

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic relapsing disease with peak incidence in the second and third decade of life. The incidence of IBD has increased in the last few decades leading to significant disease burden in the United States [1]. Various studies have demonstrated that the presence of psychological disorders is an independent predictor of quality of life in both teenage and adult patients with IBD [23]. Patients with chronic inflammatory disease conditions like sickle cell disease, rheumatological disease, have two to four fold increased risk of mental health and psychiatric conditions [4567]. Although the relation between gut inflammation and psychiatric disorders is poorly understood, IBD patients have increased prevalence of psychiatric disorders. Similar to adult population, strong association of depression and anxiety were reported in pediatric and adolescent population with IBD [89]. Clinical report from North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) states that pediatric IBD patients are at increased risk of poor quality of life, sub-optimal school and social functioning and thus recommends parents and medical providers to screen for depression and other mental health issues to provide appropriate ancillary services [1011]. Over the last decade, there are significant recent advances in the management of IBD and increased use of biologics resulting in better disease control. The advent of these newer modalities of treatment and their effect on the incidence of psychiatric disorders among IBD population still remains to be evaluated. While there are various studies demonstrating the increased prevalence of depression and anxiety in pediatric population, data regarding various other psychiatric disorders like panic attacks, post traumatic stress disorder, substance abuse, panic disorder, acute stress are lacking.
MATERIALS AND METHODS
We did a retrospective case control analysis using a deidentified cloud-based database (Explorys Inc., Cleveland, OH, USA). Explorys is a multi-institutional data analytics and research platform. The database includes health care data across 26 health care networks comprising of more than 360 hospitals across the United States of America with almost 64 million patient's data stored at the time of this study. All patient related data were deidentified and stored in accordance with the Health Insurance Portability and Accountability Act and Health Information Technology for Economics and Child Health standards.
Explorys collects data from clinical and financial data sources, including different electronic health records, primary care office, laboratory information systems, healthcare billing systems, and insurance plan and claim records. As most of the psychiatric/psychologic services are provided as an outpatient basis, Explorys serves as an ideal tool which captures both outpatient and inpatient data. Data collected across different hospitals were classified and stored according to Systematized Nomenclature of Medicine-Clinical Terms (SNOMED-CT) which is a comprehensive classification system emerged from the merger of two coding systems developed by the College of American Pathologists and National Health Service [12]. Explorys employs unique identification number for each patient and thus prevents duplication of records due to transfers or patient seeking medical care across different hospital systems. However, patients receiving care outside of the participating hospital system are not captured in the database.
Case selection
Based on previous literature, we preidentified ten psychiatric disorders which are commonly prevalent in pediatric population with chronic diseases. In an a-priori manner, we then queried the database for the presence of at least one of these ten following psychiatric disorders: major depressive disorder, dysthymia, bipolar disorder, acute stress disorder, anxiety disorder including generalized anxiety disorder, phobic disorder, panic attacks, post-traumatic stress disorder, adjustment disorder and substance abuse. Phobic disorders is a diagnostic term under SNOMED under diagnostic tree and it includes specific phobias such as agoraphobias, social phobia and simple phobia such as body dysmorphic disorder (previously known as dysmorphophobia).
We included patients in the age group between 5 and 24 years which better reflects the IBD population among children and adolescents until the transition of care to adult physicians. We included all patients with at least one of the following three diagnosis 1) IBD 2) Ulcerative colitis (UC) and 3) Crohn's disease (CD). All patients who did not have a diagnosis of IBD in the population served as controls for comparison. For calculating incidence, first ever diagnosis of any of the psychiatric disorders were included. Any patient already having one of psychiatric disorders in their diagnoses were excluded and not considered to be the part of at-risk population.
Data analysis
Pearson chi-square test was used to compare proportions of categorical variables and a p-value of <0.05 was considered significant. Odds ratio (OR) ratio was considered significant if the 95% confidence interval (CI) does not include 1. All prevalence and incidence rates were expressed as percentages. As Explorys does not provide individual patient data, we determined separate individual values for each combination of categorical values in order to perform multiple logistic regression. Cochran Armitage trend test was done to assess the trend in the incidence of psychiatric disorders among IBD patients. All statistical analyses except Cochran Armitage test were done using IBM SPSS Statistics for Windows, Version 24.0 (IBM Co., Armonk, NY, USA).
RESULTS
At the time of this study, the database had a total of 11,316,450 patients in the age group between 5 and 24 years. Total number of patients with a diagnosis of IBD, CD or UC were 58,020 patients. The distribution was equal among male and female (50% each) and the predominant race was Caucasian contributing to 74.0% of the total IBD population. Of the total population with IBD, 55.0% had private insurance and 37.9% were covered by public insurance (Table 1).
Table 1
Demographics of the study population

Values are presented as number (%).
IBD: inflammatory bowel disease, AA: African American, MHD: mental health disorder.
![]()
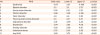
In our cohort of patients with IBD, 12,540 patients had at least one of the aforementioned psychiatric disorders. The prevalence of psychiatric disorder is 21.6% among our patients which is considerably higher in comparison to 6% in the control group. The risk of associated psychiatric disorder was significantly higher in patients with IBD, p<0.001 (Fig. 1). In our cohort, the OR of having any of the psychiatric disorders was 3.83 (CI: 3.75 to 3.91; p<0.001). Depression, anxiety and adjustment disorder collectively contribute to about 95% of all psychiatric disorders (Fig. 2). Depression and anxiety have similar prevalence of about 13% each among IBD patients. All other psychiatric disorders contribute to less than 5% individually to psychiatric disorders burden in pediatric IBD population. Among the screened psychiatric disorders, IBD patients had increased risk of associated anxiety, depression, panic disorder, phobias and dysthymias (Table 2). Although the proportion of panic disorders, phobias and dysthymias were less individually, the OR of having these associated psychiatric disorders are significantly higher among pediatric IBD population than the controls, p<0.001.
 | Fig. 1Association of various psychiatric disorders with inflammatory bowel disease.BPD: bipolar disorder, PTSD: post traumatic stress disorder, MDD: major depressive disorder.
|
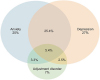 | Fig. 2Relative proportion of depression, anxiety and adjustment disorder among inflammatory bowel disease patients with psychiatric disorder.
|
Table 2
Risk of MHD in IBD
![]()
Fig. 3A demonstrates the steady significant upward trend in the incidence of psychiatric disorders in patients with IBD, p<0.001. The incidence of psychiatric disorders disease was higher in females than compared to males. Fig. 3B represents the incidence trend of anxiety, depression and adjustment disorders. Both anxiety and depression showed a significant upward trend, the incidence rate of anxiety disorder increased from 1 to 11% and depression increased from 0.5 to 10% during the study period. Using multivariate analysis, after adjusting for known confounders including age, sex, race, insurance, presence of family history of psychiatric disorder, we found a highly significant association between psychiatric disorders and IBD diagnosis (IBD or CD or UC), p<0.001 (aOR: 5.1, CI: 4.84–5.43; p<0.001). The risk of psychiatric disorders was significantly higher among females (aOR: 1.468, CI: 1.464–1.472) and among older patients between 15 to 24 years than aged less than 15 years (aOR: 2.12, CI: 1.78–2.41; p<0.001).

DISCUSSION
IBD is a systemic inflammatory disease with a waxing and waning course. The surge of inflammatory cytokines in the body and its effect on brain is suggested as a plausible explanation for the increased prevalence of psychiatric disorders [1314]. The diagnosis of a chronic illness like IBD puts the patient and the family under considerable stress, while learning to adapt with the new medical routine of medications and hospital visits. Pediatric patients with IBD are often malnourished and short statured which leads to poor body image perception. Patients undergoing surgeries with construction of colostomies may have a hard time coping with the bodily changes. Adolescents are particularly susceptible to psychiatric disorders as the onset of disease often coincides with the physical changes and emotional stress that often accompanies puberty. Often patients are started on steroids which can result in mood changes and psychosis.
Our study is the largest population-based study to evaluate the burden of psychiatric disorders in children and young adults with IBD in USA. Although similar studies exist in literature, most of the studies are single center small cohort of patients or national registries from other countries like Switzerland, Canada, Australia [15]. In our study, we report a four-fold increased risk for pediatric and young adult IBD patients to have an associated psychiatric disorder. The prevalence rate of having at least one of the psychiatric disorders is 21.6%. Although there are various studies which evaluated depression and/or anxiety among IBD patients, we did not come across a study which evaluated other psychiatric disorders like in our study for comparison.
Similar to previous studies, depression and anxiety contributes to the major proportion of psychiatric disorders in our study population. Studies have shown the presence of internalizing symptoms is a strong predictor of health-related quality of life. Walter et al. [16], reported that depression and anxiety are also associated with perceived functional disability in patients who are having clinical remission. Further, internalizing symptoms such as depression and anxiety are found to be independently associated with recurrence of IBD in adult population [1517]. The prevalence of depression varies anywhere between 13% in disease remission state to as high as 60% in patients with disease activity [38161819202122]. In our study, the prevalence of depression is estimated to be 13% amongst IBD patients and the single largest contributor of psychiatric disorders in our cohort followed by anxiety −12.7%. This slight decrease in prevalence could be explained by the inclusion of IBD patients with both active disease and those in remission. Further, the low prevalence of psychiatric disorders during earlier years of study could have decreased the overall prevalence across a twenty-year time period. In a recent study by Bernstein et al. [23], they showed that incidence rate ratio for depression and anxiety are 1.58 and 1.4 respectively. Walker et al. [18], in their report of Manitoba IBD registry, had shown that almost 25% to 30% of the IBD patients will experience depression (OR: 2.2, CI: 1.64 to 2.95) or anxiety during their life time. They also reported that females with IBD are twice at risk of developing anxiety or depression than males. In our study, depression, anxiety and adjustment disorder contributes to approximately 80% of the total psychiatric disorders. We report a five-fold increased risk of having depression and anxiety in pediatric IBD patients, (aOR: 5.1, CI: 4.84–5.43; p<0.001). Although various studies have reported IBD as an independent risk factor for psychiatric disorders, we report a much higher risk of psychiatric disorders among pediatric patients than adults.
In addition to the increased prevalence of depression and anxiety, we report significantly higher risk of other psychiatric disorders in IBD patients, p<0.001. Similar to previous studies, we found increased risk of psychiatric disorders in females than males (aOR: 1.468, CI: 1.464–1.472) and those in age group between 15 to 24 years than aged less than 15 years (aOR: 2.12, CI: 1.78–2.41; p<0.001). Our study is the first to report the pediatric incidence of psychiatric disorders in IBD patients over two decades. There is a steady increase in the incidence of psychiatric disorders, from around 2% in 2006 to about 16% in 2017. This could be due to increased awareness among the treating physicians about the importance of mental well-being in IBD management and increased screening for psychiatric disorders in office practice. NASPGHAN also recommended screening for depression and other mental health dysfunction symptoms and prompt intervention with appropriate services including cognitive behavioral therapy [1011]. Although newer modalities of treatment with better disease control has now come into play, the incidence of psychiatric disorders is still on the rise. Clark et al. [19] showed that infliximab use was not associated with rate or severity of depression in pediatric IBD patients. Whether treatment with biologics had any effect on the incidence of psychiatric disorders in IBD patients was not assessed in our study.
There are various limitations to this study, including the retrospective nature of the study. The intrinsic bias arising due to pooled data across different EHR during different time frame is an unavoidable bias unique to big pooled data analysis. Further due to differences in assigning diagnoses and coding practices, under representation of data is a potential limitation and actual disease burden may be higher than the study results. Further, all the information is based on administrative data and more relevant clinical data of patients such as severity, medication duration, response to medication, number of hospitalizations, length of stay limit further detailed analysis. Also, we did not include the medications including immunosuppressive therapy, biologics and/or surgery which plays a critical role in disease severity thereby affecting the quality of life. Lack of temporal relationship between psychiatric disorders and disease modifying intervention is also a limitation of this study.
Despite these limitations there are various strengths to our study. This is the largest population-based analysis of various psychiatric disorders among pediatric and young adult patients with IBD. Our study comprehensively evaluated the risk of various psychiatric manifestation while most of the studies were limited to anxiety and/or depression. We report an increasing incidence of psychiatric disorders over years which is alarming and needs focused services and interventions. Addressing these comorbid psychiatric disorders may pave way to improve quality of life, medication compliance and better outcomes. Further longitudinal studies are recommended to better understand the progression of IBD and outcomes in patients with concomitant psychiatric disorders and their management during childhood.
In conclusion, this is the largest US population-based study demonstrating the increased prevalence of psychiatric disorders among children and young adults with IBD. We report a high prevalence of 21.6% among our study population. Pediatric IBD patients are 5 times more likely to have an associated psychiatric disorder during the course of their illness. Our study further emphasizes the need for psychological and mental health services to be incorporated as a part of the IBD clinic. Whether incorporating mental health services in IBD management have major role in improving disease severity and quality of life should be evaluated through longitudinal studies.
 XML Download
XML Download