

 PDF
PDF ePub
ePub Citation
Citation Print
Print



BACKGROUND
Aspirin has been used for decades to prevent and treat cardiovascular disease (CVD). In the 20th century, CVD became a major cause of mortality and morbidity worldwide, and there have been numerous efforts to prevent it.123 Many strategies were proposed for CVD prevention, including lifestyle modification and strict management of major cardiovascular risks such as hypertension, diabetes, hyperlipidemia, and metabolic syndrome. Not only traditional methods but easier methods, such as taking pills, have been studied, and among these, aspirin was believed to have a beneficial effect in the primary prevention of CVD despite some controversy.45 Today aspirin is widely used and in the United States, in particular, 40% of adults over 50 are taking aspirin to prevent CVD.67
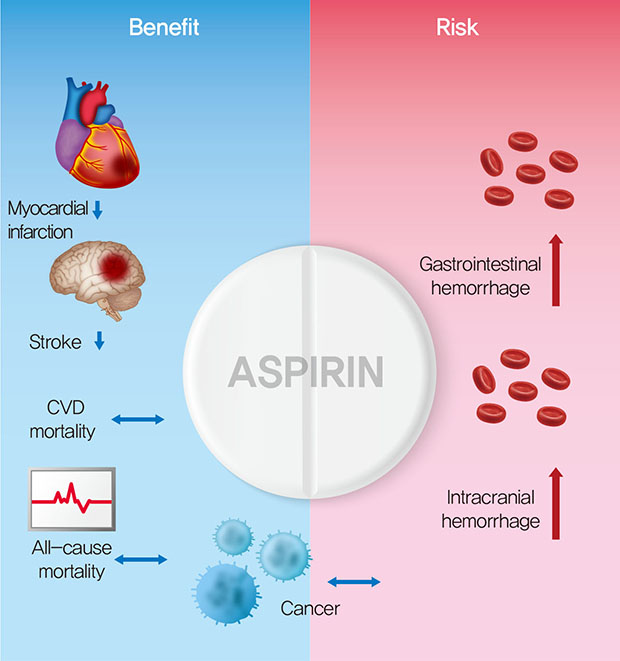
Aspirin is an irreversible and nonselective cyclo-oxygenase (COX) inhibitor, which reduces thromboxane A2 production, thus inhibiting platelet aggregation and vasoconstriction. This antiplatelet mechanism provides the potential to reduce arterial thrombosis and prevents myocardial infarction (MI) and stroke when used at a low dose.8 However, aspirin also reduces the production of prostaglandin, which protects gastrointestinal (GI) mucosa by inhibiting COX-1, resulting in the major side effect of GI bleeding.9
Several randomized clinical trials have assessed the effects of aspirin in CVD prevention. The efficacy of aspirin in the secondary prevention of CVD in high-risk patients with previous MI or ischemic stroke has been demonstrated many times through clinical trials.51011 For instance, the result of a meta-analysis by the Antithrombotic Trialists' (ATT) Collaboration group showed that the use of aspirin in secondary prevention was associated with an absolute reduction in severe vascular events (6.7% vs. 8.2%, p<0.0001).5 Currently, many guidelines recommend the use of low dose aspirin for secondary prevention in patients with documented CVD.121314
However, despite 30 years of randomized clinical trials, the effect of aspirin on the primary prevention of CVD in those who have not yet experienced cardiovascular events is still debatable. In 1988, the British Doctors Trial assessed whether aspirin could prevent MI in randomized healthy male physicians and reported a nonsignificant 3% reduction in the proportion of nonfatal MIs.15 Although this study did not produce any significant results, some studies conducted later for evaluating whether aspirin was suitable for CVD primary prevention showed a significant reduction in the risk of CVD.1617 Despite the controversial results about the role of aspirin for primary prevention, it is believed that aspirin has a beneficial effect, especially in the general population. This belief has encouraged the widespread use of aspirin for primary prevention. However, there is doubt about whether this wide use of aspirin is really appropriate, and the recently published results of several large clinical trials have added strength to this doubt. Here we will discuss whether the use of aspirin for primary prevention is correct in the current era based on the results from past and recent clinical trials.
CURRENT CLINICAL GUIDELINES
There are several clinical guidelines from various international organizations on the use of aspirin for primary prevention of CVD, and they offer some conflicting recommendations. The US Prevention Services Task Force (USPSTF) published meta-analysis data in 2016 and found that aspirin reduced the risk of nonfatal MI by 22% in 11 primary prevention trials conducted from 1988 to 2014. Despite the significant reduction in nonfatal MI, the risk reduction for CVD mortality or all-cause mortality by aspirin was not significant.16 Based on these results, in 2016, the USPSTF recommended the use of low-dose aspirin for adults aged 50 to 59 years with a 10-year CVD risk ≥10%, not at increased risk of bleeding, a life expectancy of ≥10 years, and willing to take low-dose aspirin daily for ≥10 years. For adults aged 60 to 69 with a 10-year CVD risk ≥10%, aspirin administration depends on the individual's decision. For adults aged <50 years or ≥70 years, the current evidence is insufficient to recommend aspirin for primary prevention.12
In 2016, the American Diabetes Association (ADA) recommended the use of aspirin (75–162 mg/day) as a primary prevention for men and women over the age of 50 with diabetes and high risk of CVD (10-year risk >10%),18 but the new 2019 recommendation states that individual-specific medical discussions should be conducted to use aspirin even for men and women with a high risk of CVD.14 This seems to reflect a number of recent clinical trials dealing with the effect of aspirin in primary prevention.192021
In 2012, the European Society of Cardiology did not recommend aspirin as a primary prevention drug, judging that the harm from aspirin was greater than the benefit.22 In 2016, as in 2012, the recommendations also did not propose aspirin as a drug for the primary prevention of CVD.13
Guidelines for women can be found in the American Heart Association 2011 guidelines,23 which recommend the use of aspirin for primary prevention in women 65 years or older if blood pressure is controlled and the benefit outweighs the risk of GI bleeding. For women under the age of 65, using aspirin is not recommended to prevent MI but can be considered in some cases to prevent ischemic stroke.
CHANGE IN THE PARADIGM
Despite the controversy over the safety and efficacy of aspirin, low-dose aspirin has been widely used for the primary prevention of CVD. According to the study of National Health and Nutrition Examination survey data, 22.5% of patients without a diagnosed CVD were classified as high risk, and 40.9% of them were told to take aspirin by their physician. In addition, 26.0% of people at low risk were told to take aspirin regardless of their risk category.7 Recently, however, questions have been raised about the use of aspirin for primary prevention of CVD. In particular, there are concerns that GI bleeding and hemorrhagic stroke, side effects that can occur in adults using aspirin, are increased.242526 Whether the benefits of aspirin in the prevention of CVD outweigh the risks associated with side effects is at the heart of the debate.
One of the major reasons for the paradigm shift about aspirin use is a reduction in the overall incidence of CVD. According to European CVD statistics in 2017 published by the European Heart Network, CVD mortality and the age-standardized prevalence rate of CVD are now falling in most European countries.27 Furthermore, from 1975 through to 2015, death rates from CVD have fallen in US men and women.28 Globally, the age-standardized disability-adjusted life-years (DALY) rates (per 100,000) in 2005 to 2015 for CVD decreased from 6,231.9 to 5,179.7.29 The substantial reduction of CVD mortality and incidence is due to improved prevention therapies, which manage the main risk factors of CVD such as smoking, physical inactivity, dyslipidemia, and high blood pressure. In addition, the modification of overall lifestyles, such as weight loss or regular exercise, has become popular.3031 Especially, modern-day medication use, such as statins, new anticoagulation agents, and antihypertensives, have contributed to reducing the CVD risk for the entire population.28 The magnitude of the risk reduction by aspirin in CVD primary prevention depends on the degree of initial risk in the individuals.12 Several studies have shown that if a patient's risk of CVD increases (above 1% per year), the benefit of using aspirin as primary prevention is also increased.5 Therefore, the overall CVD risk reduction caused by another preventive strategy seems to reduce the primary prevention of aspirin for CVD compared to in the past. The fact that the cardiovascular event rates for all patients who participated in the recently published Aspirin to Reduce Risk of Initial Vascular Events (ARRIVE) trial was lower than expected also supports this hypothesis.20
In contrast to the recent decrease in the effectiveness of aspirin for the primary prevention of CVD, the bleeding risk associated with aspirin still exists.26 In many studies, it is well-known that the use of low-dose aspirin was associated with a significantly increased risk of major bleeding events.323334 It is questionable whether the use of aspirin for CVD primary prevention will have a significant effect when compared to the risk of aspirin in the current era. Recent trends have observed that the use of aspirin for primary prevention of CVD is decreasing in the United States.35 Therefore, it is necessary to consider whether it is appropriate to continue aspirin for the primary prevention of CVD in each patient.
OUTBREAKING RECENT CLINICAL TRIALS
Recently, the publication of a number of studies has raised doubts about the benefits of using aspirin as a primary prevention for patients with moderate cardiovascular risk. In the present review, we will focus on four large scale clinical trials published after 2014 (Table 1).192021363738 Three of the trials were published in 2018, A Study of Cardiovascular Events in Diabetes (ASCEND), Aspirin in Reducing Events in the Elderly (ASPREE), and ARRIVE, and 1 clinical trial that was published in 2014, the Japanese Primary Prevention Project (JPPP) trial conducted in an Asian population.
Table 1
Randomized clinical trials of aspirin for primary prevention

HR, hazard ratio; RR, relative risk; ARRIVE, Aspirin to Reduce Risk of Initial Vascular Events; ASCEND, A Study of Cardiovascular Events in Diabetes; ASPREE, Aspirin in Reducing Events in the Elderly; JPPP, Japanese Primary Prevention Project; CV, cardiovascular; MI, myocardial infarction; TIA, transient ischemic attack; CVD, cardiovascular disease; DM, diabetes mellitus; HTN, hypertension.
*Dyslipidemia, current smoking, HTN, family history of CVD; †Dyslipidemia, HTN, DM.
The ASCEND study examined the usefulness of aspirin for primary prevention in patients with diabetes and found that aspirin lowers the risk of CVD (nonfatal MI, nonfatal stroke or transient ischemic attack [TIA], or death from any vascular cause) by about 12% (relative risk [RR], 0.88; 95% confidence interval [CI], 0.79–0.97; p=0.01).19 The study assessed the effectiveness and safety of aspirin use by randomly assigning 14,480 patients with diabetes into 100 mg aspirin or placebo groups and following them for an average of 7.4 years. Bleeding has emerged as a problem in the safety assessment. All major bleeding in this study was 29% higher in the aspirin administration group (RR, 1.29; 95% CI, 1.09–1.52; p=0.003) and a high risk of bleeding was seen in patients with a high risk of vascular events. The populations in this study had high rates of statin use, antihypertensive medications, and anticoagulant use, which directly affects the balance of aspirin use benefits and risks but also reflects the current pattern of medications in patients with diabetes. Finally, they concluded that aspirin use prevented serious vascular events in patients who had diabetes and no previous CVD, but this absolute benefit was largely counterbalanced by a similar rate of bleeding hazard.
In the ASPREE trial, elderly patients aged 70 or older who did not have CVD, dementia or disability were randomized and given 100 mg aspirin or placebo at a median of 4.7 years of follow-up.213637 Unlike other studies which set the occurrence of CVD as the primary endpoint, ASPREE evaluated all causes of death, dementia, and persistent physical disability as primary endpoints. As a result, taking aspirin in healthy elderly subjects did not prolong disability-free survival and caused more serious bleeding than the placebo. The primary incidence of outcomes, including deaths due to all causes, dementia, and persistent physical disability, was 21.5 aspirin per 1,000 person-years in the treatment group and 21.2 in placebo groups per 1,000 person-years with no significant risk difference between the groups (hazard ratio [HR], 1.01; 95% CI, 0.92–1.11; p=0.79). Furthermore, unlike other studies, the ASPREE study analyzed the cause of death. Death from any cause was 12.7 per 1,000 person-years in the aspirin group and 11.1 per 1,000 person-years in the placebo group with a significantly increased risk in the aspirin group (HR, 1.14; 95% CI, 1.01–1.29). However, the incidence of CVD was 10.7 in the aspirin and 11.3 in the placebo groups per 1,000 person-years, which indicated there was no difference (HR, 0.95; 95% CI, 0.83–1.08) between groups. Cancer was the major contributor of mortality in the aspirin group, accounting for 1.6 excess deaths per 1,000 person-years and cancer-related death occurred in 3.1% of the participants in the aspirin group and in 2.3% of those in the placebo group (HR, 1.31; 95% CI, 1.10–1.56). The incidence of bleeding, similar to other studies, was 8.6 per 1,000 person-years for aspirin, which was 38% higher than for the placebo at 6.2 per 1,000 person-years (HR, 1.38; 95% CI, 1.18–1.62; p<0.001). They concluded that when aspirin was taken for the primary purpose of preventing CVD in healthy elderly subjects without CVD, there was no benefit, and the risk of bleeding was greater and the mortality rate was higher. Finally, aspirin is not worth prescribing as a preventive medicine for healthy elderly people. The interesting point of this study is that they included dementia as a primary and secondary outcome because there were some previous suggestions that aspirin can reduce vascular dementia or physical inactivity by decreasing cerebral events. However, there was no significant difference between dementia and physical inactivity between groups.
The ARRIVE trial randomized 12,545 patients of 55 years (men) or 60 years (women) and older individuals (mean age 63.9) who had an average cardiovascular risk to receive 100 mg aspirin or placebo for 60 months of follow-up.20 They excluded patients at high risk of bleeding and diabetes. The primary endpoint (MI, stroke, cardiovascular death, unstable angina or TIA) occurred in 4.29% of patients in the aspirin group versus 4.48% of patients in the placebo groups (HR, 0.96; 95% CI, 0.81–1.13; p=0.6038). The major side effect of aspirin, GI bleeding events (characterized as mild), occurred in 0.97% of patients in the aspirin group versus 0.46% of patients in the placebo group (HR, 2.11; 95% CI, 1.36–3.28; p=0.0007). One of the important things to notice in the ARRIVE trial is that the actual cardiovascular event rate was lower than the predicted cardiovascular rate. This means that the group involved in the ARRIVE trials managed the CVD risk factor better than in the previous trials. The ratio of 43% in ARRIVE participants that have taken statins also supports this assumption.
Unlike other trials, the JPPP assessed the safety and efficacy of low-dose aspirin in primary prevention of CVD in Japanese patients who were representative of the oriental elderly population.38 The study population was 14,658 patients aged 60 to 85 with atherosclerotic risk factors, including hypertension, dyslipidemia, and/or diabetes. The patients were randomized to receive 100 mg of enteric-coated aspirin once daily or no aspirin other than ongoing medications for atherosclerotic risk factors and the duration of follow-up was 5 years. The primary endpoints of cardiovascular death, MI, and stroke were similar between the groups (2.8% vs. 3.0%, HR, 0.94; 95% CI, 0.77–1.15, p=0.54). Nonfatal MI (0.3% vs. 0.6%, p=0.019) and TIA (0.26% vs. 0.49%, p=0.044) were lower in the aspirin group while extracranial hemorrhage (0.86% vs. 0.51%, HR, 1.85; 95% CI, 1.22–2.81, p=0.004) and GI side effects, which include GI bleeding, were significantly higher in the aspirin group. Even though the risk of nonfatal MI and TIA decreased, the results indicated that aspirin had no superiority in reducing CVD in elderly Japanese patients with increased risk of extracranial bleeding and GI bleeding complications, in concordance with the results from other studies, supporting the need for careful consideration of the routine use of aspirin.
CONSIDERING ASPIRIN FOR PRIMARY PREVENTION IN THE CURRENT ERA
Overall, when looking at recent clinical trial results and trends, the use of aspirin as a primary prevention is generally not recommended, and individual patient contextual counseling is required for decisions. The question to consider is whether a simple comparison of the risks and benefits of aspirin use is possible. The main outcomes of the previous trials were mortality or incidence of CVD, but discussed side effects were bleeding, mainly GI bleeding, and some intracranial hemorrhage. However, these outcomes do not have the same effect on long-term health, and it is difficult to suggest that these outcomes have a 1:1 relevance in individual patients.39 Thus, in the context of primary prevention, an assessment of the balance between the benefits and risks of aspirin use is complex because it is difficult to compare the severity of vascular and bleeding events.
Patient-specific bleeding risk calculations are an important point in the use of aspirin for primary prevention. However, there are not yet adequate validation tools to assess the risk of bleeding associated with the use of aspirin in primary prevention.2632 A risk prediction tool for upper GI complications exists but does not predict overall major bleeding risk, and it cannot be adequately applied to a population for primary prevention.40 Therefore, further study for the assessment of bleeding risk is needed, and a reasonable decision is required to consider patient-specific history (e.g., history of GI ulcers, current bleeding) and several bleeding risk factors at present. In addition, several drugs that may reduce the bleeding risk of aspirin use need to be considered. In the bleeding of aspirin-treated patients, approximately half were GI bleeding, about a third of which were from upper GI tracts.41 It is possible that the occurrence of upper GI bleeding may be reduced by the continuous use of proton pump inhibitors (PPIs). Several studies have shown that the concomitant use of PPIs can reduce GI bleeding risk among aspirin users.253242
Another important factor for consideration in aspirin use is the effect of aspirin on the prevention of colorectal cancer. Several studies have shown that the use of aspirin reduces the incidence of colorectal cancer. Unlike the recommendation by the FDA on the use aspirin, the USPSTF recommendation for adults aged 50 to 59 was that aspirin not only works in the prevention of CVD prevention but also in the prevention of CRC.12 The result of recent clinical trials generally show no protective effect of aspirin in colorectal cancer, however, there are problems relating to the duration of the studies. If it is considered that the generally acceptable periods for cancer prevention are at least 10 or more years, overall, studies published recently have been relatively too short for the evaluation of cancer prevention and all of them leave questions about this problem.192021363738 A longer period of study will be needed to form an accurate conclusion.
In addition, it is necessary to consider that aspirin can give additive prevention or increase the risk of complications with medications that have been developed later and are already known to be effective with/without fewer complications such as statins, antihypertensive drugs, anticoagulation agents, or other antiplatelet agents. Recently, there have been many attempts to increase the efficacy of treatment by combining aspirin and other drugs.39 Studies in a Korean population compared whether dual antiplatelet therapy with aspirin or clopidogrel are more effective in preventing CVD than aspirin monotherapy, and the results showed that dual antiplatelet therapy is more beneficial.434445 Therefore, before deciding to use aspirin for primary prevention, efforts should first be made to find and manage modifiable risk factors and then the additional benefits should be later considered for individual patients.
ASPIRIN FOR PRIMARY PREVENTION IN VERY HIGH-RISK PATIENTS
As mentioned above, the magnitude of reducing the risk of CVD in primary prevention by aspirin depends on the degree of risk in the individual. In the ASCEND trial, aspirin decreased events of CVD in patients with diabetes but with the increased risk of bleeding. This result suggests that aspirin could have some role in patients with higher risk. Because of the lack of data and limited results, it is hard to define which patients are at a very high risk and have a net clinical benefit with aspirin in the current era, further studies with patients at very high risk will be needed.
A cardiovascular risk assessment will eventually become an important issue in deciding whether or not to use aspirin. In many studies, a global risk score is used to calculate CVD risk, which is based on the 2013 American College of Cardiology (ACC) and the AHA guidelines. This risk score estimates the 10-year risk of ASCVD, which includes MI, ischemic stroke, and ASCVD death.46 Based on these risk scores, the 2016 USPSTF guideline recommends a 10 year-ASCVD risk of 10% as a high-risk threshold when considering the use of aspirin for CVD primary prevention.12 However, it should be considered that the actual observed CVD rates in recent clinical trials are lower than the estimated CVD rates, these risk equations for high-risk thresholds are thought to be open to modification based on the recent population or epidemiologic data.
An additional factor in assessing the risks and benefits of using aspirin when applying a global risk score to a specific patient is the possibility of race dependent differences. It should be noted that the characteristics of Asian patients may differ from Western patients. Compared with Western patients, Asian patients show differences at various points such as past history of risk, treatment strategies, and drug responses.4748 In addition, Asian patients have a relatively low prevalence rate of obesity and dyslipidemia compared to Western patients.474950 Most risk calculation methods that are currently available are from the data of Western populations, and it is difficult to conclude that simply applying these risk scores to Asian populations is possible. Therefore, those with a very high risk of CVD should optionally be recommended to take aspirin by considering evidence, bleeding risks, and individual patient characteristics.
CONCLUSION
Recent clinical results show that low dose aspirin in patients with low CVD risk had no significant effect when used for the primary prevention of CVD, because of the high risk of bleeding side effects. These results appear to be due to the overall reduction in CVD risk with the development of modern CVD prevention therapies. Therefore, there is no evidence to recommend that the public take aspirin for the primary prevention of CVD, and especially for the patients who have only low to moderate risk. The assessment of the balance between the benefits and risks of aspirin use should take into account the risk of bleeding, patient preferences, costs, and patient status, and the use of aspirin should be determined on the basis of a thoughtful discussion between the physician and the patient.
 XML Download
XML Download