

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the development of silicone breast implants in 1960s, reconstruction techniques after breast cancer surgery have evolved considerably with the development of novel devices and surgical advancements. Owing to the relative simplicity of the procedure, reduced donor-site morbidity and operation time, and quicker postoperative recovery, immediate reconstruction with adjustable tissue expander insertion (TEI) after total mastectomy and delayed definitive reconstruction with a permanent implant are important emerging techniques [12].
Several studies advocate early shoulder mobilization after total mastectomy without reconstruction [345]. Furthermore, clinicians usually allow shoulder mobilization within 1 week after breast cancer surgery without reconstruction in actual practice.
To prevent surgical site complications such as prosthesis failure, surgical site infection, reoperation, hematoma, and capsular contraction [67], many plastic surgeons use the so-called “conventional protocol,” which immobilizes the shoulder and upper arm for 1 month after reconstruction. However, long-term immobilization of the shoulder joint leads to shoulder dysfunction after reconstruction, resulting in reduced quality of life [8]. Early shoulder mobilization has been shown to aid in the prevention of shoulder dysfunction after total mastectomy without reconstruction, and no additional surgical site or implant complications have been reported [91011]. However, since immediate breast reconstruction with TEI is a novel surgical technique, there is a lack of evidence regarding early postoperative shoulder exercise.
In an effort to improve shoulder mobility and quality of life of patients undergoing immediate breast reconstruction with TEI, authors of the present study introduced an early rehabilitation protocol with a short-term immobilization period of 2 weeks. The primary objective of this study is to compare the early rehabilitation exercise program with the conventional protocol by evaluating shoulder mobility, pain, quality of life, and complications. Additionally, we analyze factors affecting shoulder mobility and quality of life of patients after immediate breast reconstruction.
METHODS
Subjects
After obtaining approval by our Institutional Review Board (IRB) of Samsung Medical Center, a retrospective chart review of prospectively collected data was conducted in patients who underwent breast reconstruction with TEI at a tertiary hospital between May 2016 and August 2017. Due to the retrospective study design and harmless nature of the study, the IRB approved a waiver of informed consent. The IRB number was SMC 2018-01-008-001. Patients who had pre-existing conditions that limited shoulder movements were excluded.
Procedures
From May 2016 to December 2016, patients with breast cancer who underwent immediate breast reconstructive surgery with TEI were referred to the cancer rehabilitation clinic for postoperative rehabilitation. A physiatrist evaluated the baseline characteristics of the patients at 1 week after surgery. According to the conventional protocol, patients were asked to immobilize the operation site shoulder for more than 4 weeks and to engage in a self-exercise program after the end of the immobilization period. The physiatrist and plastic surgeon evaluated shoulder mobility, pain, quality of life, and complications at postoperative 1 month (midpoint) and 2 months (endpoint). In patients diagnosed with secondary adhesive capsulitis at the postoperative 1-month (midpoint) evaluation, supervised shoulder physical therapy was performed. In other cases, self-administered exercise was continued.
Beginning in January 2017, the Department of Rehabilitation and Physical Medicine and the Department of Plastic Surgery developed an early rehabilitation exercise program for postoperative patients of immediate breast reconstruction with TEI. Patients were educated to undergo a self-exercise program after a short-term immobilization period of 2 weeks. Follow-up assessment was also performed at postoperative 1 month (midpoint) and 2 months (endpoint).
Then, we conducted a retrospective case-control study comparing the 2 groups: the conventional protocol group including patients enrolled between May 2016 and December 2016 and the early rehabilitation group comprising patients enrolled between January 2017 and August 2017 (Figure 1).

Surgical method
Immediately after skin-sparing total mastectomy by a general surgeon, a plastic surgeon inserted a tissue expander into the subpectoral plane and placed it under the fascia of the pectoralis major and serratus muscles.
Self-exercise program
During the immobilization periods, patients were advised not to lift their arms above shoulder height or to let their arm fall backward. All activities that pulled the arms toward the body were prohibited. After the immobilization period, patients were instructed to perform a self-exercise program to improve shoulder range of motion (ROM) and overcome disuse muscle atrophy. The self-exercise program consisted of 6 types of progressive shoulder-stretch exercises, including beach pose, chest stretch, and biceps curl with low weight. The exercise program was structured as a set of 5 to 10 repetitions, performed 4 times a day, 7 days per week (Figure 2).

Measurement
At postoperative 1 week (baseline), independent factors that could affect the outcomes of rehabilitation protocols were assessed, including the following demographic and clinical characteristics: shoulder ROM at postoperative 1 week, numeric rating scale (NRS) for pain at postoperative 1 week, short-form 36 health survey (SF-36) at postoperative 1 week, extent of lymph node dissection, and history of neoadjuvant chemotherapy.
At postoperative 1 month (midpoint) and 2 months (endpoint), the outcomes of rehabilitation protocols were evaluated. The shoulder ROM and surgical site complications were evaluated as primary outcomes. The disabilities of the arm, shoulder, and hand (DASH) score, NRS for pain, and SF-36 were evaluated as secondary outcomes.
Shoulder ROM
Passive shoulder ROM was measured for flexion, abduction, and external and internal rotation in the affected upper arm. Measurements were conducted by a physiatrist using a goniometer, with patients in a seated position. Flexion and abduction were measured while the examiner elevated the patient's arm in the sagittal and coronal planes of the trunk, respectively. Scapular rotation was permitted for flexion and abduction. Internal and external rotation were measured in a neutral position with the shoulder adducted, the elbow flexed at 90°, and the forearm in a neutral pronation-supination position. The angle between the long axis of the forearm and anteroposterior axis of the trunk was determined as rotational ROM [12]. Patients who showed progressive loss of glenohumeral motion in a capsular pattern (i.e., external rotational ROM restriction of > 30° and 1 or more additional directional restriction) with inflammatory shoulder pain were diagnosed as having secondary adhesive capsulitis [13].
Surgical site complication
A single plastic surgeon evaluated the surgical site for hematoma, seroma, surgical site infection, implant rupture, extrusion of the implant, displacement of the implant, and any other complications.
DASH outcome measure questionnaire
The DASH questionnaire is a 30-item questionnaire designed to assess physical function and symptoms in patients with musculoskeletal disorders of the upper limbs. Scores were transformed to a 0 to 100 scale. A higher score indicates greater upper extremity disability. The inter-rater and intra-rater reliabilities of the questionnaire were > 0.95 [14].
NRS for pain
In our study, we used the NRS for pain assessment, instead of the visual analog scale (VAS). Based on a review of pain assessment tools, NRS has greater sensitivity compared to the VAS and facilitates an easier assessment of pain severity [15]. Resting pain was measured while the patient was lying on the bed without moving the shoulder. Motion pain was measured at the time of maximal shoulder motion.
SF-36
The SF-36 was used to assess the quality of life of the study participants. The SF-36 contains 8 sections measuring 8 domains of quality of life, namely, physical functioning, role limitations because of physical health problems, bodily pain, general health perception, vitality, social functioning, role limitations because of emotional problems, and mental health. Scores of each section are calculated on a 0–100 scale, with a higher score indicating a positive result on each scale. The 8 sections are summarized into 2-component summary scores: physical and mental. The SF-36 exhibits satisfactory internal consistency and good validity among breast cancer survivors [16]. The Korean version of the SF-36 has been developed and validated previously [17].
Statistical analysis
To compare the outcomes (shoulder ROM, SF-36, DASH score, and NRS at postoperative 1 and 2 months) of the early rehabilitation exercise program with those of the conventional protocol, we used a linear mixed model, which enabled us to control the effects of variables such as age, extent of lymph node dissection, and history of neoadjuvant chemotherapy. The rehabilitation protocol and other parameters (age, extent of lymph node dissection, history of neoadjuvant chemotherapy) were registered as fixed effects, and the patient was registered as a random effect. We used Bonferroni correction as post hoc analysis.
Baseline characteristics of the 2 groups were compared using the χ2 test or Fisher's exact test for categorical information and the independent t-test or Mann-Whitney test for quantitative data, based on normality testing using the Shapiro-Wilk test. All analyses were conducted using SPSS version 19.0 (SPSS Inc., Armonk, USA). The p-values < 0.05 were considered statistically significant.
RESULTS
Baseline characteristics
We reviewed 115 patients who underwent total mastectomy and immediate breast reconstruction with TEI in this present study. Of the total patients, 66 received the conventional shoulder rehabilitation protocol from May 2016 to December 2016, and the remaining 49 received the early rehabilitation protocol from January 2017 to August 2017. Patients were encouraged to perform their exercises on a daily basis and were asked regarding compliance during the follow-up period. Demographic and baseline clinical characteristics of patients are shown in Tables 1 and 2. There were no statistically significant differences between the 2 groups in terms of demographic and baseline clinical characteristics.
Table 1
Demographic and clinical characteristics related to shoulder mobility and quality of life of patients undergoing immediate expander-implant breast construction (n = 115)
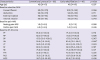
Values are presented as median (range).
ROM = range of motion; NRS = numeric rating scale; SF-36 = short-form 36 health survey; PF = physical functioning; RP = role limitations because of physical health problems; BP = bodily pain; GH = general health perception; VT = vitality; SF = social functioning; RE = role limitations because of emotional problems; MH = mental health; PCS = physical component summary; MCS = mental component summary.
The p-values obtained from the Mann-Whitney test or *independent t-test.
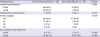
Table 2
Clinical characteristics related to breast cancer treatment of patients undergoing immediate expander-implant breast construction (n = 115)
Early rehabilitation versus the conventional protocol
Shoulder mobility and upper limb function
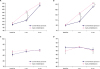
The shoulder flexion and abduction range at 1 month after surgery was greater in the early rehabilitation group than in the conventional protocol group (p < 0.001 for flexion, p < 0.001 for abduction). At postoperative 2 months, the significant difference in the shoulder abduction range between the 2 groups continued (p = 0.017), whereas that in the shoulder flexion range did not (p = 0.139) (Figure 3A and B). The shoulder internal and external rotation ranges showed no significant difference between the 2 groups during 2 months of follow-up (Figure 3C and D). There was no significant difference in the DASH score between the groups.
Figure 3
Shoulder range of motion: early rehabilitation versus conventional protocol
(A) Early rehabilitation and shoulder flexion ROM. Early rehabilitation group had greater shoulder flexion at postoperative 1 month than conventional protocol group. (B) Early rehabilitation and shoulder abduction ROM. Early rehabilitation group had greater shoulder abduction at postoperative 1 and 2 months than conventional protocol group. (C) Early rehabilitation and shoulder external rotation ROM. The ranges of shoulder external rotation showed no significant difference between conventional protocol and early rehabilitation during 2 months of follow-up. (D) Early rehabilitation and shoulder internal rotation ROM. The ranges of shoulder internal rotation showed no significant difference between conventional protocol and early rehabilitation during 2 months of follow-up.
ROM = range of motion.
*p < 0.05.
Complications
1) Surgical site complications
Only one patient in the early rehabilitation group had oozing at the operation site at 1 and 2 months after surgery. However, the surgical site oozing had been detected at the postoperative week 1. Therefore, the patient's surgical site complication cannot be attributed to the early rehabilitation protocol. Otherwise, there were no other surgical site issues during the 2 months of follow-up in either group.
2) Secondary adhesive capsulitis
At the 1-month follow-up evaluation, 4 patients in the conventional group were diagnosed with secondary adhesive capsulitis, in contrast to none in the early rehabilitation group. All patients received supervised physical therapy for 1 month. At the 2-month follow-up evaluation, 3 of the 4 patients diagnosed with secondary adhesive capsulitis showed full recovery of shoulder ROM, with one patient showing further decreased shoulder ROM after supervised physical therapy.
Other factors affecting shoulder mobility
Extent of lymph node dissection
The extent of lymph node dissection influenced shoulder flexion and abduction range at postoperative 1 week (p = 0.011 for flexion, p = 0.013 for abduction), 1 month (p < 0.001 for flexion, p < 0.001 for abduction) and 2 months (p = 0.003 for flexion, p = 0.004 for abduction). Overall, patients who underwent sentinel lymph node biopsy showed better shoulder flexion and abduction ROM than those who underwent axillary lymph node dissection throughout the follow-up period (Figure 4). However, the extent of lymph node dissection was not associated with shoulder internal or external rotation ROM or the pain NRS, SF-36, or DASH scores.
Figure 4
Shoulder range of motion: sentinel lymph node biopsy versus axillary lymph node dissection
(A) Extent of lymph node dissection and shoulder flexion ROM. The SLNB group showed better ROM in shoulder flexion than ALND group throughout 2 months of follow-up. (B) Extent of lymph node dissection and shoulder abduction ROM. The SLNB group showed better ROM in shoulder abduction than ALND group throughout 2 months of follow-up.
ROM = range of motion; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection.
*p < 0.05.

Other factors
During the 2-month follow-up period, age and neoadjuvant chemotherapy were not associated with shoulder ROM or quality of life. No patients in the conventional protocol group and one patient in the early rehabilitation group underwent postoperative radiotherapy; that patient underwent neoadjuvant chemotherapy and nipple-sparing mastectomy with axillary lymph node dissection and showed nearly full shoulder ROM at the 1-month follow-up. After radiotherapy to the chest wall and rib cage, the patient showed full shoulder ROM at the 2-month follow-up.
DISCUSSION
This study clearly demonstrates that after total mastectomy and immediate breast reconstruction with TEI, early rehabilitation with a shorter immobilization period of 2 weeks resulted in a significantly faster recovery of shoulder mobility without additional complications than the conventional protocol. It also demonstrates that the extent of lymph node dissection is a key factor in the recovery of shoulder mobility after surgery.
Several previous studies have addressed early rehabilitation after breast cancer surgery without reconstruction [34]. In a 2010 Cochrane review, McNeely et al. [5] reviewed 10 studies including 1,304 patients comparing early shoulder exercise (postoperative day 1–3) and delayed shoulder exercise (postoperative day 4–). The study reported that although early exercise results in a larger volume and longer duration of wound drainage compared to delayed exercise, early exercise more effectively facilitates the short-term recovery of shoulder ROM, without any significant difference in the incidence of seroma formation, delayed wound healing, wound aspirations, pain, or lymphedema. Accordingly, clinicians tend to prescribe shoulder mobilization within 1 week after breast cancer surgery without implant insertion.
Previously, total mastectomy without implant followed by delayed breast reconstruction was the most preferred surgical method; however, in recent years, the number of cases of concurrent TEI has increased. Despite the increasing number of patients receiving immediate breast reconstruction with TEI, no study has investigated postoperative rehabilitation after such surgery, to the best of our knowledge. Due to the lack of evidence, many plastic surgeons and physiatrists are hesitant to recommend early mobilization for patients undergoing breast reconstruction with TEI. Thus, the positive results of our study may encourage plastic surgeons and physiatrists to prescribe early postoperative shoulder mobilization in these patients.
Generally, adjuvant radiotherapy or chemotherapy is performed at 2 months postoperatively, which was the time period covered in this study. Radiation therapy for patients with breast cancer requires the proper positioning of the affected upper limb, i.e., greater than 120 degrees of ROM in shoulder forward flexion and abduction. Consequently, limited shoulder joint ROM at this critical stage may delay the initiation of radiation therapy, which may increase the risk of local recurrence. Each month of delay confers a 0.5% increase in the risk of local recurrence [18]. Therefore, the rapid recovery of shoulder ROM after breast cancer surgery, achieved by early rehabilitation, allows oncologists to maximize adjuvant therapy options.
In our study, irrespective of the protocol, the limitations of shoulder forward flexion and abduction were more severe than those of shoulder rotation, which is in line with the results of previous studies that addressed shoulder ROM after mastectomy without reconstruction [1920]. Patients with shoulder joint capsule defects, such as adhesive capsulitis, manifest more severe shoulder rotational problems than those of flexion or abduction. Hence, pathology of the glenohumeral joint is not the cause of shoulder dysfunction after mastectomy. During mastectomy, the fascia overlying the pectoralis major muscle is removed, and the subcutaneous tissue on the skin flaps adheres to the raw muscle. Adhesions between the pectoral muscles, subcutaneous tissue, and skin in the axillary and the pectoral areas may inhibit full extension of the pectoral muscle, causing limited flexion and abduction of the affected arm [21]. In reconstruction with TEI, the implant that is placed under the back of the pectoralis major muscle further inhibits the usual smooth sliding between the pectoralis major muscle and other surrounding structures.
In accordance with previous studies [2223], the extent of axillary lymph node dissection was significantly associated with shoulder mobility in our study. In axillary dissection, axillary fat between the axillary muscles and skin flaps is removed, and the skin flaps in the axillary area can adhere to the raw axillary muscles, causing deterioration of shoulder mobility.
There are several limitations in our study. First, this study was not conducted as a randomized trial and was performed in a single-center. However, the study population was large enough to validate this study (n = 115). In addition, there were no inter-rater differences in the surgical technique or postoperative evaluation because all patients enrolled in our study received immediate breast implantation surgery by the same plastic surgeon and were evaluated by the same physiatrist. Second, shoulder internal rotation is usually measured with the shoulder abducted 90°. However, in this study, shoulder internal rotation was measured in a neutral position with the shoulder adducted because patients had limited shoulder abduction due to postoperative shoulder pain. In this measurement method, the torso interferes with achieving the full range of internal rotation. Therefore, cautious interpretation of the internal rotation results is necessary. Third, components of the exercise program and degree of compliance may influence the effect of exercise. In this study, although we regularly educated patients during admission and at the 1- and 2-month follow-up visits regarding the importance of performing daily exercise, they were not required to record or report the strength, time, or frequency of the exercise. Thus, the objective components and quality of exercise were not properly evaluated and should, therefore, be considered in future home-based exercise studies. Finally, although no significant surgical site complications occurred during our follow-up period, long-term complications such as capsular contracture may still occur.
Despite these limitations, this is the first study to address rehabilitation after reconstruction with TEI. Therefore, our results represent an initial guideline for plastic surgeons and physiatrists. Further multi-institutional studies with a longer follow-up period are needed to validate our results.
In conclusion, early rehabilitation with a shorter immobilization period can be recommended for better shoulder mobility in patients with breast cancer undergoing immediate reconstruction with TEI. As recovery of shoulder ROM can be slow in these patients, particularly in those with axillary lymph node dissection, more intensive treatments may facilitate improved outcomes.
 XML Download
XML Download