

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The consensus on the optimal duration of endocrine therapy for non-metastatic, hormone receptor-positive breast cancer has been undergoing adjustment and is now a 5-year minimum for tamoxifen or aromatase inhibitor (AI) treatment. Extended therapy for more than 5 years can be an option for all patients with breast cancer with positive hormone receptor, but some may benefit more than others. Data from the National Cancer Institute of Canada Clinical Trials Group MA.17 trial support an improvement in disease-free survival (DFS) and overall survival (OS) with the extended use of letrozole following a 5-year completion of tamoxifen therapy for postmenopausal patients [123]. The Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) and adjuvant Tamoxifen—To offer more? (aTTOm) trials, which evaluated the efficacy of continuing tamoxifen for up to 10 years, reported a significant reduction in the risk of recurrence and breast cancer mortality [45]. With regard to extended therapy in AI-treated women, prior results conflict with the findings of the MA.17R trial that reported an improvement in DFS and a decreased incidence of contralateral breast cancer, but there were no benefits in terms of OS [6].
In women with hormone receptor-positive breast cancer, recurrences are well known to continue to occur steadily for up to 15 years after completing a scheduled 5-year endocrine therapy and decrease by extending such therapy beyond 5 years [7]. However, when selecting the patients who will receive extended therapy, potential toxicities caused by prolonged endocrine therapy must be considered. In the ATLAS trial, extended tamoxifen therapy increased the incidence of endometrial cancer by 84% (number of events = 116 vs. 63, 10 years vs. 5 years) and pulmonary embolus by 95% (number of events = 41 vs. 21, 10 years vs. 5 years), although the number of associated death events was not different [4]. A prior meta-analysis on the toxicity profile of extended AI revealed an increased risk of cardiovascular events and bone fracture [8]. Other common side effects associated with tamoxifen or AI treatment, which are not life-threatening but bothersome, include hot flashes, vaginal dryness, and sexual dysfunction. These side effects have the potential to greatly impair the quality of life in long-term survivors who carry a lower risk of recurrence and consequently are expected to gain minimal benefit from an extended endocrine therapy regimen. Hence, decisions to proceed with these extended treatments must be made with careful and detailed consideration of the original prognosis of the tumor, reports of ongoing side effects by the patient, and potential for toxicity from prolonged endocrine treatment.
The recently updated guidelines by American Society of Clinical Oncology (ASCO) state that the benefits of extended endocrine therapy in breast cancer survivors in terms of decreasing the absolute risk of recurrence are modest and that an individualized approach to treatment duration that is based on considerations of risk reduction and tolerability is appropriate for lower-risk node-negative or limited node-positive breast cancers [9]. However, it must be noted that current practices lack more sophisticated prognostic factors by which the risk of late events can be estimated and accordingly evidence-based recommendations regarding extended endocrine therapy can be made. This study aimed to identify such prognostic factors for breast cancer-specific mortality in patients with hormone receptor-positive breast cancer who have completed 5 years of tamoxifen treatment and remained disease free. Additionally, it aimed to categorize subgroups based on breast cancer-specific death risks determined by the presence or absence of combinations of the abovementioned prognostic factors. This was intended to assist with the clinical decision-making on prolonged endocrine therapy in breast cancer.
METHODS
Patients with breast cancer who underwent surgery followed by adjuvant tamoxifen treatment for stage I–III hormone receptor-positive tumors at Asan Medical Center between January 1999 and December 2008 (other than patients with bilateral cancer or with an initial plan for neoadjuvant systemic therapy) and had been followed successfully in the initial 5 years without any recurrences were initially enrolled (n = 3,706). Patients receiving extended AI treatment that started in 2015 at our institution were excluded from further analysis (n = 548). Thus, the final study cohort comprised 3,158 patients who had been scheduled to receive 5 years of endocrine therapy with tamoxifen.
All patient information and tumor characteristics were retrieved from our prospectively collected database. The size of the tumor, lymph node (LN) status, histologic grade, nuclear grade, presence of lymphovascular invasion (LVI), and immunohistochemical (IHC) status of the estrogen receptors (ERs), progesterone receptors (PRs), human epidermal growth factor receptor 2 (HER2), and mutant p53 were determined at our institution by pathological analysis of formalin-fixed paraffin-embedded tissue sections of the primary tumor excised at the time of definitive surgery. ER or PR positivity was defined as nuclear staining ≥ 1% or by an Allred score ranging from 3 to 8 based on IHC staining. The hormone receptor status was determined as positive in cases of ER positivity and/or PR positivity and negative in cases of both ER and PR negativity. For HER2, the results were graded according to the level of staining of the cancer cell membranes. A result was defined as positive (3+) when the tumor showed uniform, intense membrane staining in more than 30% of the invasive tumor cells. An equivocal (2+) result was defined as the presence of weak or nonuniform membrane staining in more than 10% of the tumor cells. A negative result was defined as the presence of weak/incomplete membrane staining (1+) or the complete absence of membrane staining (0) in any portion of the tumor cells. Because fluorescence in situ hybridization (FISH) was not used in the current study period, tumors graded 2+ were considered HER2 negative. This study was reviewed and approved by the Institutional Review Board of Asan Medical Center (2017-1341). Informed consent was waived because the study design was based on retrospective clinical data.
Two periods of diagnosis, 1989–2003 and 2004–2008, were considered in the analysis because each showed a different availability of systemic agents for the treatment of breast cancer. The former period (1989–2002) is representative of an era in which doxorubicin and cyclophosphamide (AC) regimens were not available, and cyclophosphamide, methotrexate, and fluorouracil (CMF) regimens were used for chemotherapy in many breast cancer cases. Moreover, gonadotropin-releasing hormone agonist or AIs were not used in endocrine therapy before 2003.
In our present study, breast cancer-specific survival (BCSS) was calculated only in patients who were successfully followed for 5 years with no evidence of recurrence. Patients who died of any reason within the initial 5 years post-diagnosis were also excluded. Any death resulting from breast cancer at more than 5 years post-diagnosis was designated as a late death event in this study. Hence, BCSS after 5 years of tamoxifen therapy was defined as the time from the 5-year follow-up to the first incidence of death from breast cancer. Survival curves were generated using the Kaplan-Meier method, and the significance of survival differences among selected factors was verified using the log-rank test. The Cox proportional hazards model was used to evaluate independent prognostic effects on BCSS. Unless stated otherwise, the data are presented as mean ± standard deviation, and statistical significance was set at a p-value < 0.05. All statistical analyses were performed using SPSS version 21.0 (IBM Inc., Armonk, USA)
RESULTS
Characteristics of patients with breast cancer at the time of diagnosis
The age at diagnosis of the entire study cohort (n = 3,158 patients) was 46 ± 9 years (range, 19–82 years), and the numbers of patients with initial stage I, II, and III were 1,488 (47.1%), 1,381 (43.7%), and 289 (9.2%), respectively. ER and PR positivities were detected in 2,902 (91.9%) and 2,626 (83.2%) patients, respectively. Endocrine treatment was performed with tamoxifen in all patients, among which 486 patients (15.4%) received additional ovarian function suppression therapy. A positive HER2 status was found in 620 patients (19.9%), none of which received anti-HER2 therapy during the study period. Following definitive surgery in 1,462 patients who underwent breast conserving surgery (46.3%) and 1,694 patients who underwent total mastectomy (53.7%) in our present study, 1,769 patients (56.3%) received adjuvant chemotherapy. Patient characteristics are summarized in Table 1.
Table 1
Characteristics of the 3,158 study patients who completed a 5-year scheduled tamoxifen treatment regimen

Data shown are number (%) not otherwise specified.
SD = standard deviation; LN = lymph node; LVI = lymphovascular invasion; ER = estrogen receptor; PR = progesterone receptor; HER2 = human epidermal growth factor receptor 2; BCS = breast-conserving surgery; RT = radiotherapy; CT = chemotherapy; CMF = cyclophosphamide, methotrexate, and fluorouracil; ET = endocrine therapy; SERM = selective estrogen receptor modulator; OFS = ovarian function suppression.
Prognostic factors in predicting breast cancer-specific death beyond 5 years
The median follow-up duration from completion of a 5-year tamoxifen regimen was 81 months (range, 0–179 months). The additional 5- and 10-year BCSS rates were 97.9% and 93.9%, respectively, for the entire study population. Unfavorable survival rates were observed in the subgroups with a < 40 or ≥ 60 years of age (vs. 40 to 59 years of age, p < 0.001), tumor size > 2 cm (vs. ≤ 2 cm, p < 0.001), positive LN metastasis (vs. negative, p < 0.001), grade 2/3 tumor (vs. grade 1, p = 0.003), positive LVI (vs. negative, p < 0.001), and PR negativity (vs. PR positivity, p = 0.021), who received chemotherapy (vs. did not receive, p < 0.001), and with the diagnostic period from 1999 to 2003 (vs. 2004 to 2008, p = 0.016) (Figure 1). The Cox proportional hazards model analysis presented in Table 2 suggested that an age extreme at diagnosis (i.e., < 40 or ≥ 60 years), tumor size > 2 cm, and positive LVI were robust independent prognostic factors for late breast cancer-specific death in tamoxifen-treated patients (hazard ratio [HR] = 2.162, 1.739, and 1.993; p = 0.001, 0.047, and 0.011, respectively). LN metastasis and PR negativity had borderline significance (HR = 1.741 and 1.638; p = 0.099 and 0.061, respectively) in this regard, whereas the other variables, including grade, chemotherapy, and year of diagnosis, were not significant after adjustment.
Figure 1
BCSS after 5 years of scheduled tamoxifen treatment by (A) age at diagnosis, age extreme vs. middle aged; (B) tumor size, > 2 vs. ≤ 2 cm; (C) nodal status, positive vs. negative; (D) tumor grade, grade 1 vs. grade 2/3; (E) LVI, positive vs. negative; (F) PR expression, positive vs. negative; (G) CT, yes vs. no; and (H) year of diagnosis, 1999–2003 vs. 2004–2008. (A-H) All factors were found to be significant predictors for BCSS by univariate survival analyses.
BCSS = breast cancer-specific survival; LVI = lymphovascular invasion; PR = progesterone receptor; CT = chemotherapy.

Table 2
Cox proportional hazards regression model for BCSS after 5 years of tamoxifen therapy
BCSS = breast cancer-specific survival; HR = hazard ratio; CI = confidence interval; LN = lymph node; LVI = lymphovascular invasion; PR = progesterone receptor; CT = chemotherapy.
*HRs generated from a Cox proportional hazard model with adjustment for the eight indicated variables in the table; †Five factors considered to be possible classifiers for the risk stratification system.
Risk stratification system for groups with a low, intermediate, high, and extremely high risk of mortality at 5 years or more post-diagnosis
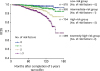
We constructed a risk stratification system using 5 risk factors associated with late breast cancer-specific mortality, i.e., an age extreme at diagnosis, tumor size > 2 cm, positive LVI, LN metastasis, and PR negativity. We then classified all 3,158 study patients into four subgroups according to the number of risk factors as follows: low-, intermediate-, high-, and extremely high-risk groups that had 0, 1, 2, and 3 or more risk factors, respectively. As shown in Figure 2, the BCSS rates significantly differed between these groups. A greater number of risk factors was associated with a poorer BCSS (HR = 2.054, 4.425, and 8.438 for 1, 2, and 3 or more risk factors, respectively) and shorter OS (data not shown). From 5 years post-diagnosis, the additional 5- and 10-year cumulative risks of breast cancer-specific death in each risk group were as follows: 0.8% and 1.5% in the low-risk group, 0.9% and 3.9% in the intermediate-risk group, 1.3% and 7.3% in the high-risk group, and 4.8% and 13.8% in the extremely high-risk group, respectively.
Figure 2
BCSS after 5 years of scheduled tamoxifen treatment in subgroups classified using the risk stratification system. The low, intermediate, high, and extremely high-risk groups had 0, 1, 2, and 3 or more predictors, respectively, among variables including age extreme at diagnosis, tumor size > 2 cm, positive LVI, LN metastasis, and PR negativity.
BCSS = breast cancer-specific survival; LVI = lymphovascular invasion; LN = lymph node; PR = progesterone.
DISCUSSION
In the present study, we found that there are significant prognostic indicators of the risk of late breast cancer-specific death after 5 years of tamoxifen treatment for hormone receptor positive tumors. These include an age extreme at diagnosis (much younger or much older), tumor size > 2 cm, positive LVI, LN metastasis, and PR negativity (Table 2). Patients showing a greater number of these risk factors can therefore be selected for extended endocrine therapy because they are predicted to have a higher risk of a late death event. This will in turn lead to greater benefits from these extended treatments.
The clinicopathological factors that have the most consistently reported association with a high risk of cancer-specific mortality are a positive LN and greater tumor size. LN metastasis is the best predictor of an early recurrence in the hormone receptor positive subgroup of breast cancer, along with a high tumor grade, low ER or PR expression, and high Ki67 index, which may represent disease burden, proliferation rate, and consequently a relative aggressiveness of this otherwise favorable subtype [101112]. Because tumors with such aggressive features can cause early recurrence (i.e., within 5 years), the prognostic roles of these factors as predictors for late recurrence can be weakened or sometimes reversed during the period beyond 5 years. Nevertheless, the nodal status has persistently been almost the sole independent predictor for late recurrence across several studies [713141516]. After multivariate adjustment, five variables associated with late breast cancer-specific mortality were observed in our current study and enabled us to devise a new risk stratification system. In terms of tumor burden, tumor size > 2 cm (HR = 1.739; p = 0.047), LN metastasis (HR = 1.741; p = 0.099), and positive LVI (HR = 1.993; p = 0.011) could be regarded as candidate risk classifiers, as reported in other studies [161718]. With respect to tumor proliferation, PR negativity (HR = 1.638; p = 0.061) showed potential as a risk classifier but neither the tumor grade nor HER2 overexpression status had a significant association with recurrence after adjustment (Table 2).
It was interesting that an age extreme, i.e., younger (< 40 years) or older (≥ 60 years) age, was found to be the most powerful independent predictor of late-occurring breast cancer-specific death (HR = 2.162; p = 0.001). A possible explanation for this is that a considerably younger or older age bracket is a risk factor for non-adherence to adjuvant endocrine therapy [192021]. The precise reasons may be somewhat more complex than this, but women in the age extreme as defined herein have been reported previously to have a higher association with non-adherence risk factors such as endocrine therapy-related side effects or depression compared to middle-aged women [2223]. Although it is beyond the scope of this study, another clinical implication of this finding may be that the adherence level in the initial 5 years needs to be carefully checked in women aged < 40 or > 60 years when making decisions on whether longer endocrine therapy can be successfully completed.
A plausible explanation for a poorer long-term prognosis in younger women with hormone receptor positive breast cancer is that the tumors that develop in this age group are more likely to express high-proliferation molecular markers, which can cause aggressiveness [101112]. In the case of older women, under-treatment could be an explanation [2425]. In our present study, women aged ≥ 60 years received chemotherapy less frequently compared to the other age groups. The percentages of patients in our cohort who received chemotherapy in the < 40 years, 40–59 years, and ≥ 60 years subgroups were 45.5%, 33.6%, and 11.7%, respectively, for the negative LN status cases (p < 0.001), and 98.7%, 96.8%, and 68.2%, respectively, for the positive LN status cases (p < 0.001). In the present study, the age extreme variable remained a significant predictor of late mortality after adjustment with conventional prognostic variables and was thus incorporated into our risk stratification system.
Categorizing subgroups based on the risk of breast cancer-specific mortality could be clinically useful when decision-making is required regarding possible prolonged endocrine therapy. Dowsett et al. [26] previously described a simple prognostic tool (Clinical Treatment Score post-5 year; CTS5) which integrated four clinical variables, including nodal status, tumor size, tumor grade, and age, for predicting late breast cancer recurrence. Notably, however, the variables in our current risk stratification system are binary, whereas those in the CTS5 are continuous or ordinal. Despite the relative weaknesses of our system in terms of the detailed estimation, we believe that it can be used as reliably and practically as the CTS5 because real-world clinical decisions will be based on an arbitrary cutoff that separates patients into two groups only: patients continuing endocrine therapy and those who cease receiving this treatment after 5 years.
For candidate patients for extended endocrine therapy who completed 5 years of tamoxifen treatment and were recurrence-free at that point, there are two management options that clinicians commonly consider, i.e., extending tamoxifen beyond 5 years or using an AI following tamoxifen treatment. If our risk stratification system is applied to this decision-making, previous studies need to be taken into account in terms of the absolute survival benefits rather than the relative survival benefits of extending the endocrine therapy.
Two large trials, ATLAS [4] and aTTom [5], have demonstrated that continuing tamoxifen for up to 10 years is more effective with respect to DFS and OS than discontinuing this therapy at 5 years after diagnosis. The experimental arm in ATLAS, which randomized 15,244 women into 10- versus 5-year tamoxifen groups, showed a significant reduction in the recurrence risk at 5–14 years by 3.7% (21.4% for women allocated to continued treatment versus 25.1% for controls, p = 0.002) and in breast cancer-specific mortality by 2.8% (12.2% for women allocated to continued therapy versus 15.0% for controls, p = 0.01) [4]. Similarly, an approximately 3% absolute risk reduction was reported in the aTTom trial [5]. However, it should be noted that a 3% absolute risk reduction is too modest to apply tamoxifen extension to all women with hormone receptor positive breast cancer. Moreover, the absolute increase in the cumulative incidence and mortality of endometrial cancer at 5–14 years was in no way negligible in the ATLAS trial (3.1% and 0.4% for women receiving continued treatment versus 1.6% and 0.2% for the controls) [4]. In this regard, the authors of the ATLAS trial revealed that the clinical benefits of a 10-year tamoxifen regimen are particularly relevant to premenopausal women with continued ovarian activity among whom there is low risk of tamoxifen causing uterine cancer or vascular side effects that would negate the absolute reduction in breast cancer mortality [4]. In our risk stratification system, the 10-year breast cancer-specific mortality rates of the low- and intermediate-risk groups were approximately 1.5% and 3.9%, respectively, suggesting that little additional benefit would be gained from a tamoxifen treatment extension in patients in these risk groups.
The absolute benefits and adverse effects of an AI extension were analyzed in the previous MA.17 trial, which was the first large-scale randomized trial of letrozole for an additional 5 years after the initial 5-year tamoxifen treatment of postmenopausal women with hormone receptor positive early breast cancer. Regardless of the nodal status, the distant metastasis-free survival rates for the following 4 years were 96.6% for the AI extension group and 93.7% for the control group (absolute difference, 2.9%) [12]. However, the MA.17 trial reported that osteoporosis was significantly more frequent in the AI extension group (8.1% vs 6.0%, p = 0.003) [12]. In terms of the more severe osteoporotic fracture complication, the reported results are conflicting, with no difference in incidence found with letrozole [2] and a significantly increased risk of fractures with anastrozole in the Austrian Breast and Colorectal Cancer Study Group (ABCSG)-16 trial [27]. A finding from a previous meta-analysis of seven trials including 16,349 women receiving an AI treatment extension is worthy of consideration in this regard [8]. The authors reported a statistically insignificant increase in non-breast cancer-related mortalities, which may have masked any cancer-specific survival benefits of using AI extension therapy and led to a similar OS outcome between the two groups [828]. We believe that the more granular subgrouping with our five clinicopathological prognostic factors that are associated with the risk of breast cancer-specific mortality could also be a practical aid for clinicians in deciding on the use of an AI extension approach, given that the incidence of fatal AI-related complications remains controversial.
The findings of this present study had some limitations. First, an IHC assay of Ki-67 was not routinely performed at our institution in the study period. Longer follow-up periods are needed to assess the effect of Ki-67 on late breast cancer-specific mortality, and a future risk stratification system into which Ki-67 is incorporated may have a more precise prediction capability. Second, as adjuvant trastuzumab therapy has been covered by the Korean National Health Insurance since 2009, anti-HER2 therapy was not used in the majority of our patients. Hence, the survival outcomes in the present cohort may be out of date as anti-HER2 therapy would have been administered to > 19.9% of these patients if the current practice guidelines had been followed. Moreover, tumors with equivocal IHC HER2 expression patterns were not reexamined for gene amplification by FISH, and only cases graded 3+ were considered to be HER2 positive, as mentioned in our Methods section. However, it is notable that HER2 overexpression has an insignificant prognostic impact on late breast cancer-specific mortality in trastuzumab-naïve patients with breast cancer. Third, patients receiving neoadjuvant chemotherapy were excluded from our cohort. Therefore, the application of our risk stratification system to patients without neoadjuvant chemotherapy only would be reasonable considering that the ambiguous prognostic role of the anatomical or biological responses of these less aggressive tumors to neoadjuvant chemotherapy could confuse the shared decision-making with regard to predicting late mortality [2930]. Finally, we analyzed the Korean population only, which is a limitation in terms of generalization. However, we believe that our study still has unique value as it highlights that fact that the prognosis of the long-term tamoxifen-treated patients may depend on the level of medication adherence, and this is known to vary according to cultural or ethnical backgrounds.
We conclude that our newly described risk stratification system for late mortality in breast cancer can be used to resolve some of the current controversies on how to identify candidates for extended endocrine therapy after 5 years of tamoxifen treatment. Moreover, the application of this system is practicable because the five clinical factors are automatically generated and easy to access in most clinical settings without any additional costs and using current standard clinical management and pathological tests. Therefore, in circumstances where expensive molecular assay scores for this purpose are not available, this system will have significant utility in helping clinicians decide whether to continue endocrine therapy for up to 10 years.
 XML Download
XML Download