

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Protein-losing enteropathy (PLE) involves the abnormal loss of serum proteins from the vascular compartment into the gastrointestinal (GI) lumen leading to a hypoproteinemic state [12]. The documentation of increased stool losses of α1-antitrypsin along with low serum albumin and α1-antitrypsin confirms the diagnosis [12]. A proposed pathophysiologic mechanism of PLE in the Fontan circulation involves increased pressure in the lymphatics (lymphangiectasis) with loss of lymph into the GI lumen i.e. lymph-losing enteropathy (LLE) [12]. Fontan surgery is the final stage in the univentricular repair of complex congenital heart disease (CCHD) and involves anastomosis of the inferior vena cava to the pulmonary artery. PLE can occur anytime between 2 and 10 years after Fontan repair [345]. The incidence of PLE is 3–18%, equaling approximately 2,000 cases in the US and comprising a major cause of mortality [3456]. Here we present a child with CCHD who developed severe segmental PLE for which she underwent image-guided selective GI lymphatic embolization and showed prompt and sustained clinical improvement.
CASE REPORT
A 3-year-old girl born with L-transposition of the great arteries (LTGA), ventricular inversion, ventricular septal defect, and pulmonary atresia underwent a double-switch procedure (Hemi-mustard, Rastelli and Glenn) at 15 months of age. Interestingly, the mother was also born with LTGA and ventricular inversion but had not required surgery. Post-operatively, the patient developed refractory chylothoraces, which was initially treated by non-operative maneuvers but later by pleurodesis and thoracic duct (TD) ligation. She subsequently developed chylous ascites, severe PLE (serum albumin ≤0.9 g/dL, elevated alpha-1-antitrypsin in the stool) and malnutrition despite vigorous nutritional rehabilitation. At that time, she was diagnosed with narrowing of her systemic venous baffle and resultant inferior vena caval (IVC) obstruction with mean IVC pressure of 18 mmHg (normal, 3-8 mmHg). Because of the catheterization findings, the patient underwent revision of the hemi-Mustard systemic venous baffle. On follow-up catheterization, the IVC pressure had improved to 7 mmHg, but the PLE persisted. Over the next 2 years, multiple medical and nutritional interventions failed (corticosteroids, long-chain fat-restricted diet, subcutaneous heparin, octreotide, and diuretics). She became severely malnourished, suffered multiple PLE-related complications with hypoalbuminemia (albumin nadir=0.9 g/dL), failure to thrive, hypercoagulability, and osteopenia, and required frequent albumin and intravenous immunoglobulin infusions.
Bilateral lymphangioscintigraphy (Tc99m sulfur colloid) with three-dimensional single-photon emission computed tomography (SPECT-CT) showed rapid transport from the foot centrally and documented lymphatic obstruction at the cisterna chyli, with subsequent tracer dispersion further localized on SPECT-CT and progressive accumulation of radiotracer isolated in the duodenal loop area, dynamically delineating the segmental duodenal chyle leak (Fig. 1). Upper-GI endoscopy demonstrated chylous lymphangiectasia limited to the duodenum (Fig. 2A, B). Magnetic resonance (MR) enterography revealed coarse thickening localized to the duodenal loop from the pylorus to the first part of the jejunum along with lymphangiectasia and a segmental chyle leak (Fig. 3). She was then transferred to the Children's Hospital of Philadelphia, where MR inguinal intranodal lymphangiography revealed leakage (Fig. 4). When the dye was injected into the TD along with simultaneous endoscopic visualization of the duodenum, leakage of the dye into the duodenal lumen was demonstrated (Fig. 5). Selective glue embolization of the refluxing and leaking intestinal lymphatic trunk with n-butyl-2-cyanoacrylate (n-BCA) liquid embolic system (Trufill; Cordis Neurovascular, Miami Lakes, FL, USA) resulted in rapid reversal of the PLE over just a few weeks after the procedure (Fig. 6). Follow-up endoscopy revealed complete resolution of the chylous lymphangiectasia (Fig. 2C, D). The patient's edema and ascites completely resolved with weight gain and catch-up growth. She has maintained normal albumin levels (>4.0 g/dL) in over 3 years of follow-up since the lymphatic embolization.
Fig. 1
Lymphangioscintigram and single photon emission computed tomography (SPECT). (A) Bilateral Tc99m sulfur colloid lower-extremity lymphangioscintigraphy showing rapid transport from foot injection sites central to the cisterna chyli (arrow) and later tracer dispersion. (B) SPECT localizing an abnormal area in the duodenal loop (arrow) corresponding to thickening with a loss of wall (arrows) throughout the duodenal loop as seen on magnetic resonance enterography.

Fig. 2
Gastrointestinal endoscopy image showing chylous lymphangiectasia localized to the duodenal loop (A, B) and complete resolution after the procedure (C, D).
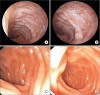
Fig. 3
Magnetic resonance enterography image showing a thickened lymphangiectatic duodenal loop (arrow) corresponding to loss of lymph throughout the duodenal loop.
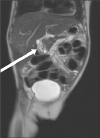
Fig. 4
Selective intranodal magnetic resonance lymphangiogram recorded prior to embolization showing enhanced contrast medium uptake by the lymphatic system and retrograde flow into the intestinal lymphatics from the intestinal lymphatic trunk, confirming a duodenal obstruction.

Fig. 5
Simultaneous blue dye injection in the thoracic duct along with endoscopic visualization of the duodenum demonstrating leakage of the dye into the duodenal lumen.

Fig. 6
(A) Conventional lymphangiogram showing the stump of the thoracic duct (TD) and the intestinal trunk prior to embolization. (B) After embolization of the intestinal lymphatic trunk with 0.5 cc of TrueFill glue, a glue cast is visible in the intestinal trunk. A microcatheter remains in the remnant of the TD.

DISCUSSION
PLE in CCHD most commonly occurs after Fontan repair. It has also been reported to occur after Glenn repair, in cases of central venous obstruction, and in cases of complete lymphatic obstruction [789]. Lymphatic obstruction may indeed be the common factor in the development of PLE in CCHD [789]. Conventional treatment strategies have included attempts to halt intestinal protein leaks and improving cardiovascular physiology using medications, the creation of fenestration, atrial pacing, or heart transplantation [10]. After the Fontan procedure, the central venous pressure (CVP) increases, typically by 12–16 mmHg, but in instances in which the CVP is substantially increased, the lymph pressure and resistance can increase to extremely high levels [11]. The pathophysiologic sequence of events following elevated CVP consists of increased lymphatic pressure and lymph flow, followed by lymphatic collateral formation and progressive resistance to lymph return to the central veins, leading to an increase in capillary filtration and lymph production [211]. In some patients, the increase in intestinal lymphatic pressure can also cause localized rupture of the lymphatics in the intestinal mucosa, resulting in lymph leaking into the body cavities (chylothorax, chylopericardium, chylous ascites) or through the intestinal mucosa into the lumen [11]. The loss of chyle including circulating immune cells and proteins resulting in PLE is called LLE. If the albumin production does not compensate for the losses, LLE results in hypoalbuminemia [1211]. It is still not fully understood why only some patients after Fontan repair subsequently develop PLE [81213]. Further implication of the lymphatic system in the etiopathogenesis has been documented on GI endoscopic biopsies showing intestinal lymphangiectasia [14]. LLE and PLE patients can have profound nutritional disorders, abnormal bone mineral density, severe lymphopenia, decreased CD4 and CD3 T cell counts, and other immune consequences [151617]. In patients with CCHD, the addition of nutritional and infectious challenges would be an added burden increasing the morbidity and mortality rates. Traditional management includes diuretics, supplemental protein, steroids, and heparin, but their efficacy remains controversial [10]. Liver lymphangiography and embolization of the hepatic lymphatic was first described in a patient in whom lymphorrhea resolved [18]. In a series of eight patients with CCHD and PLE, selective lymphatic embolization improved symptoms and albumin levels [1920].
We hypothesized that our patient's IVC obstruction coupled with the ligated TD precipitated the development of lymphatic fistulous connections to her duodenum along with lymphatic rupture with a resulting copious lymph leak. The pathogenesis of PLE in this case could be similar to Fontan physiology and secondary to a combination of underlying CCHD with an increased systemic pressure.
Noninvasive bipedal or 4-limb SPECT-CT and GI endoscopy are useful for the initial screening of chylous reflux and LLE. Subsequently, dynamic contrast-enhanced intranodal MR lymphangiography can accurately delineate the extent of chylous reflux. MR-guided direct central lymphatic puncture and selective catheter embolization with n-BCA (Trufill) can then be performed. Liver lymphangiography can identify additional lymphatics requiring embolization by demonstrating reflux of lymph from the liver into the duodenum through abnormal hepato-duodenal lymphatic communication [1819]. These may be aggravated by congestive liver disease, which further promotes liver lymph flow into the already overloaded cisterna chyli and TD. In such situations, percutaneous transabdominal TD catheterization and interruption of the lymphatic flow by lymphatic embolization can abolish this retrograde flow into the GI tract and decrease the enteropathy [19]. These imaging modalities can monitor and guide interventional lymphatic sclerosis, and decompressing lymphatic shunts into the pulmonary vein or left atrium, thereby mobilizing excessive TD lymph flow into the low-pressure left heart and reversing the lymphatic complications [1113]. Repeating the SPECT-CT and GI endoscopy after the intervention can monitor the procedure's clinical efficacy.
 XML Download
XML Download