

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gastric volvulus (GV) is a rare pathology in pediatric patients. Notably, acute GV in newborns and infants may lead to life-threatening complications. The pathophysiology of GV usually involves a problem with the ligament that supports the gastric structure. Changes in the gastric anatomy or function, or problems with an adjacent organ may result in secondary GV. Congenital diaphragmatic hernia, paraesophageal hernia, and wandering spleen are known secondary causes of GV [123]. Herein, we describe the rare case of a 9-year-old boy with chronic GV following left hemihepatectomy for hepatoblastoma.
CASE REPORT
A 9-year-old boy presented with recurrent abdominal pain, postprandial upper abdominal discomfort and bloating, and episodes of intermittent vomiting of 1 year duration. At 4 months of age, he was diagnosed with hepatoblastoma and underwent open left hemihepatectomy. At the 5 year follow-up, there was no evidence of local recurrence and metastasis. On physical examination, his vital signs and weight were stable. The abdominal examination revealed a postprandially distended upper abdomen with no tenderness, guarding, or rebound tenderness. His bowel sounds were normal. The initial differential diagnosis was gastroesophageal reflux based on his symptoms. He received prokinetic medications for 3 months without improvement.
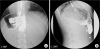
For a confirmatory diagnosis, an upper gastrointestinal contrast study was performed. The Gastrografin swallow study showed that the stomach was rotated along its longitudinal axis, causing delayed gastric emptying (Fig. 1). A final diagnosis of chronic GV was made. Due to persistent abdominal bloating and discomfort, we decided to perform laparoscopic derotation and gastropexy.
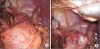
After obtaining the parent's informed consent, pneumoperitoneum was established by an open technique, followed by the placement of three 5 mm trocars. At the time of laparoscopy, the greater curvature of the stomach was attached to the abdominal wall and the left side of the liver. We gently separated the adhesions from the abdominal wall and liver using scissors and a harmonic scalpel (Ethicon Endo-Surgery Inc., Cincinnati, OH, USA) (Fig. 2). No strangulation or stricture of the stomach was observed. The anterior wall of the stomach was anchored to the abdominal wall by an absorbable multifilament suture (Fig. 3). We did not perform fundoplication.
 | Fig. 2(A) Operative finding shows multiple adhesions in the abdominal wall. (B) Operative finding shows greater curvature of stomach attached to the liver.
|
 | Fig. 3Intraoperative views. (A) The completion of adhesiolysis. (B) Anterior wall gastropexy was done with absorbable suture.
|
The patient was discharged on postoperative day 10, and his postoperative course was uneventful. He has not shown signs of postprandial abdominal distension 2 years postoperatively.
DISCUSSION
The stomach has four ligaments (the gastrocolic, gastrohepatic, gastrophrenic, and gastrosplenic ligaments) that anchor it to the peritoneal cavity; any disruption in this anatomic environment may induce GV [4]. Depending on the axis of rotation of the stomach, GV can be classified into organoaxial, mesenteroaxial, or combined types [4]. GV can also be classified as acute or chronic and intra-abdominal or thoracic based on anatomic localization [4]. Acute GV is frequently associated with other anatomical abnormalities, such as a diaphragmatic or paraesophageal hernia and congenital asplenia [4]. Conversely, chronic GV is commonly idiopathic and rarely associated with anatomical anomalies of the stomach or adjacent organs [5].
The clinical symptoms of GV depend on the degree of rotation and subsequent obstruction [6]. Compared with acute GV, chronic GV can have more subtle manifestations with nonspecific symptoms, such as gastroesophageal reflux, respiratory infection, and recurrent abdominal pain varying from mild to severe [7]. The most common symptom of chronic GV is nonbilious vomiting. Gastric distension, difficulty in feeding, and failure to thrive are also more common with chronic GV than with acute GV [4]. Based on these symptoms, it is difficult to diagnosis chronic GV. In this case, the patient was asymptomatic for 7 years prior to the outpatient clinic visit. Postoperative anatomic defects are frequently associated with acute GV. Therefore, chronic GV was not initially suspected as a postoperative complication. Consequently, the diagnosis of chronic GV requires a high level of clinical suspicion and an upper gastrointestinal contrast study. Treatment is categorized as medical or surgical according to the underlying pathology of GV. Acute GV requires emergency exploration due to the possibility of gastric perforation and gangrenous change. In chronic GV, the treatment plan is determined based on the patient's clinical condition, age, comorbidities, physical performance, and failure to thrive [5].
The medical treatment of chronic GV involves conservative management combined with body positioning (i.e., the head is kept slightly propped up in the prone position), prokinetic drugs, and antisecretory drugs [5]. Al-Salem [8] reported a successful outcome with conservative management in patients with chronic GV and concluded that mild to moderate symptoms of chronic GV should be treated conservatively. Persistent and severe symptoms are indications for surgical management.
Despite successful conservative management, there is a risk of chronic GV developing into acute GV [4]. The mortality rate of acute GV is more than twice that of chronic GV [4]. Thus, when determining the treatment options, conservative management may be considered for chronic GV. However, if the cause of chronic GV is suspected to be of secondary origin, surgical intervention must be considered as the primary treatment option.
GV due to postoperative adhesion in a child is very rare but should be considered in the differential diagnosis of postprandial abdominal bloating and vomiting after hepatectomy. Early suspicion and appropriate treatment are necessary. The timing of the correction of chronic GV is still controversial; persistent or severe symptoms and GV with a secondary cause indicate that chronic GV should be treated surgically.
 XML Download
XML Download