

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neoadjuvant chemotherapy (NAC) is the standard treatment of choice for patients with locally advanced or inoperable breast cancer. It is increasingly used in patients with large operable breast cancer to perform breast-conserving surgery (BCS) or eradicate clinical axillary lymph node (LN)-positive disease [1]. The benefits of NAC include a reduction in the size of breast tumors to enable performance of BCS previously requiring total mastectomy and eradication of metastatic axillary LNs with increasing need for sentinel LN biopsy previously requiring axillary LN dissection [23]. NAC offers similar outcomes to that of postoperative adjuvant chemotherapy in terms of disease-free survival and overall survival [45].
Pathologic complete response (pCR) has been considered as the most important predictor of NAC outcomes and has emerged as a surrogate prognostic marker in many clinical trials. Patients achieving pCR in the breast and axillary LN after NAC have improved locoregional and survival outcomes irrespective of the initial stage and molecular subtype [467]. Breast cancer was classified into five major molecular subtypes based on estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and Ki-67 expression: luminal A, luminal B HER2−, luminal B HER2+, HER2+, and triple-negative breast cancer (TNBC) [8]. In NAC for breast cancer, pCR rates widely vary depending on the breast cancer subtype. The pCR rate is lower after NAC in luminal breast cancer, which is defined as the high expression of hormone receptor (HR) and absence of HER2 overexpression or amplification, compared with those in HER2+ and TNBC subtypes, despite the better overall prognosis [91011]. Luminal breast cancer had a reported pCR rate ranging from 6% to 11%. Therefore, NAC is less effective in luminal breast cancer than in other subtypes; thus, the decision to administer NAC to these patients remains controversial. As a result, neoadjuvant endocrine therapy (NET) and surgery as initial treatment are potential treatment options for luminal breast cancer [1213].
Although pCR is rarely achieved in luminal breast cancer, patients with this subtype showed good partial response to NAC, which enables performance of BCS in patients originally requiring total mastectomy [11]. Therefore, pCR is not the most important predictive marker of tumor response in luminal breast cancer for the performance of BCS. There are limited data regarding the rates of tumor response based on the histological subtype of breast cancer after NAC. Although several studies have examined the BCS conversion rate according to the histological subtype of breast cancer, the BCS conversion rate alone has limitations in evaluating the benefits of NAC.
In the present study, we classified HR+/HER2− breast cancers as luminal HER2− breast cancer and other subtype breast cancers as non-luminal HER2− breast cancer. We analyzed the factors associated with BCS conversion and therapeutic efficacy of NAC for surgical outcomes including BCS conversion and tumor response rate in luminal HER2− breast cancer. We also investigated the factors that predict good tumor response among patients who received NAC.
METHODS
Patient population
A prospectively collected database of 3,229 patients who underwent breast cancer surgery at the Seoul St. Mary's Hospital, from January 2010 to December 2016 was reviewed. Among these patients, we identified patients with clinical stage II or III primary breast cancer who received NAC before surgery. Patients who had not completed all regimens due to toxicity and without confirmed axillary LN metastasis were excluded. All eligible patients had axillary LN metastasis at presentation confirmed by core needle biopsy of axillary LN. All patients received chemotherapy before breast and axillary surgery. The patients subsequently underwent either BCS or total mastectomy with axillary LN dissection. Thus, a total of 244 patients with confirmed axillary LN metastasis received chemotherapy and subsequently underwent surgery of the primary tumor with concurrent axillary LN dissection. All patients received sequential or combination chemotherapy consisting of anthracycline and taxane. For some patients with HER2-type breast cancer, trastuzumab was included in the NAC. The study protocol was approved by the Institutional Review Board of Seoul St. Mary's Hospital (KC 18RESI0738). Informed consent from the patients was not required in this study.
Assessment of surgery and response
Mammography, breast ultrasonography, and breast magnetic resonance imaging (MRI) were performed to determine the response to therapy before (baseline) and after NAC (before surgery). Before and after NAC, through these evaluations, the surgeon assessed patients who were unable to undergo BCS based on the following criteria: 1) the size of the tumor was > 5 cm including non-mass enhancement on the MRI and suspicious microcalcification on mammography; 2) the tumor extended to the nipple-areolar complex before NAC, even if the response was good after NAC; 3) the extent of the tumor was > 25% of the total breast volume; 4) tumor was multicentric.
Tumor response rate was defined as the calculated percent rate of tumor and axillary LN size reduction between baseline and before surgery. The tumor response rate was calculated according to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria. Two experienced radiologists performed the visual assessment and calculation of tumor and axillary response rates in breast MRI. The BCS conversion rate was defined as the percentage of patients who initially required total mastectomy before NAC but were converted to BCS after NAC, excluding those with inflammatory breast cancer.
Pathological diagnosis and intrinsic subtypes
Breast and axillary LN status was evaluated using core needle biopsy before NAC. From the initial core needle biopsy, ER, PR, HER2, and Ki67 expression and histologic grade were evaluated. Breast cancer subtypes were defined by HR and HER2 status. Positive ER status and PR status were defined as an Allred score ≥ 3 or nuclear staining ≥ 1%. Immunohistochemistry (IHC) or fluorescence in situ hybridization (FISH) was performed to evaluate the HER2 status. Positive HER2 status was defined as an IHC score of 3+ or 2+ with confirmed HER2 gene amplification by FISH in accordance with the American Society of Clinical Oncology/College of American Pathologists guidelines [14]. Ki-67 was classified based on cutoff points according to the expressed cell ratio (< 14% and ≥ 14%). A single pathologist interpreted all IHC results. Breast cancer subtypes were defined as follows: luminal HER2− (ER and/or PR positive, HER2 negative, any Ki-67), luminal HER2+ (HER2 3+ by IHC or amplification by FISH, ER and/or PR positive, any Ki-67), HER2+ type (HER2 3+ by IHC or amplification by FISH, ER and PR negative), and TNBC type (ER and PR negative and HER2 negative). In this study, total pCR was defined as the absence of invasive carcinoma in both the breast tissue and LNs after NAC. Breast pCR was defined as the absence of invasive carcinoma in the breast regardless of the axillary response. Finally, axillary pCR was defined as the absence of invasive carcinoma in the axilla regardless of the breast response.
Statistical analysis
The primary endpoints in the present study were the tumor response and BCS conversion rates according to the breast histological subtype. The secondary endpoints were the clinicopathological factors associated with higher tumor response rate in luminal HER2− breast cancer. Differences between groups were assessed using the chi-square or Fisher's exact tests for categorical variables. Summary statistics are presented as number (%) for categorical variables and median (interquartile range) for continuous variables. We conducted simple and multivariate logistic regression models. Variables with statistical significance (p < 0.05) in the univariate analysis were included as covariates in the multivariate analysis. These were then used to analyze the relationship and estimate the odds ratios (ORs) and 95% confidence intervals (CIs) between covariates. All results were analyzed using SAS version 9.4 (SAS Institute, Cary, USA). The p-values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
A total of 311 patients received NAC and subsequently underwent radical surgery at Seoul St. Mary's Hospital between January 2010 and December 2016. After excluding patients, we identified 244 patients with clinically node-positive breast cancer. The study profile is shown in Figure 1. Table 1 shows the clinicopathological characteristics of the 244 patients in our study. Of these patients, 46.3% had clinical T2 tumors, 41.0% had clinical T3 tumors, and 7.4% had clinical T1 tumors. Thirteen patients with clinical T4 tumors were classified as those with inflammatory breast cancer. All 13 patients underwent total mastectomy after NAC. In the 244 patients with breast cancer, the intrinsic molecular subtypes were as follows: luminal HER2− (n = 114 [46.7%]), luminal HER2+ (n = 39 [16.0%]), HER2+ (n = 44 [18.0%]), and TNBC (n = 47 [19.3%]). Overall, total pCR (both breast and axilla), breast pCR, and axilla pCR were achieved in 14.8%, 19.7%, and 32.4% of patients, respectively. The median tumor response rate to NAC was 46.40% (range, −25.8% to 100%) according to the RECIST 1.1 criteria. Before receiving NAC, 178 patients were scheduled for total mastectomy. After receiving NAC, 92 patients (37.7%) underwent BCS, and 152 patients (62.3%) underwent total mastectomy. Twenty-six of 165 patients previously requiring total mastectomy were converted to undergo BCS, excluding 13 patients with inflammatory breast cancer. The BCS conversion rate was 15.8%. No patients previously requiring BCS were converted to undergo total mastectomy. Moreover, there were 3 patients who had improvement after NAC, but BCS was not possible before NAC.
Figure 1
Study profile. A total of 311 patients received NAC and subsequently underwent surgery between January 1, 2010, and December 31, 2016. Of these, 244 patients met the eligibility criteria and were enrolled in this study.
NAC = neoadjuvant chemotherapy; LN = lymph node; HER2 = human epidermal growth factor receptor 2; TNBC = triple-negative breast cancer.

Table 1
Patients characteristics

pCR and BCS conversion rates according to intrinsic molecular subtype
The pCR in the 244 patients according to molecular subtype is summarized in Table 1. The overall, breast, and axillary pCR rates were 7.9%, 12.3%, and 22.8%, respectively, in the subtype of luminal HER2− breast cancer. The patients were subdivided into luminal HER2− and non-luminal HER2− breast cancer groups (luminal HER2+ and HER2+ and TNBC types). The total pCR rate was significantly higher in patients with non-luminal HER2− breast cancers (20.8%) than in those with luminal HER2− breast cancer (7.9%; p < 0.013). The breast pCR rate was significantly higher in patients with non-luminal-type breast cancer (26.2%) than in those with luminal-type breast cancer (12.3%; p = 0.009). The axillary pCR rate was also significantly higher in patients with non-luminal-type breast cancer (40.8%) than in those with luminal-type breast cancer (22.8%; p < 0.013) (Table 2 and Figure 2).
Table 2
Clinical and pathologic features of patients according to intrinsic subtype

Figure 2
pCR rates and BCS conversion rates in neoadjuvant chemotherapy by histologic subtype.
pCR = pathologic complete response; BCS = breast-conserving surgery; HER2 = human epidermal growth factor receptor 2; TNBC = triple-negative breast cancer.
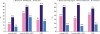
The BCS conversion rate was 16.3% (13 of 80) in luminal HER2− breast cancer. Of the other subtypes, BCS conversion rates were 14.0% (8 of 57) and 17.9% (5 of 28) in luminal HER2+ and HER2+ and TNBC, respectively (Table 1 and Figure 2). The BCS conversion rate did not differ significantly between the luminal HER2− and non-luminal HER2− breast cancer groups (p = 0.836) (Table 2). Using the median tumor response rate (46.4%) as the cutoff value, low tumor response rate was classified as < 46.4% and high tumor response rate as ≥ 46.4%. Tumor response rate also did not differ significantly between the luminal HER2− and non-luminal HER2− breast cancer groups (p = 0.180) (Table 2).
Predictors of BCS conversion
Univariate and multivariate analyses that were used to identify predictive factors of achieving BCS conversion are summarized in Table 3. In the univariate and multivariate logistic regression analyses, patients exhibiting a high tumor response rate (≥ 46.4%) (OR, 6.490; 95% CI, 2.164–19.461; p = 0.001) were significantly associated with an increased probability of BCS conversion. However, the intrinsic breast cancer subtype was not significantly associated with the BCS conversion rate (Table 3).
Table 3
Univariate and multivariate logistic regression analysis of total patients according to the BCS conversion
Factors associated with response and axillary pCR in luminal HER2− breast cancer
Supplementary Table 1 summarizes the patient and tumor characteristics of 114 patients according to the tumor response rate. Higher Ki67 expression and total pCR, breast pCR, axillary pCR, and BCS conversion rates were significantly more common in patients with higher tumor response rates. Table 4 shows the results of the univariate and multivariate analyses performed to identify predictive factors of higher tumor response rate in luminal HER2− breast cancer. In the multivariate analysis, higher Ki67 expression (OR, 2.478; 95% CI, 1.066–5.762; p = 0.035), axilla pCR rate (OR, 3.715; 95% CI, 1.356–10.177; p = 0.011), and BCS conversion rate (OR, 5.793; 95% CI, 1.358–24.708; p = 0.018) were significantly associated with tumor response to NAC. Higher clinical tumor and nodal stage before NAC was not significantly associated with tumor response to NAC (Table 4). Of the 114 patients with luminal HER2− breast cancer, 26 (22.8%) achieved axillary pCR, and 88 (77.2%) exhibited residual axillary disease after NAC. The multivariate analysis using axillary pCR after NAC as the dependent variable demonstrated that a higher tumor response rate (≥ 46.4%) was an independent predictive factor for achieving axillary pCR (OR, 3.395; 95% CI, 1.300–8.868; p = 0.013; Supplementary Table 2).
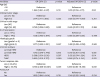
Table 4
Univariate and multivariate logistic regression analysis of luminal HER2− breast cancer according to the tumor response rate

DISCUSSION
NAC is the standard treatment of choice for patients with locally advanced and inflammatory breast cancer. NAC may improve the rate of BCS conversion by reducing the size of the tumor, and the cosmetic effect can be achieved by reducing the resection range. It can also reduce axillary LN metastasis to avoid axillary LN dissection [123]. Therefore, it is effective in improving the quality of life. However, the prognosis and responses to NAC differ according to the molecular subtype of breast cancer. Patients with luminal HER2− breast cancer generally show good long-term outcomes, whereas those with HER2 and TNBC breast cancer have poor outcomes [15]. Despite the favorable long-term outcome, luminal HER2− breast cancer is relatively resistant to NAC. Previous studies have reported that luminal HER2− breast cancer has a significantly lower clinical and pathological response relative to HER2+ and TNBC types and suggested that luminal HER2− breast cancer has a poorer response to NAC than the other subtypes [151617]. The pCR rate in patients with luminal HER2− breast cancer was only 9% in a previous study [18]. Our results also revealed a low pCR rate (7.9%). Therefore, the use of NAC in luminal-type breast cancer has been questioned. Recent studies have demonstrated that NET was more effective in allowing breast conservation than NAC by decreasing the size or extent of the tumor, with fewer unnecessary chemotherapy-induced toxicities [111920].
Several studies have reported that pCR after NAC is associated with improved outcomes compared with absence of pCR. Therefore, pCR has become a major focus and the most commonly used prognostic marker in studies on NAC [621]. However, pCR is not the only aim of NAC. In luminal HER2− breast cancer, pCR is less likely to occur, and patients with this tumor type do not demonstrate a correlation between good long-term outcomes and pCR observed in HER2+ and TNBC type breast cancer [7101822]. The main benefit of NAC is reduction in the size of the breast cancer tumor, thus allowing the performance of BCS in patients requiring total mastectomy before NAC. Additionally, NAC can eradicate metastatic axillary LN, thus increasing the possibility of avoiding axillary LN dissection. With improvement in breast cancer survival rates, oncological outcomes are also important in surgical treatment; however, quality of life is also an increasingly important consideration [23].
BCS with radiotherapy provides similar long-term outcomes and better cosmetic effect and quality of life than total mastectomy [24]. The proportion of patients who undergo BCS after NAC varies from 13% to 83%. This broad range is likely due to different patient selection criteria [25]. Our results revealed a 16.3% BCS conversion rate in luminal HER2− breast cancer, with no significant difference from the rates in other subtypes. In our study, axillary LN metastasis was confirmed in all patients before NAC using core needle biopsy of axillary LN before the patients underwent axillary LN dissection. However, NAC also affects the eradication of metastatic axillary LNs. Many studies have reported sentinel LN biopsy after NAC in patients with axillary LN metastasis breast cancer [2627]. Our results demonstrated an axillary pCR rate of 22.8% in luminal HER2− breast cancer. Although this value is low, nevertheless, it highlights a significant difference compared with those in other subtypes, and they are expected to improve the conservation rate of axillary LN after NAC in luminal HER2− breast cancer and avoid complications of axillary LN dissection such as lymphedema, arm pain, and reduced arm movement [28].
In our study, the BCS conversion rate was lower than those reported in other studies [11], and there may be bias in determining BCS conversion after NAC. Therefore, we conducted a more objective analysis by measuring the tumor response rate of each breast cancer subtype to evaluate the benefit of chemotherapy in luminal HER2− breast cancer. A high tumor response rate (≥ 46.4%) (OR, 6.490; 95% CI, 2.164–19.461; p = 0.001) were significantly associated with an increased probability of BCS conversion. Moreover, tumor response rate did not differ significantly between the luminal HER2− and non-luminal HER2− breast cancer groups (p = 0.180). Therefore, the low pCR rate in patients with luminal-type breast cancer does not consistently result in lower BCS conversion and tumor response rates after NAC compared to those in patients with other breast cancer subtypes. Our results demonstrated a significant tumor response following NAC in patients with luminal HER2− breast cancer; thus, NAC can preserve the breast in luminal HER2− breast cancer compared with other subtypes. NAC is also expected to improve cosmetic outcomes in patients scheduled for BCS before NAC by reducing the excision range.
It is important to identify patients with luminal HER2− breast cancer in whom NAC may provide significant benefits. Our subgroup analysis of patients with luminal HER2− breast cancer demonstrated that high Ki-67 expression was a significant independent factor associated with a higher tumor response rate (≥ 46.4%) in the multivariate analysis. Therefore, we demonstrated a positive relationship between Ki67 expression and tumor response rate in luminal HER2− breast cancer. High Ki67 expression in luminal HER2− breast cancer was significantly associated with improved tumor response rates.
Our study had several limitations. First, it has a single-center, retrospective design. It was not always possible to determine whether a patient would be a candidate for BCS or total mastectomy before and after NAC. Therefore, our study could not rule out the possibility of selection bias. Second, we did not include trastuzumab in the NAC regimen of some patients with HER2+ breast cancer. Third, our study did not include treatment with pertuzumab, which has a significant effect on the pCR of patients with HER2+ breast cancer. Lastly, sentinel LN biopsy could be performed to assess axillary nodal status in patients with axillary pCR after NAC; however, our study performed axillary LN dissection in all patients. Despite these limitations, the strength of our analysis was the assessment of the tumor response rate, which was evaluated relatively accurately using breast MRI after NAC. Furthermore, the patient groups were less heterogeneous because the same treatment was administered at a single institution.
Therefore, the indications for NAC in luminal HER2− breast cancer remain unclear, and as such, controversy regarding the effectiveness of NAC persists. Our results demonstrated similar tumor response and BCS conversion rates after NAC, especially in patients with clinically node-positive luminal HER2− breast cancer. A low pCR rate alone is not a sufficient reason to hesitate performing NAC in patients with luminal HER2− breast cancer. NAC still provides a potential benefit of reduction in tumor extent for these patients.
 XML Download
XML Download