

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Breast cancer is notorious for its propensity to metastasize. It is common for breast cancer to recur or metastasize years after complete remission [12]. Some authors claim that breast cancer is a systematic disease from its early stages and has metastatic potential regardless of its size [3]. While the characteristics of the primary tumor are usually preserved in metastases, studies indicate a change in biomarker status in metastatic breast cancer (MBC) [45]. An example of this is the “receptor conversion” phenomenon which involves changes in estrogen receptor (ER), progesterone receptor (PR) or human epidermal growth factor receptor 2 (HER2) in MBC.
The cause of receptor conversion during metastatic progression is yet to be elucidated, but there are some theories regarding the process, one of which is intra-tumoral heterogeneity. This theory states that breast cancer cells within a single tumor mass can exhibit phenotypic and genetic heterogeneity, with only a small number of these cells acquiring metastatic potential and forming a metastatic lesion [3]. If biomarker status is heterogeneous in the primary tumor and is associated with different metastatic potential, then it can also change during metastatic progression. Another theory refers to selection pressure from treatment. A patient diagnosed with breast cancer receives endocrine or HER2-targeted therapy according to the receptor status. Only breast cancer cells that have survived the therapy's selective pressure can form a metastatic tumor, further increasing the chance that a metastatic lesion shows altered biomarker status [67].
The importance of re-evaluation of biomarker status in metastatic lesions has been emphasized in a previous clinical practice guideline [8]. Since the receptor status in breast cancer is directly related to the patient's treatment, it is necessary to identify any receptor conversions in MBC. Negative conversion generally means that the current medication is no longer effective, and positive conversion suggests a chance for a new therapy. However, tissue confirmation of MBC remains optional and is not routinely performed. The reported incidence of receptor conversion varies largely between studies [5], and characteristics of MBCs with receptor conversion have not been established. Receptor conversion is also known to have an impact on the clinical outcomes in patients with MBC. Of note, negative conversion of hormone receptor status is associated with poor clinical outcomes [9101112], whereas its prognostic significance remains ambiguous.
In this study, we aimed to evaluate the frequency of biomarker changes in patients with MBC diagnosed at our institution and to identify the characteristics of tumors that have undergone a change in biomarker status. We also investigated the impact of biomarker alterations on the prognosis of patients with MBC.
METHODS
Patients and samples
This retrospective study included 152 patients diagnosed with MBC through tissue confirmation from May 2005 to April 2017 at Seoul National University Bundang Hospital. All patients had at least 2 different tumor tissues, one from the primary tumor (either biopsy or resection specimen) and the other from the metastatic tumor(s) (biopsy or resection specimen, single or multiple sites). In cases with multiple metastatic lesions, the tumor sample from the first metastatic site was used for analysis. Loco-regional metastases including lymph node (axillary, internal mammary and supraclavicular), skin, and chest wall recurrences were also counted as metastatic lesions.
A pair of formalin-fixed and paraffin-embedded tumor samples from the primary and metastatic sites were collected. Medical records and hematoxylin and eosin-stained sections were reviewed to acquire clinicopathological information including age, sex, initial clinical or pathological tumor, node, metastasis (TNM) stage, metastatic sites, histological subtype, histological grade, and biomarker status. This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (protocol No. B-1601/332-304), and informed consent was waived.
Immunohistochemical analyses and scoring
For each case, basic biomarkers were reviewed on immunohistochemistry (IHC) slides. All IHC staining procedures were performed using BenchMark XT autostainer (Ventana Medical Systems, Tucson, USA) with an UltraView detection kit (Ventana Medical Systems). The following antibodies were used: ER (1:100; clone SP1; Labvision, Fremont, USA), PR (1:70; PgR 636; Dako, Carpinteria, USA), HER2 (ready to use; clone 4B5; Ventana Medical Systems), p53 (1:600; D07; Dako), and Ki-67 (1:250; MIB-1; Dako). ER and PR were considered positive if there were at least 1% positive tumor nuclei. For ER and PR, expression level was scored in 10% increments, and their Allred scores were calculated [13]. HER2 expression was scored according to 2013 American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines [14]. For Ki-67 proliferation index, positive staining in 20% or more tumor cells was regarded as a high index. As biomarker status can change after neoadjuvant chemotherapy (especially PR and Ki-67 proliferation index) [1516], we used the biomarker data from the pre-treatment needle biopsy specimen in patients who received neoadjuvant chemotherapy.
Determination of HER2 status
HER2 status was determined via HER2 fluorescence in situ hybridization or silver in situ hybridization (SISH) for cases with equivocal HER2 IHC. HER2 SISH was also performed in cases that showed discrepant results in HER2 status between primary and metastatic tumors. HER2 SISH assays were performed with INFORM HER2 DNA and Chromosome 17 probes (Ventana Medical Systems) using an ultraView SISH Detection Kit (Ventana Medical Systems) as previously described [17]. After scanning the whole section, at least 50 cells were evaluated in each case, and HER2 status was determined according to the 2013 ASCO/CAP guidelines [14]. In this study, HER2-equivocal cases were regarded as HER2-non-amplified for statistical analysis.
Definition of breast cancer subtypes
Breast cancer subtypes were categorized according to the 2011 St. Gallen Expert Consensus [18] as follows: luminal A (ER+ and/or PR+, HER2−, Ki-67 < 14%), luminal B (ER+ and/or PR+, HER2−, Ki-67 ≥ 14%; ER+ and/or PR+, HER2+), HER2+ (ER−, PR−, HER2+), and triple-negative (ER−, PR−, HER2−) subtypes.
Statistical analysis
Statistical significance was assessed using Statistical Package, SPSS version 19.0.0 for Windows (IBM Corporation, Armonk, USA). Paired sample t-test was used to compare continuous variables between primary and metastatic tumors. Mann-Whitney test was used when the variables did not satisfy the assumption of normality. Kruskal-Wallis test and subsequent Mann-Whitney test were used when comparing more than 2 groups. When needed, corrections for multiple testing were made using the Bonferroni method, and adjusted p-values were presented. Progression-free survival (PFS) was calculated from the date of diagnosis of primary tumor to the date of first loco-regional or distant metastasis. For patients initially staged as M1, PFS time was considered zero. Overall survival (OS) was estimated from the date of diagnosis of primary tumor to date of death from any cause. Survival curves were estimated by the Kaplan-Meier method, and the significance of differences was assessed using the log-rank test. Univariate and multivariate analyses were performed with Cox proportional hazard model for OS. Hazard ratio (HR) and 95% confidence intervals (CIs) were calculated. Unless otherwise specified, p-values less than 0.05 were considered statistically significant, and all reported p-values are 2-sided.
RESULTS
Clinicopathological characteristics of the patients
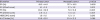
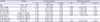
The clinicopathological characteristics of the patients are summarized in Table 1. Of the 152 patients, 14 patients presented with MBC at the time of diagnosis, and 138 patients were diagnosed with MBC during follow-up. There were 64 cases of loco-regional metastases, of which there were 30 cases of chest wall recurrence, 30 cases of supraclavicular, axillary, internal mammary, or Rotter's node metastases, and 4 cases of breast or axillary skin recurrence. There were 88 cases of distant metastasis, of which there were 8 cases of mediastinal lymph node metastases, 1 case of cervical lymph node metastasis, and 4 cases of skin metastases other than breast or axillary such as abdomen. Eighty-seven patients received neoadjuvant chemotherapy; in these cases, we used clinical stage instead of pathological stage for initial TNM staging. Initial T1 stage included one case of microinvasive carcinoma. Initial N1 stage included three cases of micrometastases. Invasive carcinoma of no special type was the most common histological subtype (132 cases, 85.5%), followed by invasive lobular carcinoma (6 cases, 3.9%) and metaplastic carcinoma (6 cases, 3.9%). Other histological subtypes included three cases of mucinous carcinoma, three of mixed ductal and lobular carcinoma, one of micropapillary carcinoma, and one of apocrine carcinoma.
Table 1
Clinicopathologic characteristics of the patients

Values are presented as numbers of cases (%) or median (range).
ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2.
![]()
Biomarker expression level in primary and metastatic tumors
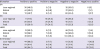
In paired analyses of primary and metastatic tumors, ER and PR expression levels generally decreased during metastatic progression (Table 2). The decrease in PR expression level was more substantial (mean, 20.4% to 7.8%, p < 0.001) than ER (mean, 43.5% to 37.3%, p = 0.003). Allred scores for ER and PR also decreased significantly (4.14 to 3.69, p = 0.001; 2.89 to 1.36, p < 0.001, respectively). However, there was no significant change in HER2 expression levels and Ki-67 index during metastatic progression.
Table 2
Paired analyses of biomarker expression levels between primary and metastatic tumors
p-values were calculated by paired sample t-tests. Data are presented as mean ± standard deviation.
ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2; IHC = immunohistochemistry.
![]()
Biomarker changes during metastatic progression
We classified patients into 4 groups according to biomarker alterations during metastatic progression: positive to positive (remained positive), positive to negative (negative conversion), negative to negative (remained negative), and negative to positive (positive conversion) (Table 3). Negative conversion occurred more frequently than positive conversion in hormone receptors. Negative conversion occurred in 8 cases (5.3%) for ER and 37 (24.3%) for PR, whereas positive conversion occurred in 1 case (0.7%) for ER and 3 (2.0%) for PR. Negative conversion of PR was the most frequent change among all biomarker alterations. HER2 negative conversion occurred in 9 cases (5.9%) and positive conversion in 3 (2.0%). For Ki-67 proliferation index, change from a low to high index (20 cases, 13.2%) occurred more frequently than from a high to low index (9 cases, 5.9%). Representative images of biomarker conversion are shown in Figure 1. We subdivided the patients into 2 groups, loco-regional and distant metastasis, and found no significant difference in receptor conversion rates between the 2 groups (Table 3). We also analyzed biomarker changes according to the initial M stage. There were minor differences in the frequencies of biomarker changes between initial M0 and initial M1 groups, but none of these changes were statistically significant (Supplementary Table 1).
Table 3
Biomarker changes during metastatic progression
Data are presented as numbers of cases (percentage).
ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2.
*For Ki-67 index, positive indicates a high proliferation index (≥ 20%) and negative represents a low proliferation index (< 20%).
![]()
 | Figure 1A representative image of biomarker conversion. The left column is from the primary tumor, and the right column is from the metastatic tumor. ER (A, B) and PR (C, D) show negative conversion in the metastatic tumor. HER2 (E, F) exhibits positive conversion. Ki-67 index (G, H) reveals alteration from a low to high index. (A-H) Immunohistochemical staining, ×200 magnification.ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2.
|
As ER and PR expression are closely related to each other, we classified patients with combined hormone receptor status and observed changes in biomarker expression in the metastatic tumors (Supplementary Table 2). All ER-PR+ primary tumors were ER-PR− in metastatic tumors. Primary ER-PR− tumors rarely gained positivity at the metastatic sites, and positive conversion of both ER and PR never occurred.
When comparing hormone receptor expression levels in primary tumors between the positive to positive (remained positive) and positive to negative (negative conversion) groups, ER expression levels were significantly lower in the negative conversion group (median, 90.0% vs. 35.0%, positive to positive vs. positive to negative; p = 0.001) (Supplementary Table 3). As for HER2, cases with positive to negative conversion frequently showed 1+ or 2+ HER2 IHC in primary tumors, compared to positive to positive cases (77.8% vs.11.1%; p < 0.001) (Supplementary Table 4). We also performed HER2 SISH in representative tissue sections of primary and metastatic tumors, which showed discrepant results for HER2 status, and we found that four of the nine cases with HER2 negative conversion showed heterogeneous HER2 gene amplification in the primary tumor.
When analyzing changes in the breast cancer subtypes during metastatic progression (Table 4), all primary triple-negative breast cancers remained triple-negative in the metastatic lesion. While none of the luminal A subtype changed to triple-negative during metastatic progression, 7 (11.9%) cases of the luminal B subtype changed to triple-negative. Nonetheless, these changes were not statistically significant.
Table 4
Changes in breast cancer subtype during metastatic progression
Subtype was classified according to 2011 St. Gallen Expert Consensus. Data are presented as numbers of cases (percentage).
HER2 = human epidermal growth factor receptor 2.
![]()
Frequency of biomarker changes according to the metastatic sites
Frequencies of biomarker changes according to the metastatic site are shown in Table 5. Biomarker changes occurred relatively frequently in liver metastasis (ER in 4 [16.7%]: PR in 8 [33.3%]; HER2 in 4 [16.7%]; and Ki-67 in 5 [20.8%] cases) compared to other sites. In brain metastasis, no changes in ER, PR, or HER2 status were observed. In skin metastasis, no changes in ER or HER2 status were found. In lung metastasis, no changes in ER status were found. As for bone metastasis, no changes in HER2 status were observed. However, these results were not statistically significant possibly due to the small sample size. Other metastatic sites not shown include the uterine adnexa, stomach, and ampulla of Vater.
Table 5
Frequencies of biomarker changes according to the metastatic sites

Data are presented as numbers of cases (percentage).
ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2; LN = lymph node.
![]()
Prognostic significance of biomarker changes in metastases
In the next step, we compared PFS time with regards to biomarker changes during metastatic progression (Table 6). PFS time was significantly longer in persistent hormone receptor-positive groups than in persistent hormone receptor-negative groups (persistent ER-positive vs. persistent ER-negative, adjusted p < 0.001; persistent PR-positive vs. persistent PR-negative, adjusted p < 0.001). PR-negative conversion group showed longer PFS than persistent PR-negative group (adjusted p = 0.024). Although ER-negative conversion seemed to be associated with decreased PFS compared to persistent ER-positive status, the result was not statistically significant (adjusted p = 0.192). There was no statistical difference in PFS with respect to alterations of HER2 and Ki-67.
Table 6
Comparison of progression-free survival (years) for biomarker alteration during metastatic progression

Data are presented as median (interquartile range). p-values were calculated by Mann-Whitney test after Kruskal-Wallis test and adjusted by Bonferroni's method.
ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2.
*,†adjusted p < 0.001; ‡adjusted p = 0.024.
![]()
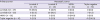
In the Kaplan-Meier survival analysis for OS (Figure 2), the persistent ER-negative group showed lower OS than the persistent ER-positive group (p < 0.001). Moreover, positive to negative alteration (negative conversion) of ER was associated with decreased OS compared to persistent ER-positive status (p = 0.001). However, changes in PR, HER2, and Ki-67 showed no prognostic significance.
 | Figure 2Kaplan-Meier survival analysis for OS according to estrogen receptor status change. Patients with persistent ER-negative tumors (blue line) show decreased OS compared to those with persistent ER-positive tumors (green line) (p < 0.001, log-rank test). ER-negative conversion group (yellow line) shows poor OS compared to persistent ER-positive group (green line) (p = 0.001, log-rank test).OS = overall survival; ER = estrogen receptor.
|
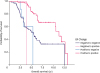
Table 7 shows univariate and multivariate analyses of OS in primary ER-positive tumors. In multivariate analysis, ER-negative conversion in the metastatic site was found to be an independent prognostic factor for decreased OS (HR, 6.255; 95% CI, 1.758–22.263; p = 0.005).
Table 7
Univariate and multivariate analyses of overall survival in primary ER-positive tumors
HR = hazard ratio; CI = confidence interval; [M] = metastatic; ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2.
![]()
DISCUSSION
It is widely accepted that receptor conversion occurs during metastatic progression of breast cancer; however, its reported incidence is quite variable. Schrijver et al. [5] reported in their meta-analysis that the pooled percentage of positive to negative conversion in ER, PR, and HER2 was 22.5%, 49.4%, and 21.3%, respectively. Conversely, the percentage of negative to positive conversion was 21.5%, 15.9%, and 9.5%. In the present study, positive to negative conversion was found in 5.3%, 24.3%, and 5.9% while negative to positive conversion was found in 0.7%, 2.0%, and 2.0% for ER, PR, and HER2, respectively. The frequency of biomarker conversions, especially that of positive conversion, was relatively low in comparison to previous reports. These discrepancies may have been due to differences in the examined population, data collection methods, and analytical issues. Biomarkers usually undergo adverse changes, as shown in this study. Negative conversion was more frequent in hormone receptors, and positive conversion was more frequent in Ki-67 index. Almost half of ER-positive and PR-positive primary tumors (29 cases, 45.3%) changed to ER-positive and PR-negative tumors which are associated with worse biological behavior compared to ER-positive and PR-positive tumors [619].
The reason for receptor conversion in metastatic lesions remains unclear. Changes in receptor status could be due to a true switch in the biology of the disease, a sampling error in focally receptor-positive cancers, or limited accuracy and reproducibility of receptor assays. All cases included in the present study were immunohistochemically stained using the same method at a single institution and evaluated by a single experienced breast pathologist (SYP). In a previous study, we demonstrated that the concordance rate of biomarker expression between core needle biopsies and excised specimens was excellent in our institution with a rate of 99.0% for ER and 97.1% for PR [20]. Considering these factors, it would be reasonable to assume that receptor conversion reflects a genuine switch in the biology of the disease rather than being a result of sampling error or limited reproducibility.
In this study, cases with ER-negative conversion showed low expression levels compared to persistent ER-positive tumors. Of the eight cases exhibiting ER-negative conversion, six showed ER-positive staining in less than 50.0% of the tumor cells in primary tumor. Thus, it is possible that the ER-negative tumor cells in those tumors which were resistant to endocrine therapy acquired metastatic potential during disease progression. Moreover, of the nine cases exhibiting HER2 negative conversion in metastases, seven showed 1+ or 2+ HER2 IHC and four showed HER2 heterogeneity in the primary tumor. All nine patients were treated with trastuzumab. Therefore, it is probable that the HER2-negative clones survived HER2-targeted therapy and progressed to metastatic disease. Hence, our study revealed the possible role of intratumoral heterogeneity in receptor conversion.
So far, a few studies have attempted to find factors related to receptor discordance [212223]. Among the possible associated factors suggested are metastatic location (loco-regional or distant metastasis), time interval, and intervening therapy. However, none of them showed a significant relationship with receptor conversion. In this study, no difference in receptor conversion rates was observed between loco-regional recurrence and distant metastases. In metastatic location-specific analysis, we were not able to obtain meaningful results probably due to the small sample size, with the exception of relatively frequent biomarker conversion in the liver. As for time intervals, we did not find a statistical difference between biomarker-concordant group and discordant group although tumors with ER-negative conversion seemed to show decreased time to relapse compared to persistent ER-positive tumors. However, analysis of additional cases is needed to obtain more reliable findings.
ER-negative conversion proved to be an independent prognostic factor in the present study. Previous studies showed variable results with respect to prognosis from receptor alteration during metastatic progression of breast cancer: some reported no significant survival difference [242526], whereas others found a negative prognostic effect of hormone receptor-negative conversion [9101112]. In studies with no significant results, there was at least a trend for decreased survival. Prognostic significance was usually found in hormonal receptor changes, and it was also previously found in HER2 changes [1227], which was not apparent in this study. Taken together, it seems that negative conversion of hormone receptor status is undeniably a poor prognostic indicator.
Many retrospective studies have suggested that differences between primary and metastatic lesions lead to dismal outcomes. However, prospective studies have shown that these differences are no longer associated with worse outcomes if clinicians adjust treatment based on the results from a metastatic lesion [2328]. In light of such evidence, recent guidelines [8] insist that re-evaluation of MBC lesions, including biomarker status, is important. Some even suggest multiple metastases should be biopsied for the optimal reassessment of receptor status [29]. This re-evaluation is significant in three aspects: definite diagnosis of metastasis at a histological level, possible changes in treatment based on altered biomarker status, and prognostication.
Since positive conversion of biomarker status is not a frequent phenomenon in metastases, the chance of implementing a new line of treatment is not high. However, a few studies have shown positive response to treatment after including HER2-targeted therapy based on HER2 positive conversion in metastatic tumors. Chang et al. [7] showed that 2 out of 5 patients with HER2 positive conversion achieved partial response with trastuzumab therapy. Fabi et al. [30] reported that patients whose HER2 status changed from negative to positive in metastases showed significantly longer PFS when treated with trastuzumab compared to those who were not treated. In this study, three patients showed HER2 positive conversion, and one of them received trastuzuamb based on the positive HER2 status in the recurrent tumor. After 3-years of follow-up, the patient is still progression-free after receiving HER2 targeted therapy. While the odds are still low, this is an important result that should not be neglected.
In cases of negative conversion, theoretically, therapy should be discontinued to avoid unnecessary side effects of the treatment. However, in clinical practice it is not easy to make such a decision since it is uncertain whether the evaluated metastatic lesion represents all of the metastatic burden left in the patient's body. The 2015 ASCO clinical practice guideline [8] suggests preferential use of the results from the metastatic site to direct therapy if supported by the clinical scenario and patient's goal of care. Whether altered receptor status in metastatic sites has an effect on drug response is yet to be elucidated, and further large-scale prospective studies are needed.
There are several limitations in this study. First, the follow-up period was relatively short. We collected data from patients who were diagnosed with MBC from 2005 to 2017, and the median follow-up period was about 5 years. In the most recent cases, the follow-up period was not long enough to observe any events. Second, this was a small, retrospective study. Thus, the patients had been treated with various modalities. Moreover, in some of the subgroup analyses, it was impossible to obtain significant results due to the small number of subjects. Additional studies using a large number of homogeneously-treated cases with long-term follow-up should yield more meaningful results.
In conclusion, biomarker changes occur rather frequently in MBCs, usually in an unfavorable direction. Negative conversion of ER was found to be an independent poor prognostic indicator. Therefore, it is important to re-evaluate basic biomarkers in metastatic lesions for proper management and better prognostication of patients with metastatic breast cancer.
 XML Download
XML Download