin therapy using a multiple logistic regression model that contained the 51 covariates shown in Tables 1 and 2 (Supplementary Fig. 1). The C-statistic for the propensity model was 0.65, indicating fair ability to discriminate treatment groups. The Hosmer-Lemeshow goodness-of-fit test p-value was 0.16, confirming good calibration and fit of the multivariable model that estimated the propensity score. Matching was performed using a greedy matching protocol (1:2 nearest neighbor matching without replacement) with a caliper width of 0.2 of the standard deviation.15 We matched 302 patients receiving less intensive statin therapy to 604 patients receiving more intensive statin therapy. Standardized differences were estimated for all covariates before and after matching to assess the balance between the less intensive and more intensive statin groups. After matching, none of the covariates showed a standardized difference exceeding 10% (Fig. 1), indicating all the measured covariates were well balanced between the matched groups.16 Differences between the matched pairs were evaluated using the paired t-test or the Wilcoxon signed rank test for continuous variables and McNemar's test for categorical variables. The risks of clinical endpoints in the matched cohort were compared using a Cox proportional hazards regression model stratified on matched pairs, including factors considered significant (p-value <0.1) using univariate analysis or clinically important in the multivariate model.
Table 1
Baseline clinical characteristics and laboratory findings

Values are number (%), mean±standard deviation, or median (interquartile range).
CAD, coronary artery disease; hs-CRP, high-sensitivity C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; MI, myocardial infarction; GRACE, Global Registry of Acute Coronary Events.
![]()
Table 2
Angiographic and procedural characteristics and medical treatment during hospitalization

Values are number (%), mean±standard deviation or median (interquartile range).
ACC/AHA, American College of Cardiology/American Heart Association; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BMS, bare-metal stent; CABG, coronary artery bypass graft; DES, drug-eluting stent; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction.
![]()
The impact of statin intensity on the primary endpoint was further assessed in the following multiple subgroups: age, sex, clinical diagnosis, Killip class, diabetes, stroke, estimated glomerular filtration rate, left ventricular ejection fraction, high-sensitivity C-reactive protein (hs-CRP), and Global Registry of Acute Coronary Events (GRACE) score.17 For subgroup analysis, the same propensity score matching process was repeated when both the score and subgroup variables were matched, forcing exact matches on the subgroup characteristics. Conditional logistic regression was used to identify treatment-subgroup interactions. Time-varying measurements of LDL cholesterol and hs-CRP were analyzed using the generalized estimating equation model. Treatment effects over time were estimated with time, group, and time-group interactions, and the baseline values were used as covariates in the generalized estimating equation model for accommodating missing values.
All p-values were two-tailed, with statistical significance set at a level of <0.05. Statistical analyses were conducted using SPSS version 21 (SPSS Inc., Chicago, IL, USA) and R version 3.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
1. Patient characteristics
Baseline clinical, procedural characteristics, and treatment during hospitalization of the patients before and after propensity matching are shown in Tables 1 and 2. Overall, the patients in the less intensive statin group were older; more likely to be female; to have hypertension, lower hemoglobin level, higher GRACE score, and multivessel disease; and more often received clopidogrel. Patients in the more intensive statin group underwent stenting with drug-eluting stents and received ticagrelor more often than the patients in the less intensive statin group. In the 1:2 propensity-matched cohort (less intensive group, n=302, more intensive group, n=604), baseline characteristics were not statistically different between the two groups. Over 12 months of follow-up, 128 (11.8%) among the 1,086 patients switched between intensive and more intensive statins: 30 patients (2.8%) from less intensive to more intensive statins and 98 patients (9.0%) from more intensive to less intensive statins.
2. Lipid profile and hs-CRP
At baseline, median levels of LDL cholesterol and hs-CRP were not different in the two groups (59 mg/dL and 2.9 mg/L, respectively) in the propensity-matched cohort (Table 1). At 12 months, median LDL cholesterol level was significantly lower in the more intensive compared with the less intensive statin group (61 mg/dL vs. 67 mg/dL, p=0.032; Fig. 2A). Median level of hs-CRP was reduced to 0.7 mg/L and 0.9 mg/L in the more intensive and less intensive statin groups, respectively (p=0.651, Fig. 2B). Median high-density lipoprotein (HDL) cholesterol level increased during follow-up from 40 mg/dL at baseline in each group to 44 mg/dL in the more intensive statin group and 41 mg/dL in the less intensive statin group (p=0.232).
 | Fig. 2Changes in levels of LDL cholesterol (A) and hs-CRP (B) from baseline to 12 months in the propensity-matched cohort. Median (interquartile range) values in the two groups. The p-values are for interaction effects between treatment group and time.hs-CRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein.
|
3. Clinical outcomes
Unadjusted and adjusted clinical outcomes at 12 months before and after propensity score matching are shown in Table 3. The patients in the more intensive statin group had lower rates of coronary revascularization by PCI (7.3% vs. 4.1%, p=0.039); target-vessel revascularization (4.6% vs. 2.0%, p=0.029); cardiac death, MI, PCI, or CABG (8.6% vs. 5.0%, p=0.027); and MACCE (11.6% vs. 6.8%, p=0.010) compared with patients in the less intensive statin group. In the propensity-matched cohort, the more intensive statin group showed lower rates of target-lesion revascularization (3.3% vs. 1.2%, HR, 0.35; 95% CI, 0.13–0.91; p=0.032); target-vessel revascularization (4.6% vs. 1.8%, HR, 0.41; 95% CI, 0.19–0.90; p=0.027); cardiac death, MI, or stroke (7.6% vs. 4.3%, HR, 0.55; 95% CI, 0.32–0.97; p=0.039); and MACCE (11.6% vs. 7.0%, HR, 0.59; 95% CI, 0.38–0.92; p=0.021; Table 3, Fig. 3).
Table 3
Unadjusted and propensity-adjusted clinical outcomes at 12 months

Values are number (%) or median (interquartile range).
CABG, coronary artery bypass graft; CI, confidence interval; HR, hazard ratio; MI, myocardial infarction; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction; TLR, target-lesion revascularization; TVR, target-vessel revascularization.
![]()
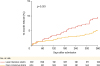 | Fig. 3Cumulative MACCE at 12 months with adjustment using propensity score matching.MACCE; major adverse cardiac and cerebrovascular event.
|
Subgroup analysis in the propensity-matched cohort showed consistent treatment effects of more intensive vs. less intensive statin therapy for 12-month MACCE across all subgroups (Fig. 4). The beneficial treatment effects of more intensive statins were more pronounced in the subgroup of patients with higher baseline hs-CRP (>3 mg/L) than in patients with lower baseline hs-CRP (≤3 mg/L; p for interaction=0.03; Fig. 4).
 | Fig. 4Subgroup analysis for MACCE at 12 months in the propensity-matched cohort.CI, confidence interval; hs-CRP, high-sensitivity C-reactive protein; eGFR, estimated glomerular filtration rate; HR, hazard ratio; LVEF, left ventricular ejection fraction; MACCE, major adverse cardiac and cerebrovascular event; MI, myocardial infarction; GRACE, Global Registry of Acute Coronary Event.
|
DISCUSSION
Results from the present study demonstrated that more intensive statin therapy was associated with significantly lower major adverse cardiovascular events in patients with acute MI and baseline LDL cholesterol <70 mg/dL compared with less intensive statin treatment. Patients receiving more intensive statins showed lower target-vessel revascularization and MACCE at 12 months without increased risk of hemorrhagic stroke or major bleeding. To the best of our knowledge, this is the first study in which the effectiveness of higher-intensity statins compared with lower-intensity statins was explored in ACS patients with very low LDL cholesterol at presentation. The results from the study suggest that more intensive statin treatment after ACS would be beneficial even for East Asians, known to have heightened response to statins and very low baseline LDL cholesterol level.
Data from randomized trials show that statin therapy in patients with ACS reduces the risk of cardiac mortality, recurrent MI, stroke, and coronary revascularization.12 Higher-risk patients benefited more from high-intensity statin therapy, as shown in the Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis In Myocardial Infarction 22 (PROVE IT-TIMI 22)1 and Myocardial Ischemia Reduction With Acute Cholesterol Lowering (MIRACL) trials,2 than from moderate- or low-intensity statin therapy. Nevertheless, high-intensity statin therapy has not been extensively utilized in East Asians,181920 possibly due to the lack of randomized trials in this population and a concern for the safety and tolerability of high-intensity statins because Asian patients frequently have heightened response to therapeutic drugs.21 In retrospective studies involving Korean patients with acute MI, the majority of patients received low-to-moderate intensity statins, and clinical outcomes were similar at 12 months between patients receiving high-intensity statins and low-to-moderate intensity statins.1920 However, in the recent Randomized Evaluation of Aggressive or Moderate Lipid Lowering Therapy With Pitavastatin in Coronary Artery Disease (REAL-CAD) study of Japanese patients with stable coronary artery disease, high-dose pitavastatin significantly reduced the risk of cardiovascular death, nonfatal MI, nonfatal ischemic stroke, and unstable angina compared with low-dose pitavastatin, without difference in the risk of adverse side effects,22 confirming the benefit of higher intensity statins for reducing cardiovascular events in high-risk East Asian patients.
Currently, initiating high-intensity statin therapy early after admission is recommended for all patients with ACS, the treatment goal being LDL cholesterol <70 mg/dL or at least 50% reduction of LDL cholesterol if the baseline level is between 70 and 135 mg/dL.3 However, for patients with very low baseline LDL cholesterol level, the safety and effectiveness of intensive statin therapy are not well established. The statin efficacy in ACS patients with very low LDL cholesterol has been evaluated in only a few observational studies.4523 Lee et al.4 and Piao et al.5 investigated the clinical outcomes of statin therapy in patients with acute MI whose baseline LDL cholesterol level was <70 mg/dL and ≤50 mg/dL, respectively, and found that statin therapy was associated with significant reduction in major adverse cardiac events at 12 months (14.5% vs. 20.4%, p=0.014 and 11.8% vs. 19.3%, p=0.025, respectively). Tsai et al.23 evaluated the effects of statin therapy in patients with ACS whose LDL cholesterol level was ≤80 mg/dL. The incidence of death, reinfarction, or stroke at six months was significantly lower with statin therapy (29.0% vs. 9.5%, p=0.005). The results from these studies consistently demonstrated that statin therapy resulted in more favorable clinical outcomes in ACS patients with lower LDL cholesterol level compared with those receiving no statin treatment, suggesting that patients with very low LDL cholesterol would still benefit from statin treatment post-ACS.
However, studies comparing the intensity of statins in ACS patients with very low LDL cholesterol at presentation are currently not available, although evidence indicates the safety and efficacy of very low LDL cholesterol in high-risk patients.24 In this regard, the results from the present study showed that dose-dependent efficacy of statins after ACS, even in patients with baseline LDL cholesterol <70 mg/dL, has important clinical implications, providing evidence in favor of more intensive statin therapy for this patient population. Concerns have been raised over the potential association between very low LDL cholesterol level and increased risk of hemorrhagic stroke, partially offsetting the overall benefit of high-intensity statin therapy.25 However, data from the randomized Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT)26 and Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER)27 trials showed that patients achieving extremely low LDL cholesterol level with intensive lipid lowering had no increase in hemorrhagic stroke. Consistent with findings from these trials, more intensive statin therapy did not increase the risk of hemorrhagic stroke in ACS patients with very low LDL cholesterol in the present study.
Despite the unequivocal benefits of statin therapy in reducing cardiovascular events, statins are underutilized in high-risk patients, especially those with lower LDL cholesterol level.28 In addition, most patients in clinical practice do not achieve an LDL cholesterol goal of <70 mg/dL, even when on high-intensity statins,29 warranting further LDL cholesterol lowering with addition of either ezetimibe or a PCSK9 inhibitor based on the results of IMPROVE-IT26 and FOURIER27 trials. Similarly, the present study results indicate the challenge of further reduction of LDL cholesterol with statin therapy alone in patients with very low LDL cholesterol at presentation. Several explanations are plausible for these findings, including an insufficient duration of follow-up, or that many higher-risk patients, as indicated by higher GRACE score, received less intensive statin therapy in the overall population. This demonstrates the difficulty of more significant risk reduction as well as LDL cholesterol lowering with more intensive statin therapy, although an adjustment was made using propensity score analysis. In addition, the treating physician might not have been aggressive in further reducing LDL cholesterol by increasing statin intensity in higher risk patients with very low LDL cholesterol due to safety concerns and insufficient clinical data in this patient subset, leading to higher risk patients more often receiving less intensive statins. Despite the less pronounced LDL cholesterol reduction, the clinical benefit conferred by more intensive statin therapy in the present study may involve mechanisms other than LDL cholesterol lowering, referred to as pleiotropic effects, which include attenuation of vascular inflammation, improved endothelial cell function, stabilization of atherosclerotic plaques, and inhibition of thrombogenic response.30
The present study had several limitations. First, although these results were derived from a large cohort, and adjustment was made using propensity score analysis for confounding variables, unmeasured factors may still exist. Higher-risk patients more often received less intensive statin therapy in the overall population. Although this discrepancy was not observed after propensity matching, the potential role of unmeasured residual confounding factors cannot be ruled out. Second, specific information regarding adherence or intolerance to statin therapy and why specific patients switched between more intensive statins and less intensive statins during follow-up were not available from the registry database. Third, the number of patients in each group who underwent follow-up measurements of LDL cholesterol and hs-CRP at 12 months was relatively small.
In conclusion, the results from this large, real-world study with propensity score analysis showed that more intensive statin treatment for patients with acute MI and very low LDL cholesterol significantly reduced major adverse cardiovascular events at 12 months compared with less intensive statin therapy. The results from this study support that more intensive statin treatment after ACS would be beneficial even for East Asians, known to have heightened response to statins.
 XML Download
XML Download