

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Breast cancer is the most common cancer in women worldwide and the second most common malignancy in Korean women [12]. Breast-conserving surgery and adjuvant radiotherapy (RT) are increasingly performed in patients with breast cancer [23]. Accordingly, post-RT complications are of great interest for both physicians and patients. Late cardiac complications following adjuvant RT for the left breast have been widely investigated, and a linear association between heart dose and coronary heart disease was identified in a large population-based study [4].
The ipsilateral lung and heart are the normal organs of concern when planning for whole breast RT. However, other normal organs such as the stomach, liver, and colon are also frequently irradiated, depending on individual anatomy. The stomach is located directly below the left diaphragm and occasionally included in the tangential RT field in left breast cancer treatment. However, little is known about the effect of irradiation on the stomach following adjuvant RT for breast cancer. Although the stomach is considered relatively safe to irradiate, we hypothesized that several factors predisposing to gastric disease in the Korean population may enhance RT-related toxicities of the stomach.
This study aimed to evaluate late complications in the stomach following adjuvant RT for breast cancer using data from the Health Insurance Review and Assessment Service (HIRA) of South Korea.
Methods
Database and study population
The Institutional Review Board of Samsung Medical Center approved this study and informed consent was waived. (IRB No. 2017-06-019).
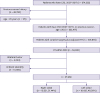
A nationwide cohort diagnosed with breast cancer (C50.* according to the International Classification of Disease Tenth Revision [ICD-10]) from 2007 to 2017 was extracted from the HIRA database. Figure 1 describes the process of selecting the study population. After excluding women who were already diagnosed with other cancers prior to breast cancer and those aged < 20 years, 225,477 women were identified. Among these, patients who underwent curative surgery for breast cancer followed by adjuvant RT were identified (n = 109,894). To secure ≥ 5 years of follow-up, the cohort who underwent RT in 2012 was selected and followed until 2017 for development of gastric complications. Right and left breast cancers were identified using breast cancer codes: right breast (C50.*0) and left breast (C50.*1). Cases with unknown tumor laterality and both right and left breast codes were excluded. Finally, a total of 37,966 patients were included in the analysis.
Gastric complications
Gastric complications were assessed by the identifying diagnosis of gastric cancer and hemorrhagic gastric disease from the date of RT until December 2017, and the incidences between right and left breast cancers were compared. The diagnosis of gastric cancer was defined as C16.* codes in the claim data, and the diagnosis of hemorrhagic gastric disease was defined as diagnostic codes of K25.0, K25.1, K25.2, K25.4, K25.5, K25.6, K26.0, K26.1, K26.2, K26.4, K26.5, K26.6, K27.0, K27.1, K27.2, K27.4, K27.5, K27.6, K28.0, K28.1, K28.2, K28.4, K28.5, K28.6, K29.0, K92.0, K92.1, and K92.2 in ICD-10 [5]. Supplementary Table 1 shows detailed information regarding claim codes for surgery and RT.
Statistical analysis
Distributions of categorical variables between right and left breast cancers were compared using the chi-square test. Time to disease was defined as the time between the last day of RT for breast cancer and the date of the first disease claim. To estimate the cumulative incidence of gastric disease and generate hazard plots, the Kaplan-Meier method was used. The cumulative incidence curves between groups were compared using log-rank test. Cox proportional-hazards model was used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) to control for other covariates. All statistical analysis was conducted using SAS software version 9.4 (SAS Institute, Cary, USA).
Results
Patient characteristics
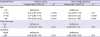
A total of 37,966 patients were included in the analysis. Of a total of 37,966 patients, 19,531 (51.4%) had right breast cancer, and 18,135 (48.6%) had left breast cancer. The most frequent age was 41–50 years (n = 15,765, 41.5%), which was followed by 51–60 years (n = 10,332, 27.2%), < 40 years (n = 6,617, 17.4%), and > 60 years (n = 5,252, 13.8%). Chemotherapy was performed in 62.3% of all patients. The distributions of chemotherapy are presented in Table 1.
Table 1
Characteristics of patients: right vs. left

![]()
Gastric cancer
After a median follow-up duration of 6.3 years (range, 0–10.5), 236 patients developed gastric cancer, and the 10-year cumulative incidence was 0.85% (Figure 2A). The cumulative incidence of gastric cancer did not differ between right and left breast cancers (0.81% vs. 0.89% at 10 years, p = 0.414). The incidence of gastric cancer at 10 years was 0.30%, 0.77%, 1.01%, and 1.53% in patients aged ≤ 40 years, 41–50 years, 51–60 years, and > 60 years, respectively (Figure 2B). From the mutually adjusted Cox proportional-hazards model that included the age group, chemotherapy, and tumor laterality, old age was the only significant factor for the development of gastric cancer (p < 0.001) (Table 2). The HRs (95% CI) for gastric cancer in patients aged 41–50 years, 51–60 years, and > 60 years compared to those aged ≤ 40 years were 2.23 (1.33–3.76), 2.77 (1.63–4.71), and 4.84 (2.82–8.33), respectively.
 | Figure 2Cumulative incidence of gastric cancer in (A) women with right and left breast cancers and (B) women aged ≤ 40, 41–50, 51–60, and > 60 years.HR = hazard ratio; CI = confidence interval.
|
Table 2
Adjusted cox regression models for gastric complications
![]()
Hemorrhagic gastric disease
After excluding 5,121 patients who had gastric disease before the diagnosis of breast cancer, 2,936 of 29,909 patients developed hemorrhagic gastric disease after RT, and the 5-year cumulative incidence rate of gastric hemorrhage was 2.5%. The cumulative incidence of hemorrhagic gastric disease was not different between right and left breast cancers (2.6% vs. 2.4% at 5 years, p = 0.166, Figure 3A). The 5-year incidence rates of hemorrhagic gastric disease were 2.16%, 2.37%, 2.51%, and 3.08% in patients aged ≤ 40 years, 41–50 years, 51–60 years, and > 60 years, respectively (Figure 3B). In the multivariable analysis, old age was the only significant factor (p < 0.001) (Table 2). The HRs (95% CI) for hemorrhagic gastric disease in patients aged 41–50 years, 51–60 years, and > 60 years compared to women aged ≤ 40 years were 1.14 (0.96–1.37), 1.28 (1.07–1.55), and 1.54 (1.25–1.89), respectively.

Discussion
This study demonstrated that the risk of late gastric complications following adjuvant RT was not different between patients with right and left breast cancers and age was the most important risk factor for the development of gastric complications. In the Korean insurance system, most patients with cancer complete the regular follow-up at 5 years and thereafter visit local hospitals because patient costs increase 5 years after initiating cancer treatment if there is no evidence of recurrence. Accordingly, most information on late complications that develop after 5 years might be lost if hospital data is used. To overcome this issue, we used the data of the National Health Insurance system of South Korea, which covers > 98% of the Korean population [6].
The stomach is a relatively radioresistant organ, and the estimated dose with 5% risk at 5 years (TD 5/5) for the whole stomach is reported to be 50 Gy [7]. The rate of gastric ulcer was 4% after a dose < 50 Gy vs. 16% after a dose ≥ 50 Gy in early studies [8]. Considering standard doses of adjuvant RT for breast cancer (50.4–54 Gy), the dose to the stomach would not be negligible if > 90% of the prescribed dose is irradiated to the stomach. Similar to radiation proctitis, RT-induced hemorrhagic gastric disease usually presents within 3 years of RT. It manifests as an edematous change in the mucosa and multiple telangiectasias in the irradiated area, resulting in hemorrhage [9]. RT-induced hemorrhagic gastric disease has been reported in a few case reports, most of which were from gastrointestinal malignancy cases [1011121314]. Das et al. [10] reported nine cases of gastric bleeding following RT for intrahepatic cholangiocarcinoma and suggested that the risk of RT-related gastric bleeding was most relevant to V40 and V50 of the stomach. Feng et al. [11] showed that RT-induced gastric bleeding is largely affected by concomitant liver cirrhosis and maximal stomach dose. A generalized equivalent uniform dose (gEUD) of 46 Gy is associated with a 20% bleeding risk in patients without cirrhosis, while a gEUD of only 18 Gy is associated with a 20% bleeding risk in patients with cirrhosis [11]. Other than cirrhosis, old age, concurrent chemotherapy, and Helicobacter pylori-induced gastritis were reported as risk factors that can lower the threshold dose of the stomach [15]. In the present study, age was the only significant risk factor for hemorrhagic gastric disease.
Korea has an epidemic of gastric cancer due to H. pylori infection and high consumption of spicy and salty food. In the Korean female population, the crude incidence rates of gastric cancer are 0.04%, 0.09%, and 0.17% for those aged 40–54 years, 55–69 years, and 70–79 years, respectively [16]. Surveillance, Epidemiology, and End Results data showed that the incidence rates of gastric cancer in patients with breast cancer were 0.14% and 0.08% in the surgery-alone and surgery plus RT groups, respectively [17]. Another Western study [18] reported that the incidence rates of stomach cancer were 0.22% and 0.16% in those who received and did not receive RT for breast cancer, respectively. A small Korean study reported that 0.6% of 2657 patients with breast cancer developed gastric cancer, which is similar with our result (0.62%) [19]. Another Korean study reported a much lower incidence rate of gastric cancer (0.29%) among breast cancer survivors [20]. The lower rates might be due to loss of diagnosis outside the hospital. The incidence rate of gastric cancer in Korean patients with breast cancer who received RT is higher than that of the general Korean population or patients with breast cancer in Western countries. However, the incidence did not differ between patients with right and left breast cancers.
This study has several limitations. First, a number of important confounding factors for gastric disease were not considered, such as H. pylori infection, smoking, and alcohol consumption. Unfortunately, HIRA data could not be linked to hospital or personal data. Second, the claim data contain some intentional or unintentional errors induced by reimbursement issues or physician priorities. Furthermore, it is difficult to identify the causal effect of RT on diseases through detailed information such as comparison between endoscopic finding and RT field, especially with hemorrhagic gastric disease. Nevertheless, we hypothesized that claim-related errors and other clinical factors such as H. pylori infection, smoking history, and medication use would be the same in right and left breast cancers, so we compared the two groups even with the possibility of these errors. Finally, there was no difference between right and left breast cancers in the development of hemorrhagic gastric disease or gastric cancer, indicating that RT does not further increase the risk of these diseases. However, crossed incidence curves of right and left breast cancers for gastric cancer development at 10 years suggest that a longer follow-up period might be needed because RT-related secondary malignancy usually develops in approximately 10 years.
Therefore, we did not find any increased risk of gastric cancer and hemorrhagic gastric disease in patients who received adjuvant RT for left breast cancer compared to those for right breast cancer in the 10-year follow-up. The RT-related chronic complications of the stomach in patients with breast cancer are minimal. A study with longer follow-up duration is needed to confirm the risk of gastric cancer in these patients.
 XML Download
XML Download