

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Invasive ductal carcinoma accounts for approximately 70%–80% of all invasive breast cancers. Squamous cell carcinoma of the breast is a very rare type, accounting for approximately 0.1% of breast cancer cases [1]. Herein, we present a case of invasive ductal carcinoma that recurred as squamous cell carcinoma of the breast. The patient had previously been diagnosed with the human epidermal growth factor receptor 2 (HER2) subtype of invasive ductal carcinoma, which relapsed as basal-HER2-subtype squamous cell carcinoma after 6 years. Squamous cell carcinoma of the breast tends to grow rapidly and is resistant to chemotherapy [2]. It is also associated with frequent development of cystic lesions [3], showing aggressive progression compared with that in other types of breast cancer [4]. Metaplastic breast cancer is related to the basal-like subtype [5]; among these, the basal-HER2 subtype is particularly rare. This report describes a case of relapsed basal-HER2 subtype of metaplastic squamous cell carcinoma of the breast.
CASE REPORT
A 49-year-old female patient presented with left periductal mastitis with nipple retraction in April 2018. Her chief complaint was left breast swelling with a febrile sensation. The patient had a previous history of invasive ductal carcinoma of the left breast in May 2012, which was managed with breast-conserving surgery and sentinel lymph node biopsy. The breast carcinoma was estrogen (prediluted, SP1; Ventana Medical Systems, Inc., Tucson, USA) and progesterone (prediluted, 1E2; Ventana Medical Systems, Inc.) receptor-negative, and the HER2 (prediluted, 4B5; Ventana Medical Systems, Inc.) score was 3+. The histopathologic result in the first surgery indicated HER2-subtype invasive ductal carcinoma. The tumor cells invaded the stroma in the form of linear strands or cords of various sizes. The nuclei of the neoplastic cells moderately varied in size; they had limited tubule formation capacity and a moderate mitotic count. HER2 immunohistochemistry showed 3+ immunoreactivity within the circumferential membrane of the tumor cells (Figure 1A and B). The basal markers cytokeratin (CK) 5/6 and epidermal growth factor receptor (EGFR) tested negative. Following the diagnosis of the relapsed mass in 2018, the basal markers that were investigated in the recurrent mass were re-examined in the first surgical specimen. Even after repeated immunostaining for CK 5/6 (1:100; B5/16 B4; DAKO, Kyoto, Japan) and EGFR (1:50; SP84; Cell Marque, Rocklin, USA), negative results were obtained (Figure 1C and D). The tumor–node–metastasis stage was stage IIA, T1cN1M0. After the first surgery, she received 4 cycles of doxorubicin and cyclophosphamide treatment, followed by 4 cycles of docetaxel. After 6 months of chemotherapy, radiation therapy was also completed, and 18 cycles of trastuzumab treatment were administered for 1 year. Thereafter, she was regularly followed up for the next 4 years. However, she skipped the scheduled examination in November 2017. After that, she visited the clinic with left periductal mastitis in April 2018. Breast ultrasound was performed, revealing a complex solid and cystic mass (approximately 3.5 × 1.9 cm) in the left upper central breast. The skin overlying her left breast showed diffuse thickening (Figure 2A and B). The cystic lesion was aspirated, and the aspiration fluid was turbid and yellowish. The aspiration fluid was cultured, and no bacteria were found. She was treated on the basis of suspected mastitis due to the abscess in the left breast. In May 2018, the abscess was incised, drained, and cultured again; however, no cultured bacteria were found (Figure 2C). After the initial incision and drainage, the tumor had enlarged. The size of the complex mass increased to approximately 5.5 × 3.8 cm (Figure 2D and E). A core-needle biopsy of the left breast lesion revealed squamous cell carcinoma. She opted to undergo left breast mastectomy, and as a preoperative evaluation, breast magnetic resonance imaging was performed, which showed a left breast mass abutting the pectoralis muscle with enlarged right axillary lymph nodes (Figure 3A). Positron emission tomography-computed tomography was performed to evaluate other metastatic lesions. Except for that in the right axillary lymph nodes, metastasis was not detected. In July 2018, her second surgery was performed because of relapsed left breast cancer. She underwent a left simple mastectomy and right axillary lymph node biopsy (Figure 3B and C). The histopathological result of the second surgery was metaplastic squamous cell carcinoma of basal-HER2 subtype. The course of treatment was decided by a multidisciplinary team, with inputs from various experts in the departments of surgery, oncology, pathology, and radiology. Her invasive ductal carcinoma had been locally controlled since 2012. Therefore, the best course of action was decided to be the repeated anthracycline and taxane chemotherapy, followed by trastuzumab, postmastectomy radiation therapy, tamoxifen, and goserelin.
Figure 1
Microscopic findings of the surgical specimen in May 2012. (A) High-grade invasive ductal carcinoma during the first surgery in May 2012 (×200, hematoxylin and eosin stain). (B) Human epidermal growth factor receptor 2 positivity of the invasive ductal carcinoma during the first surgery in May 2012 (×200, immunohistochemistry). (C) Cytokeratin 5/6 was not expressed in all tumor cells of the invasive ductal carcinoma. (D) Epidermal growth factor receptor was also not expressed in the invasive ductal carcinoma.
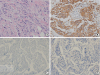
Figure 2
Ultrasound images and gross pictures of the left breast in 2018. (A) An approximately 3.5 × 1.9-cm, complex, solid, and cystic mass was detected in April 2018. (B) The presence of minimal peripheral vascularity was noted on Doppler ultrasound in April 2018. (C) Incision and drainage of the left breast mass was performed in May 2018. (D) An increased suspicious complex echoic mass was observed in July 2018. The enlarged mass in the left upper center breast was shown on breast ultrasound. (E) Increased vascularity was noted on Doppler ultrasound in July 2018. (F) The enlarged mass in the left breast was noted in July 2018, which was rapidly growing with whole-breast edema and nipple invasion.

Figure 3
MRI and specimen sections of squamous cell carcinoma of the left breast in July 2018. (A) Preoperative magnetic resonance imaging in July 2018 showed malignancy in the left upper center breast with direct invasion of the nipple–areolar complex and skin. Multiple enlarged lymph nodes in the right axilla were shown, and these lymph nodes were confirmed to be nonmalignant. (B) and (C) Postoperative specimen sections were evaluated after the second surgery in July 2018. On multiple sectioning, the cut surface showed an ill-defined, grayish-white mass with firm consistency (7.2 × 4.0 × 3.5 cm), which was very close to the nipple, areola, and deep margin.

The tumor was completely resected after the surgical treatment. Left axillary lymph node dissection was not performed because no enlarged or suspected malignant lymph nodes were detected during the second surgery. A frozen biopsy of the right axillary lymph nodes yielded negative results for malignancy. Therefore, right axillary lymph node dissection was not performed. No recurrence was observed, and chemotherapy is currently ongoing. The relapsed cancer in 2018 was pure squamous cell carcinoma and showed positive results for the breast cancer marker GATA binding protein 3. This recurring mass consisted of large polygonal malignant cells containing intercellular bridges and abundant eosinophilic cytoplasm with nuclear atypia and focal pycnotic keratinization found in squamous cell carcinoma (Figure 4A). The immunophenotype of this recurred mass was determined to be the basal-HER2 subtype. The Allred scores for estrogen and progesterone receptors were 2 and 6, respectively, and the HER2 score was 3+. The recurrent tumor cells showed strong expression of CK 5/6 in their cytoplasm and cell membrane and diffuse moderate membranous staining of EGFR (Figure 4B-D).
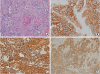
Figure 4
Microscopic findings of the surgical specimen in July 2018. (A) Pure squamous cell carcinoma was noted during the second surgery in July 2018 (×200, hematoxylin and eosin stain). (B) HER2 tested positive in the squamous cell carcinoma during the second surgery in July 2018. HER2 IHC showed 3+ immunoreactivities within the circumferential membrane of the tumor cells (×200, IHC). (C) Cytokeratin 5/6 showed strong expression in the recurred cancer (×200, IHC). (D) Epidermal growth factor receptor demonstrated diffuse moderate membranous staining (×200, IHC).
HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry.
DISCUSSION
We encountered a case of HER2-subtype invasive ductal carcinoma that recurred as basal-HER2-subtype squamous cell carcinoma of the breast. The tumor cells in the specimen from the first surgery did not show any expression of basal markers despite repeated staining. Phenotypes of invasive ductal carcinoma are not commonly completely changed to squamous cell carcinoma of the breast, especially the basal-HER2 subtype. Squamous cell carcinoma of the breast is a type of metaplastic carcinoma. Most metaplastic breast cancers (approximately 95%) are basal-like subtypes, according to previous microarray data [5]. Overexpression of the HER2/neu gene was reported in only 6% of cases of squamous cell carcinoma of the breast [6], which included both pure HER2 and basal-HER2 subtypes. According to a case report published in 2014, 3 cases of basal-HER2-subtype squamous cell carcinoma of the breast were reported among all 25,232 cases of invasive breast cancer during a 5-year period [7]. These were not cases of relapsed breast cancer, but were primary cases. According to another case report, invasive ductal carcinoma of the triple-negative subtype and adenocarcinoma recurred in a patient as squamous cell carcinoma of the breast [8]. Most previously published papers are about primary squamous cell carcinoma of the breast, apart from these aforementioned case reports. No recurrence data of basal-HER2-subtype breast cancer exist. Herein, we report a case of squamous cell carcinoma of the breast of basal-HER2 subtype at the previous site of invasive ductal carcinoma.
Both the basal-HER2 molecular subtype and squamous cell carcinoma of histopathologic subtype of the breast are characterized by poor prognosis. The basal-HER2 subtype is found in 9% of HER2-overexpressing tumors in invasive cancer [9]. The basal-HER2 subtype is characterized by poorly differentiated invasive ductal cancers or squamous cell carcinoma of the breast with a high level of p53 expression [10]. The basal-HER2 subtype confers poor disease-free survival compared to that conferred by other subtypes [11]. The 5-year overall survival rate of patients harboring the basal-HER2 subtype is reported to be 65%, whereas that of patients harboring the HER2 subtype is 96% [9]. The 5-year overall survival rate for the histopathologic subtype of squamous cell carcinoma of the breast has been shown to be 67.2% in previous studies [4]. However, no large-scale data showed the 5-year survival in those with basal-HER2-subtype squamous cell carcinoma of the breast, given its rarity. Its poor prognosis may also be partly because of its clinical resemblance to mastitis. Indeed, this case mimicked an inflammatory condition. Pure squamous cell carcinoma of the breast frequently results in large cystic changes with a necrotic background [3]. Therefore, malignancy is overlooked because of an abscess or pus-like lesion, leading to delayed diagnosis. Squamous cell carcinoma of the breast is also characterized by rapid growth. In the present case, the tumor rapidly grew enough to be visible within the 2-month period. For complex masses including both solid and cystic parts, as that in this case, the status of malignancy should be confirmed via core needle biopsy.
In this case, the nature of the breast tumor had changed despite the recurrence of cancer at the same site. Changes in the nature of the recurring tumor may be due to 2 reasons: radiation therapy that changes the microenvironment, including the surrounding immune cells of the tumor [12], and chemotherapies that also help modify the tumor characteristics into something different from the original tumor characteristics [13]. Breast cancer comprises a group of heterogeneous cells that are sensitive to treatment, which are dead and replaced by cells that are resistant to treatment. This process changes the tumor characteristics that adapt to the treatment and exhibit resistance to therapy. In this case, since the cancer recurred after chemotherapy and radiation therapy, only the cancer cells resistant to the previous treatment survived, resulting in new cellular characteristics.
In conclusion, HER2-subtype invasive ductal carcinoma can recur as basal-HER2-subtype squamous cell carcinoma of the breast with poor prognosis. The nature of the tumor in this case may have been changed due to the patient's treatment history. The possibility of cancer recurrence should be considered for cystic lesions occurring at the site of a previous breast cancer lesion.
 XML Download
XML Download