

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In 2040, more than two million dementia cases are expected in Korea.1 The current rates of increase for dementia are estimated to be 3-fold higher in Asia compared to those in developed countries,2 which are mainly due to the rapid increase of the aged population in Asian countries. Korea is one of the countries with the fastest-growing aging population; it has taken only 17 years to move from an ‘aging society’ to an ‘aged-society.’3
Meanwhile, recent studies conducted in Western countries have reported declining trends for dementia incidence and suggested that improvements in living conditions, education, and healthcare may have reduced the risk of dementia.45678910 In contrast, increasing trends of dementia incidence were noted in China and Japan, even though their follow-up intervals and the reported incidence rates were very different. A Chinese study showed a 1.73-fold increase over a decade, with incidence rates of 9.0 cases per 1,000 person-years (PY) in 1999, while a Japanese study reported a 1.68-fold increase over three decades, with incidence rates of 41.6 cases per 1,000 PY in 2012.1112 No study has investigated the time trends of dementia incidence in Korea. One study reported the trends of dementia prevalence in Korea by comparison of previous epidemiologic studies conducted in different areas. Although it noted only a slight increase after 2005, from 7.3% to 8.7% (without significance), it predicted a large increase of dementia prevalence in Korea due to the enormous aging population.13 The increasing number of older people is the most potent driving factor of the dementia epidemic. However, there have also been recent changes in educational level, lifestyle, and health conditions in older Korean adults that may have influenced the risk of dementia during recent decades. Therefore, we should estimate the future prevalence of dementia based on the changeable incidence over time.
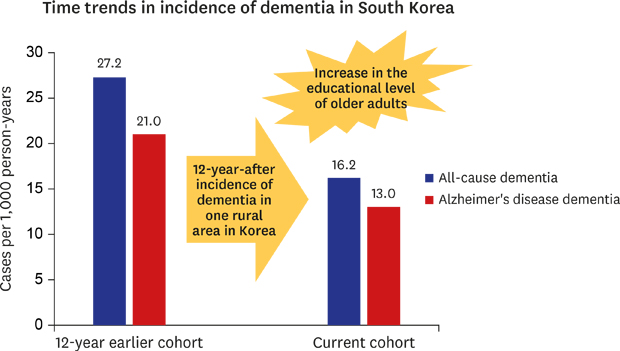
There have been two previous studies on dementia incidence in Korea: a nationwide study and a community-based study.14151617 The latter was conducted in Yeoncheon, a rural area in Korea, in which baseline assessment was conducted in 1996 in adults aged 65 years and older (n = 1,035). Subjects were followed up with a 5.4-year period, and the incidence rates of all-cause and Alzheimer's disease (AD) dementia were reported as 27.2 cases (95% confidence interval [CI], 22.3–33.2) and 21.0 cases (95% CI, 16.5–26.4) per 1,000 PY, respectively.1516 Yeoncheon is a small rural area in Korea with a current population of 43,990.3 Because all administrative areas in Yeoncheon are designated as a military protected zone due to its location adjacent to North Korea, the migration rates have been low, even compared to other rural areas.3
In the current study, we again investigated the incidence of dementia by an independent elderly cohort in Yeoncheon. Even though our community-based cohort is not representative of the elderly Korean population, it could be advantageous to compare the separate cohorts in this area, to investigate the time trends of dementia incidence and its correlates. There were two goals in the present study: we aimed to report the incidence rates and correlates of all-cause and AD dementia based on our later cohort study and to compare our results with those of an earlier cohort study to investigate the changes of dementia incidence over 12 years.
METHODS
Data collection and study population
Baseline assessments were conducted in 2008 on a target population of all eligible residents aged 65 years or older living in Yeoncheon county. A multi-stage, stratified, cluster sampling method was used to select study samples based on population census data from 2005.18 Of the 1,038 eligible subjects, 72.4% (n = 751) responded to the door-to-door interview, and subjects diagnosed with dementia (n = 50) at baseline were excluded from our analyses. Therefore, a total of 701 non-demented subjects were included in the study at baseline. There were two schedules for the follow-up: the first was in 2009–2010, and the second was in 2013–2014 (Fig. 1). The 1-year follow-up did not aim to include all participants: all subjects diagnosed with mild cognitive impairment (MCI) at baseline (n = 89) and one half of cognitively normal adults (randomly selected, n = 236) were subjected to follow-up. However, all subjects without dementia at baseline (n = 701) were supposed to participate in the 5-year follow-up. The same interview tools and diagnostic criteria were employed throughout the course of the follow-up studies.
Fig. 1
Flowchart of recruitment, participation, and follow-up.
a1-year follow-up was aimed to include only 325 subjects for the target sample: all MCI (n = 89) and randomly selected half of the CN adults (n = 236) were subject to follow-up; among them, 256 (78.8%) were followed-up at 1-year assessment.

Measurements
Cognitive diagnoses were determined by a two-stage process: 1) trained interviewers screened the subjects using the Korean version of the Mini-Mental State Examination (MMSE-KC) from the Korean version of the Consortium to Establish a Registry for Alzheimer's Disease (CERAD-K) assessment battery,19 and 2) individuals with an age-, gender-, and educational year-adjusted z-score of MMSE-KC under −1.5 standard deviations were evaluated for dementia by a psychiatrist using semi-structured interviews, and a clinical psychologist performed neuropsychological tests; both were based on the CERAD-K.1920 Final diagnosis was based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for dementia21 and the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS)–Alzheimer's Disease and Related Disorders Association (ADRDA) for AD dementia.22 MCI was determined by the consensus criteria from the International Working Group on MCI23: 1) cognitive decline by self and/or informant, 2) impairment on objective cognitive tasks, 3) preserved basic activities of daily living and minimal impairment in complex instrumental functions, and 4) not demented.
Sociodemographic characteristics, including age, gender, years of education, marital status, employment status, and the type of medical insurance, were collected via interview. Alcohol intake and smoking was questioned based on habits during the past year. Alcohol intake was divided into minimal and moderate or greater intake. Subjects were dichotomized into non-smokers and current smokers who smoked within the past year. Physical activity was assessed using a modified Korean version of the International Physical Activity Questionnaire, short form.24 Information regarding chronic medical illness was assessed by asking whether subjects had ever been diagnosed with any of the following diseases: hypertension, diabetes, dyslipidemia, and cerebrovascular attack or heart disease. Family members confirmed the diagnoses of chronic medical illness to minimize recall bias. A lifetime history of head trauma was also questioned. Lastly, the Korean version of the Geriatric Depression Scale-Short Form (SGDS-K) was used to evaluate depressive symptoms: a cut-off score of 8 was used to define depression.25
Statistical analysis
Baseline characteristics of participants were compared according to follow-up status (at least one follow-up, lost to follow-up, and deceased) using the analysis of variance for continuous variables and the χ2 test for categorical variables.
Incidence rates of all-cause and AD dementia were calculated as cases per 1,000 PY. Person-years for subjects at risk of incident dementia were calculated as the time between baseline and follow-up assessment, and the midpoint of this interval was used for those who developed dementia due to difficulties in assessing the accurate time for dementia onset. The distributions of age, gender, and educational attainment among incident dementia cases are indicated with 95% CIs calculated using a Poisson distribution. Incidence rates in subjects with baseline MCI (n = 89) were also calculated and then compared with those in age-, gender-, educational year-matched cognitively normal adults.
Cox proportional hazard regression models were used to determine whether baseline sociodemographic, lifestyle, and clinical variables were associated with the risk of all-cause and AD dementia. The effects of individual variables were examined in univariate models. Next, two multivariate models were tested: 1) those that included all variables in univariate models (Model 1), and 2) those with only significant variables in univariate analyses with a P value < 0.10 and then sequentially removed using a backward elimination method (Model 2). Results are presented as hazard ratios (HRs) with 95% CIs. All statistical analyses were performed using SPSS Statistics version 25 (IBM, Chicago, IL, USA). Two-sided tests were performed, and P < 0.05 was considered to indicate significance.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. 1307-109-506). All participants were fully informed regarding the aims and methods of the study before interviews, and informed consent was obtained before participation.
RESULTS
Of the 701 older adults without dementia at baseline, 483 (68.9%) had at least one follow-up within study periods; 72 (10.3%) had died and 146 (20.8%) were lost (unable to respond due to severe illness, impossible to contact, or refused to participate) (Fig. 1). The average follow-up period was 5.4 years. We compared baseline sociodemographic, lifestyle, and clinical characteristics of participants according to follow-up status (Table 1). Subjects who were followed up had a mean age of 71.7 ± 5.4 years at baseline and 59.2% were women. The deceased adults had a higher mean age (77.7 ± 7.4 years) compared to the followed and lost subjects, however, there was no significant difference in the percentage of women among the three groups. Participants who were followed up had a higher education level compared to the deceased and exhibited higher MMSE-KC and lower SGDS-K scores at baseline compared to lost and deceased subjects.
Table 1
Comparison of subjects' baseline characteristics by follow-up status

Data are presented as mean ± standard deviation or number (%).
Wid/Div/Sep/Nev = widowed, divorced, separated, or never married, MMSE-KC = Korean version of the Mini-Mental State Examination, a part of the Consortium to Establish a Registry for Alzheimer's Disease, MCI = mild cognitive impairment, SGDS-K = Korean version of the Geriatric Depression Scale Short Form.
aFollowed up with 1-year and/or 5-year assessments; bincluding subjects who were impossible to contact (n = 57) or impossible to examine due to physical conditions (n = 11) and those who refused to participate in the follow-up interview (n = 78); chealth insurance system for low-income brackets; done or more chronic medical illnesses, including hypertension, diabetes, dyslipidemia, stroke, and/or heart disease.
During the follow-up period, 40 new cases of all-cause dementia (16.2 per 1,000 PY) and 32 new cases of AD dementia (13.0 per 1,000 PY) were identified. Higher incidence rates of all-cause and AD dementia were observed in subjects with older age and no educational attainment, while women showed higher incidence rates for AD dementia than men (Table 2). When we calculated the age-standardized incidence rates of dementia based on the standard population in Korea (2005 mid-year population),18 similar incidence rates were noted (all-cause dementia, 16.8 cases per 1,000 PY; AD dementia, 13.5 cases per 1,000 PY).
Table 2
Incidence rates of all-cause and Alzheimer's disease dementia according to age, gender, and educational level

Among subjects diagnosed with MCI at baseline (n = 89), 13 (14.6%) progressed to dementia, 46 (51.7%) were stationary, and 24 (27.0%) recovered to normal cognition during the follow-up period (dementia conversion rate: 39.8 per 1,000 PY), whereas only three incident dementia cases were detected among age-, gender-, and educational year-matched cognitively normal subjects (n = 89; 9 per 1,000 PY). Baseline MCI increased the risk of all-cause dementia by more than 4-fold (HR, 4.4; 95% CI, 1.3–15.5; P = 0.021).
The crude and adjusted HRs of baseline characteristics for all-cause and AD dementia from Cox regression models are shown in Table 3. Univariate Cox regression analyses revealed that old age, low numbers of years of education, and low baseline MMSE-KC scores increased the risk of all-cause dementia (P < 0.05). The first multivariate Cox regression model, which included all variables tested in univariate models, showed that old age and low baseline MMSE-KC score significantly increased the risk of all-cause dementia (Model 1). Another multivariate Cox regression model (Model 2) included age, years of education, baseline MMSE-KC scores, depression, and physical activity status which were significant in the univariate models (P < 0.10) showed that only a low baseline MMSE-KC score remained as a significant risk factor for the incidence of all-cause dementia (not shown in tables). The same significant results were obtained for AD dementia.
Table 3
Univariate and multivariate Cox proportional hazards model for sociodemographic, lifestyle, and clinical variables as risk factors for the incidence of all-cause dementia

HR = hazard ratio, CI = confidence interval, Wid/Div/Sep/Nev = widowed, divorced, separated, or never-married, MMSE-KC = Korean version of Mini-Mental State Examination.
aAdjusted for age, gender, and educational year (Model 1); bexamined in 1-year or 1-score increments; chealth insurance system for low-income brackets; dhaving one or more chronic medical illnesses, including hypertension, diabetes, dyslipidemia, stroke, and/or heart disease.
*P < 0.001; **P < 0.05.
DISCUSSION
The present study investigated the incidence rates and risk factors for all-cause and AD dementia in older adults living in a rural area in Korea. The incidence rates were reported as 16.2 and 13.0 cases per 1,000 PY for all-cause and AD dementia, respectively. Baseline MCI increased the 5-year incidence of all-cause dementia by more than 4-fold, while old age and low baseline global cognitive function were noted as strong predictors of both all-cause and AD dementia.
A recent study on the incidence of AD dementia that analyzed subsamples of a Korean nationwide study reported similar incidence rates with those in our study. Although much lower incidence rates were estimated for the total subjects (7.9 cases per 1,000 PY), individuals living in rural areas showed comparable incidence rates (12.6 cases per 1,000 PY).17 Older age and low baseline cognitive function were revealed as potent risk factors for developing all-cause and AD dementia, consistent with previous studies.26 Especially, baseline cognitive function was the only variable that remained in all multivariate models (i.e., by scoring 1 point higher in baseline MMSE-KC, the risk of all-cause and AD dementia decreased by 14% and 15%, respectively, after 5 years). Baseline MCI increased the risk of all-cause dementia by 4.4-fold, with a 5-year conversion rate of 14.6%, which is comparable with findings in previous community-based studies.27
Upon comparing our results with those from the earlier cohort study in Yeoncheon,1516 the incidence rates decreased by approximately 40% over 12 years for both all-cause and AD dementia (Supplementary Table 1). This result is consistent with previous studies conducted in Western countries, in which they suggested declined trends of dementia incidence.4678928 We showed an even larger decrease in dementia incidence compared with previous studies: a 25% decrease over 10 years from the Rotterdam study in the Netherlands4; a 27% decrease only in women during a 10-year period in a French study6; a 20% decrease during two decades in a UK study7; and a decline of 44% for three decades in a Framingham study in the United States.8
In contrast, two previous studies from China and Japan reported an increased incidence of dementia and suggested that the different trends may be mainly due to the decrease in the competing risk of premature death.1112 However, though our later cohort also exhibited largely decreased mortality rates (15.1%) compared with those of the earlier cohort (29.3%),29 the declining trends of dementia incidence were noted. Different trends among Asian countries may be due to different study periods; the reference cohorts were recruited in the 1980s for both Chinese and Japanese studies, while the earlier Korean cohort study was conducted in the mid-1990s. Therefore, our results may reflect other societal changes that occurred in the early 2000s rather than the large increase of life expectancy between the 1980s and 1990s in Korea. In addition, our later cohort included less numbers of subjects aged 80 years and older (14.1%) compared with the earlier cohort (17.1%); it could affect our decreasing time trends of incidence of dementia. However, when we adjusted the incidence rates in the earlier and later cohorts with age composition of Korean old-age population based on the census in 2005 and 2015, respectively,1829 the incidence rates still decreased by 22% for all-cause dementia (from 24.3 to 19.0 cases per 1,000 PY), and 19% for AD dementia (from 19.0 to 15.5 cases per 1,000 PY).
What made the incidence of dementia decline over the past 12 years in Korea? Although both cohort studies were conducted in the same rural county, the educational level of the subjects varied widely during these periods. In total, 61.8% of subjects in the earlier cohort had no educational attainment, while 34.8% of samples in the current study had no formal education. Other sociodemographic factors, including age distribution, were comparable between the two cohorts.15 When we compared the age- and gender-specific incidence rates between the earlier and later cohort studies (Supplementary Table 1), declining patterns were observed among each age group (except for 70–74 years) and in both genders; however, the most dramatic changes were detected in age groups over 80 years and in women, which may be related with the greater changes of educational level in those groups. All of the above patterns were similar with regard to the changes in the incidence of AD dementia.
No educational attainment is a strong risk factor for dementia.2630 Education has been suggested as a proxy for cognitive reserve, contributing to toleration of pathologic brain changes caused by aging and neurodegenerative diseases.3132 Previous studies on the time trends of dementia incidence reported that educational level may explain some of the decline in incidence from 6% to 10%.68 A recent review on the trends of dementia prevalence in Korea indicated that approximately 16% of current prevalent dementia can be attributed to illiteracy.33 The proportion of uneducated older persons has decreased steeply, not only in older people living in Yeoncheon but also in the general Korean elderly population (from 44.3% in 2000 to 24.3% in 2017 among older persons aged 60 years and older)3435 and is expected to decrease continuously over the next decades. Therefore, the incidence of dementia in Korea may decline, at least as long as the proportion of uneducated older people reaches a plateau.
Meanwhile, changes in modifiable risk factors for dementia should also be considered when predicting the trends of dementia: a westernized lifestyle and increased metabolic syndrome in Korea can increase dementia incidence.36 Although vascular risk factors were not associated with new-onset dementia in our later cohort study, they should be evaluated using the same measurements in separate cohorts to compare their influence on dementia incidence in a future study.
Although the two cohort studies were not originally designed to investigate changes in incidence rates of dementia, there were several advantages to compare the separate cohorts. First, both studies were conducted in the same rural area, Yeoncheon. Additionally, because this area has low rates of move-in and -outs, we believed we could obtain more reliable data regarding the time trends of dementia incidence, independently of possible confounders. Second, the studies were managed by the same principal investigator, and the sampling methods, follow-up schedule, and data collection procedure completely coincided. Third, both cohorts were followed up for the same mean duration of 5.4 years, and the response rates were also comparable.
Nonetheless, there were several limitations. Different screening tools were used to detect the cognitively impaired subjects (Korean version of the Psychogeriatric Assessment Scale [K-PAS] in the earlier study37; MMSE-KC in the later), even though compensatory procedures to minimize false negatives were included in the second stage of both cohort studies. A lower cut-off score of K-PAS was used to include all possibly impaired subjects in the earlier cohort, and some subjects defined as having normal cognition were randomly included in the second stage for the later cohort. Additionally, the earlier study used DSM-III-R for diagnostic criteria of dementia, while the current study used DSM-IV. However, because the diagnostic sensitivity of DSM-IV for dementia is higher than that of DSM-III-R, in which the requirement of both long-term and short-term memory impairment is included,38 it might be possible that our finding of the declining incidence of dementia is correct.
By comparison with the 12-year distant, two independent cohort studies conducted in the same rural area, we support the declining trend of dementia incidence, and the increase of educational level is suggested as a main driving factor in the case of older Korean adults. Further planned epidemiologic studies using the same measurements of population characteristics, modifiable risk factors, and societal changes related to dementia incidence are needed to confirm our results.
 XML Download
XML Download