

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
To achieve a tumor-free margin and improve cosmetic outcome in patients with breast cancer who will undergo breast-conserving surgery (BCS), a preoperative assessment of surgical extent is essential. Although delineating the tumor border is a key step during preoperative evaluation, an optimal width of safety margin has long been debated. However, in 2014, joint panels from the Society for Surgical Oncology and the American Society for Radiation Oncology published consensus statements to guide the clinicians regarding the pathologic margin for BCS that is followed by whole-breast irradiation [1]. Based on a meta-analysis of margin width and ipsilateral breast tumor recurrence [2], the new guidelines recommend “no ink on tumor” as the standard for a negative margin. Thus, an accurate prediction of tumor extent with comprehensive breast imaging in addition to clinical examination has become more important.
The use of breast magnetic resonance imaging (MRI), in addition to standard assessment by mammography and ultrasonography (US), is increasing in newly diagnosed patients with breast cancer [345]. The role of MRI in determining the candidacy for BCS remains controversial because MRI findings have been shown to increase mastectomy rates without evidence of improved local control [267].
The accuracy of MRI compared with conventional imaging in predicting the pathologic tumor size remains controversial. Several studies reported that MRI is superior to mammography or US in preoperative assessment of the extent of the pathologic tumor, thereby suggesting the importance of MRI in surgical planning [89]. In contrast, other studies indicated that US had a better correlation with tumor size compared with MRI [1011]. Moreover, the discordance of MRI pathologic in predicting tumor size is affected by several factors, including histologic type and estrogen receptor (ER) status [1213].
In this study, to compare the ability of MRI and US in predicting the extent of the tumor, we investigated the correlation efficiency between the 2 imaging studies and pathologic examinations. Moreover, we compared the imaging-pathologic size correlation in conjunction with the intrinsic subtypes. Finally, we investigated the actual positive margin and re-excision rates in patients undergoing BCS after preoperative MRI.
METHODS
Patients and ethics
From January 1, 2011 to November 30, 2016, patients who were newly diagnosed with breast cancer and underwent BCS at Gangnam Severance Hospital were included in the study. Patients undergoing BCS with single tumor were included to avoid the influence of multiple tumors. Patients with ductal carcinoma in situ or lobular carcinoma in situ, those with multifocal or multicentric tumor, and who underwent total mastectomy were excluded. Moreover, patients receiving neoadjuvant chemotherapy were also excluded. Cases of invasive cancer diagnosed after simple excision or vacuum-assisted core biopsy were excluded. Preoperatively, MRI and US evaluation were conducted in all patients. Furthermore, the expression of ER, progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) was evaluated. The modified Scarf-Bloom-Richardson grading system was used for tumor grading.
The study protocol was reviewed and approved by the Institutional Review Boards (IRB) of the Gangnam Severance Hospital and were adherent to the guidelines of the Declaration of Helsinki (IRB No. 3-2018-0146). The need for informed consent was waived under the approval of the Institutional Review Board due to the retrospective study design.
Operative procedure and pathologic evaluation
During surgery, we avoided removing excessive volume; the decision was made based on the tumor size measured by MRI and US. After removing the main tumor, separate cavity shaving in superior, inferior, lateral, and medial margins was performed, followed by intraoperative frozen-section examination in an en face fashion. In general, the outer surface of each margin was marked with a silk suture. Thereafter, cavity margins were cut parallel to the marked largest surface and evaluated microscopically to identify the presence of tumor cells [14]. When the margin was positive, an additional margin shaving was performed.
Definition of tumor extent and positive margin
Pathologic tumor size was defined as the maximum extent where tumor including in situ cancer was involved. The positive margin was defined as the presence of invasive or in situ cancer in shaved margin evaluated by intraoperative frozen-section examination. The presence of atypical cells or lobular carcinoma in situ was considered as negative margin. A second surgery for margin clearance was performed when the margin was positive in the final pathologic examination, considering other pathologic and clinical characteristics, including age, tumor size, grade, and other risk factors.
Immunohistochemistry (IHC) markers
In our IHC study, formalin-fixed, paraffin-embedded tissue sections obtained from surgical specimens were stained using appropriate antibodies specific for 4 markers: ER (1:100 dilution, clone 6F11; Novocastra, Newcastle upon Tyne, UK), PR (clone 16; Novocastra), HER2 (4B5 rabbit monoclonal antibody; Ventana Medical Systems, Tucson, US), and Ki-67 (MIB-1; Dako, Glostrup, Denmark). The HER2 status was defined as positive with a score of 3+ and negative with a score of 0 or 1+. Tumors with scores of 2+ were analyzed by fluorescent in situ hybridization following the manufacturer's protocol (PathVysion kit; Vysis, Downers Grove, US or HER2 inform; Ventana Medical Systems).
IHC-based subtype
Tumors were classified into 3 molecular subtypes based on ER, PR, and HER2 expression: luminal/HER2-negative (ER-positive and/or PR-positive), HER2-positive (irrespective of ER and PR), and triple-negative breast cancer (TNBC; ER-negative, PR-negative, HER2-negative).
Statistical analysis
The correlation between tumor extent measured by imaging studies (MRI or US) and pathologic examination was assessed using Lin's concordance correlation coefficient. The subtypes were compared using a post hoc test. Discrete variables were compared using the χ2 test or Fisher's exact test. Variables with p < 0.05 in the univariate analysis were included in the multiple logistic regression analysis, and backward elimination was performed to identify risk factors for positive margin. All analyses were performed using SPSS version 18 (SPSS, Chicago, USA) and SAS (version 9.4; SAS Inc., Cary, USA) software. Statistical significance was defined as a p-value < 0.05.
RESULTS
Patient characteristics
Overall, 516 patients were included in the study. Baseline characteristics of the patients are shown in Table 1. The mean ± standard deviation age of patients was 52.3 ± 11.0 years. All patients had T1 or T2 cancer. Of 516 patients, 327 were luminal/HER2-negative, 82 were HER2-positive, and 107 had TNBC. The average tumor size measured by MRI and US was 17.8 ± 7.7 and 16.6 ± 7.7 mm, respectively. The mean of pathologic size was 17.5 ± 7.3 mm. Among the imaging studies and pathologic examination, the tumor size of the HER2-positive subtype and TNBC was larger than luminal/HER2-negative subtype.
Table 1
Baseline characteristics
Values are presented as median or mean (range) or number (%).
HER2 = human epidermal growth factor receptor 2; TNBC = triple-negative breast cancer; IDC = invasive ductal carcinoma; ILC = invasive lobular carcinoma; HG = histologic grade; US = ultrasonography; MRI = magnetic resonance imaging.
*Missing value; †Fisher's exact test.
Correlation of imaging and pathology with tumor size
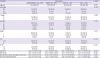
The tumor size measured by MRI was better correlated with pathologic size than US (r = 0.6975 for MRI vs. r = 0.6211 for US, p = 0.001) (Table 2, Figure 1). The concordance coefficient of MRI and US in predicting the pathologic tumor size of luminal/HER2-negative and HER2-positive breast cancer was not different. However, in TNBC, the tumor size measured using MRI was more consistent with pathologic tumor extent than that observed using US (r = 0.8089 for MRI vs. r = 0.6014 for US, p < 0.001; Table 2, Figure 1). The concordance correlation coefficient between pathologic size and MRI or US was the lowest in the HER2-positive subtype (r = 0.5243 for MRI, r = 0.4898 for US) compared with that in other subtypes. The concordance correlation coefficient between pathologic size and MRI was significantly lower for the HER2-positive subtype than for the luminal/HER2-negative subtype (p = 0.037) and TNBC (p < 0.001; Supplementary Table 1).
Table 2
Concordance correlation coefficient between pathologic size and US or MRI


Positive margin and re-excision rates based on the subtypes
Among the 516 patients, 76 (14.7%) had positive margin in the intraoperative frozen-section examination. In these patients, margin was further resected and confirmed to be negative in the intraoperative frozen-section examination. Moreover, 24 (4.7%) patients underwent a second surgery for margin clearance because the result of negative margin in the intraoperative frozen-section examination was converted to be positive in the final pathologic evaluation. A significant difference in positive margin rate was found among the subtypes (luminal/HER2-negative: 11.6%, HER2-positive: 23.2%, TNBC: 17.8%, p = 0.019; Figure 2A). However, in secondary operation, no difference in margin clearance was observed based on the subtypes (p > 0.999; Figure 2B). In the post hoc test, the HER2-positive subtype was more likely to show positive margins than the luminal/HER2-negative subtype. In addition, the positive margin rate was higher in the HER2-positive group than in the HER2-negative group (Figure 2C); however, the secondary operation rate was not different based on HER2 status (Figure 2D).
Figure 2
Positive margin and re-excision rates according to subtypes. (A) Positive margin rates and (B) re-excision rates based on subtypes (luminal/HER2-negative, HER2-positive, and TNBC), (C) positive margin rates and (D) re-excision rates based on HER2 expression.
HER2 = human epidermal growth factor receptor 2; TNBC = triple-negative breast cancer.

Logistic regression analysis
In the univariate analysis, ER and HER2 were independent risk factors for positive margin. Multivariate analysis revealed that only HER2 positivity was an independent risk factor for positive margin on intraoperative frozen sections (Table 3). Additionally, ER negativity showed a strong trend as a risk factor of intraoperative positive margin.
Table 3
Positive margin-related factors in univariable and multivariable analysis

DISCUSSION
Breast MRI has been used as a supplementary imaging tool in preoperative work-up. Although the sensitivity of MRI was 90%, its specificity was relatively low (75%) [15], frequently causing false-positive findings requiring additional procedures or biopsies. Previous meta-analyses showed that incorporation of MRI into surgical planning in patients with breast cancer might lead to higher mastectomy rates without lowering the re-excision rates or local recurrence [26]. However, the routine use of MRI in patients with newly diagnosed breast cancer remains a debatable topic.
For patients with lobular carcinoma and multifocal disease and for those diagnosed with occult disease using mammography or US, MRI can be beneficial [161718]. Moreover, MRI has been known to be the most accurate radiologic tool that can measure tumor diameter [1920]. In several studies, MRI measured the tumor size more accurately than US [89].
In our study, we determined whether MRI could more accurately predict the tumor extent than US and compared the accuracy between MRI and US based on the molecular subtypes of breast cancer. Moreover, we investigated whether the rate of positive margin and secondary operation differed based on the molecular subtypes using selected patients who underwent BCS based on the preoperative results of MRI and US. To this end, we selectively included patients with unifocal tumor because meticulous measurement of tumor extent is difficult in patients with multifocal disease. Moreover, patients who underwent mastectomy with futile margin assessment were excluded. In this perspective, we found that MRI superiorly predicted the pathologic tumor extent compared to US, especially in TNBC. Moreover, MRI and US did not precisely predict the pathologic size in the HER2-positive subtype, compared to that in other subtypes.
In detail, MRI was more concordant with pathologic tumor size than US in all patients (MRI, r = 0.6975 vs. US, r = 0.6211; p = 0.001). Franca et al. reported that breast MRI was more significantly correlated with the pathological examination than mammography (r = 0.872 vs. 0.710) or US (r = 0.836 vs. 0.704). Moreover, several earlier studies have shown that US underestimates the pathologic tumor size [101221]. Collectively, our finding was expected because subclinical tumor area that is invisible through US might be identified using MRI.
In further analyses of the molecular subtypes, MRI can effectively measure the pathologic extent, compared to US, in TNBC only; however, the same relationship was not found in other subtypes. The ability of MRI in estimating the tumor size based on the subtypes is not well explored. The study by Yoo et al. [13] suggested that the discordance rate between MRI and pathologic tumor size is higher in ER-negative tumors than in ER-positive tumors. Although the discordance of MRI pathology was not compared based on the ER status, our result might be consistent because ER negativity was noted as a risk factor for positive margin rate.
The poor performance of preoperative imaging in predicting tumor area in HER2-positive breast cancer may raise a question regarding the increase in positive margin rates or secondary operation for margin clearance in patients with HER2-positive breast cancer. Indeed, the relationship of imaging-pathologic size was least correlated in the HER2-positive subtype. This provided a rationale for the highest rate of positive margin as 23.2% in the HER2-positive subtype. The difference in re-excision rate was not significant between the subtypes, which might be largely attributable to the intraoperative frozen section examination that enables further resection in case of intraoperative-positive margins. If the intraoperative margin assessment is not performed, the correlation between imaging and pathologic size may result in increased secondary operation as margin clearance. In addition, our result is concordant with those of the study by Baek et al. [22] where HER2 overexpression was shown to cause inaccurate assessment of tumor size. While the mechanism in which the HER2 overexpression reduces the accuracy of breast MRI is unclear, angiogenesis may be one of causes. A hypoxic region within a tumor that stimulates the generation of new vessels is known to decrease the accuracy of contrast-enhanced MRI [2324]. HER2 expression is associated with increased angiogenesis via the modulation of pro- and anti-angiogenic factors [2526], which may hamper accurate measurement of tumor size in the HER2-positive subtype.
The major limitation of this study is its retrospective design. Particularly, since a new marginal guideline was published in February 2014, a half or our patients underwent lumpectomy under more conservative margin consensus. Thus, the results regarding the positive margin rate or re-excision rate should be carefully appraised. The role of MRI to reduce positive margin based on subtypes warrant further prospective study. Randomized trial comparing the outcome of patients with and without MRI would provide a definite conclusion. Another limitation is the small number of patients with HER2-positive cancer (82 of 516). Our finding that the positive margin rate was higher in the HER2 subtype needs to be verified in a larger cohort.
In conclusion, breast MRI was superior to US in the preoperative assessment of the pathologic extent of tumor size; this was most evident in TNBC. Nevertheless, the size correlation of MRI was low and the positive margin rate was higher in the HER2 subtype than in the other subtypes. A careful approach is needed to obtain negative margin in patients with HER2-positive breast cancer undergoing BCS.
 XML Download
XML Download