

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Non-immune hydrops occur in approximately 3 out of 10,000 births and is associated with a high perinatal mortality rate of 50–98% [1]. Despite extensive investigations, the etiology of non-immune hydrops remains unknown in 15–25% of these cases [1]. Though non-immune hydrops carry a poor prognosis, several etiologies can be treated with potentially good results. One easily treatable but very rare condition is meconium peritonitis. Among fetuses with meconium peritonitis, antenatal finding of hydrops very rarely occurs. Early diagnosis and intervention is associated with good postnatal outcomes. Only a few cases of hydrops have been reported in the literature. We report the extensive work up of a non-immune hydropic fetus, who was postnatally found to have meconium peritonitis and surgically managed.
CASE REPORT
A 32-year-old multigravida woman, married nonconsanguineously, came to us for counselling at 31 weeks of gestation. Antenatal scan at 25 weeks was suggestive of isolated ascites with an abdominal circumference >95th percentile. The mother was Rh positive and the Doppler middle cerebral artery peak systolic velocity was normal, ruling out the possibility of incompatibility or anemia. Amniocentesis was performed. The sample was sent for karyotyping and Toxoplasmosis, Others (Syphilis, Varicella-zoster, parvovirus B19), Rubella, Cytomegalovirus and Herpes infection workup. However, the reports came back normal. Similarly, the fetal echo was normal with no other structural abnormalities. Subsequent scan at 31 weeks of gestation showed features of hydrops fetalis like polyhydramnios, pleural effusion, gross ascites, and skin and scalp edema. Bilateral lungs were hypoplastic, secondary to an elevated diaphragm. The small bowel was echogenic and matted. Internal echoes were present in the ascites. There was a history of perinatal asphyxia and developmental delay in the previous baby. Therefore, metabolic causes for hydrops fetalis were also a possibility.
A 2,300 g hydropic female baby was delivered by caesarean section at 32 weeks of gestation suspecting preterm premature rupture of membranes. The baby did not cry at birth and required resuscitation in the form of positive pressure ventilation and intubation. The baby had scalp edema, generalized skin edema, ascites, and vulvar edema (Fig. 1). Her birth weight and head circumference were >90th percentile, and length was between the 10th–50th percentile according to the Fenton's growth chart.

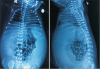
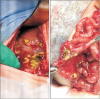
Abdominal radiograph revealed intra-abdominal calcification scattered over the bilateral hypochondrium and flanks (Fig. 2). Abdomen ultrasound revealed massive ascites with internal echoes suggestive of calcification and inferior vena cava compression. Based on these findings, meconium peritonitis was maintained as a working diagnosis. Emergency laparotomy and exploration were performed on the first day of life. Intra-operatively, there was a 10-cm perforation proximal to the ileocecal valve with matted bowel forming an abdominal cocoon with interloop adhesions. Meconium pellets were seen in the proximal ileum with calcifications over the liver, spleen, and bowel (Fig. 3). Ileal resection was performed with a double-barrel ileostomy. Histopathology of the resected bowel revealed the healed perforation with granulation tissue. Immunoreactive trypsinogen level was normal.
There is a very low incidence of cystic fibrosis in our local population and the parents in this case did not consent to further cystic fibrosis genetic workup.
Ileostomy started functioning. Feeds were initiated and gradually increased to full feeds by 7 days of life. The baby also had inguinal hernia and was subsequently operated on. She started gaining weight steadily and was discharged home. Ileostomy closure was performed at the 5-month follow-up. Her condition is good and at 8 months, she is developmentally appropriate based on the Developmental assessment scales for Indian infants [2].
DISCUSSION
The widespread use of immunoprophylaxis for red cell isoimmunization has reduced the occurrence of immune hydrops. Consequently, non-immune hydrops fetalis accounts for most cases. Meconium peritonitis has been reported as one of the etiologies of non-immune hydrops. Increasing number of fetuses with meconium peritonitis are being prenatally diagnosed by ultrasound. However, very few of them present with hydrops and only approximately 25 cases have been reported previously [34567].
Meconium is a sterile chemical peritonitis resulting from small bowel perforation in utero. The intense inflammatory reaction leads to the formation of a dense, adherent membrane that effectively seals off the intestine at the site of perforation. However, if the perforation is not completely sealed, a thick-walled cystic cavity forms, and meconium will continue to enter this cystic space. Any cause of small bowel ischemic lesion or associated mechanical obstruction such as intestinal atresia, idiopathic bowel perforation, volvulus, intussusception, congenital bands, and meconium plug syndrome, as in cystic fibrosis, may result in meconium peritonitis. In the case series by Tsai et al. [3], 1 out of 10 babies with meconium peritonitis had associated intussusception anomaly. Though meconium ileus, secondary to cystic fibrosis, accounts for 25–40% of meconium peritonitis cases according to the literature, none of the 20 fetuses in a case series of in utero meconium peritonitis in an Asian population had cystic fibrosis [48]. Our case also did not have any associated intestinal anomaly and was subsequently thriving well. Immunoreactive trypsinogen screening during the neonatal period was also negative.
According to ultrasound findings in utero, prenatally diagnosed meconium peritonitis is classified into three types: 1 (massive meconium ascites), 2 (giant pseudocyst), and 3 (calcification and/or small pseudocyst) [4]. In previous reports of meconium peritonitis presenting as hydrops, all cases were of type 2 (giant cyst) [5]. The likely cause of hydrops in type 2 meconium peritonitis is that the large giant cyst compromises venous return by obstructing the inferior vena cava, thereby increasing umbilical venous pressure [6]. A similar mechanism may explain hydrops in our case.
Ascites are usually the first ultrasound abnormality noted in prenatally diagnosed meconium peritonitis cases and some of the type 2 varieties progress to hydrops in later gestation [3]. In our case, isolated ascites were initially present and eventually progressed to hydrops by 31 weeks. Among the previous case reports, 4 fetuses with hydropic meconium peritonitis were suspected prenatally, whereas in another four, diagnosis was only made after birth [3456]. All these babies had intra-abdominal calcification after birth similar to our case. We also did not suspect meconium peritonitis prenatally and diagnosis was made postnatally.
In the study by Wang et al. [9], 4 out of 14 cases with meconium peritonitis in utero were managed conservatively and did not require postnatal surgery. Mean gestation age at diagnosis in these 4 cases was 23 weeks. Thus, early detection of meconium peritonitis correlated with a low rate of postnatal surgery and resulted in favorable neonatal outcome. They hypothesized that the perforated intestine can heal spontaneously in utero if the prenatal period is long enough [9]. Our baby had abnormal ultrasound findings at 25 weeks and was delivered prematurely at 32 weeks. Although she required postnatal surgery, she had a favorable outcome similar to that in the case series.
Thus, if the fetus already has isolated ascites with internal echoes and progresses to hydrops, meconium peritonitis needs to be considered as it is treatable and associated with good outcomes.
 XML Download
XML Download