

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Zirconia materials with high fracture resistance have become very prevalent in today's dentistry and they have started to substitute for traditional metal-ceramic restorations.12 Zirconia has good adaptability to thermal changes and high resistance to corrosion, abrasion, and chemicals. Besides, it has a quite opaque appearance due to its dense crystalline phase. Therefore, appropriate veneering ceramics are necessary to be coated in order to provide a natural tooth-like translucency and enhance the aesthetics of restoration.3 The most common problem of restorations made with zirconia is the separation of veneering ceramics from zirconia.45 Differences in the expansion coefficient of veneering ceramics and zirconia, unsuitable designs, improper dental preparations, premature contacts, laboratory faults, and physical trauma can cause veneer ceramic chipping or breakage. This situation may aesthetically and functionally disturb the dentist and patient.6
Prosthesis should be remade when the veneer ceramic is broken. However, it can be repaired in the mouth in order to avoid the increase of cost and time, need for laboratory work, difficulty of dismantling full ceramic restorations, and discomfort of patient. Duration of the restoration can be extended with less risk by using this method.789 If restoration functions can be maintained and does not need to be renewed for another reason, intraoral repair provides an alternative treatment. Composite resins are frequently used for repair of fractures in mouth.710 The connection between repair material and fracture surface is provided with a chemical and micromechanical connection.1112 In order to increase the bond strength, surface treatments can be performed such as sandblasting with aluminum oxide (Al2O3) particles,13 acid application,14 roughening with diamond burs,15 laser application,16 sandblasting with silica coated particles,17 and silane application.12
Thermal aging is an important method applied to materials to simulate the oral environment. Many studies have reported that the durability of dental materials decreases when they are used in mouth for a certain period of time.1819 The aim of this study is to evaluate the effect of different thermal cycle applications on RBS between composite materials used for the repair of zirconia-based veneer ceramic restorations and fracture surfaces. The null hypothesis of the present study was that there are no differences between short- and long-term cycles RBS.
MATERIALS AND METHODS
The brand names, codes, and manufacturer details of all tested materials are shown in Table 1.
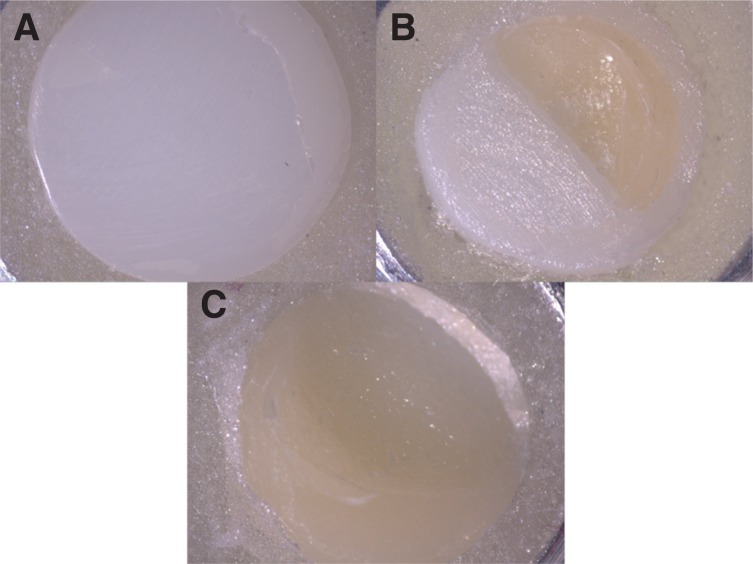
A total of 180 disc shaped specimens (7 mm in diameter and 3 mm in height) were prepared to test the RBS of veneer ceramic repair system to various ceramic surfaces treated with different methods (Fig. 1). The specimens were divided into 3 groups of 60 discs each.
Group I: Test surfaces of the specimens consisted of zirconia (Zirconia 100%).
Group II: Test surfaces of the specimens consisted of veneering ceramic (Veneer ceramic 100%).
Group III: Test surfaces of the specimens consisted of 50% veneering ceramic and 50% zirconia.
Zirconia specimens with three different shapes were produced for the specimens and the target size was reached by sintering according to the manufacturer's recommendations. The target sizes were 7 mm in diameter and 3 mm in height for zirconia specimens (Group I), 7 mm in diameter and 1.5 mm in height for veneer ceramic specimens (Group II). Veneer ceramic-zirconia specimens were 7 mm in diameter and 3 mm in height with the interface in the middle (Group III). Subsequently, 1.5 mm thick veneering veneer ceramic was applied to the test surface of zirconia discs in Group I and Group II. They were put into a vacuum veneer ceramic furnace that was be programmed to 760℃.
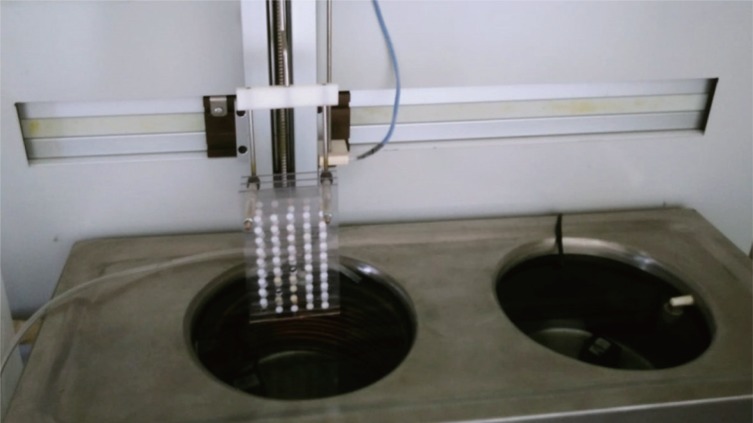
In order to simulate fracture types, Group I, Group II, and Group III were formed. Each group consisted of 60 specimens. These groups were divided into 4 subgroups: control (no thermal cycle), 3000, 6000, and 12000 thermal cycles. Therefore, a total of 12 groups were obtained (n = 15). These subgroups were named as control, 3000 T, 6000 T, and 12000 T. All specimens were placed in the apparatus prepared according to the number of thermal cycling. Afterwards, 3000, 6000, and 12000 thermal cycles were applied to the specimens in the thermal cycle device at 5 - 55℃ with dwell and transfer times of 30 seconds each (Fig. 2). Control group specimens were stored in distilled water at 37℃ for 24 hours.
The surfaces of all group specimens were roughened for 10 seconds by using a 120 µm diamond bur (Bosphorus, Istanbul, Turkey) with a high-speed water cooled clinical aerator to simulate the clinical situation. Afterwards, the materials included in the repair kit (Kuraray Clearfil Repair Kit, Okayama, Japan) were then applied in the order recommended by the manufacturer. Phosphoric acid (K-Etchant Gel) was applied to the all surfaces as a first step and, after waiting for 5 seconds, it was washed with water and dried with oil-free air. Clearfil SE Bond Primer and Clearfil Porcelain Bond Activator were mixed in a 1:1 ratio and applied for 5 seconds. Clearfil SE Bond was then applied and light-cured for 10 seconds. The same surface treatments were applied to ensure standardization for each group of specimens.
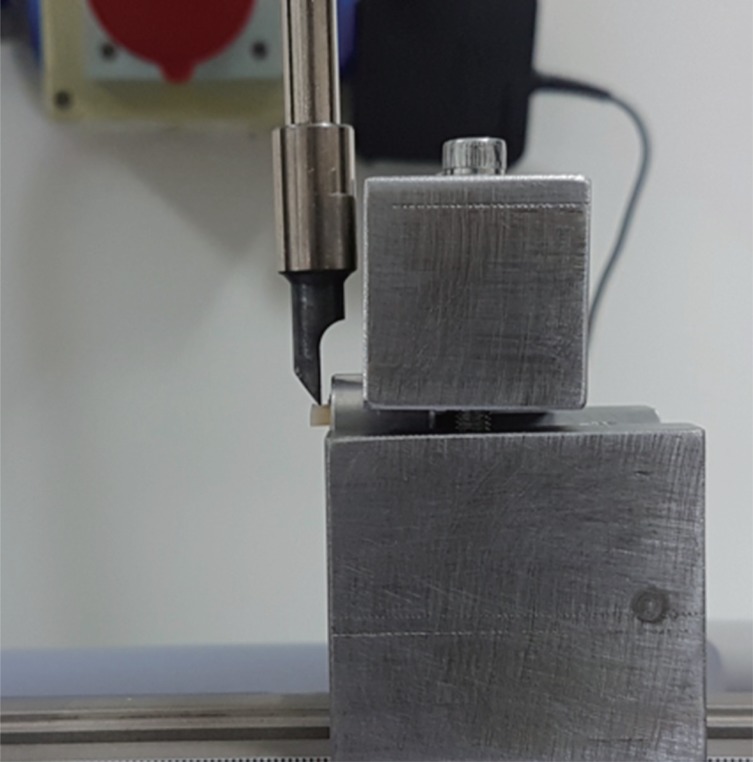
To standardize the bonding surface, a tygon tube with 3 mm diameter and 3 mm height was placed at the center of each specimen. The composite material (GrandioSo, Voco, Cuxhaven, Germany) was then placed into the tubes and photopolymerized for 40 seconds using a light-polymerizing unit (Valo Cordless, Ultradent, South Jordan, UT, USA). After polymerization, the tygon tubes were gently detached using a scalpel and all specimens were subjected to RBS test. The specimens were embedded in acrylic resin (Imicryl, Konya, Turkey) molds and placed into the universal testing machine (DCS 500, Shimadzu Corp., Kyoto, Japan). RBS tests were performed at a 0.5 mm/min crosshead speed to measure the repair bond strength values (Fig. 3). The tester blade was placed at an angle of 90° with the bonding surface and the forces at the time of separation were measured in Newton (N). The RBS values obtained in N were converted to MPa by dividing the bonding area of the composite resin.
The fracture patterns of all specimens after RBS testing were examined under stereomicroscope (Zeiss, Jena, Germany) at ×15 magnification. These examinations revealed adhesive (between composite resin and ceramic surface), cohesive (within the ceramic or composite resin), and mixed (both fracture types) failure modes.
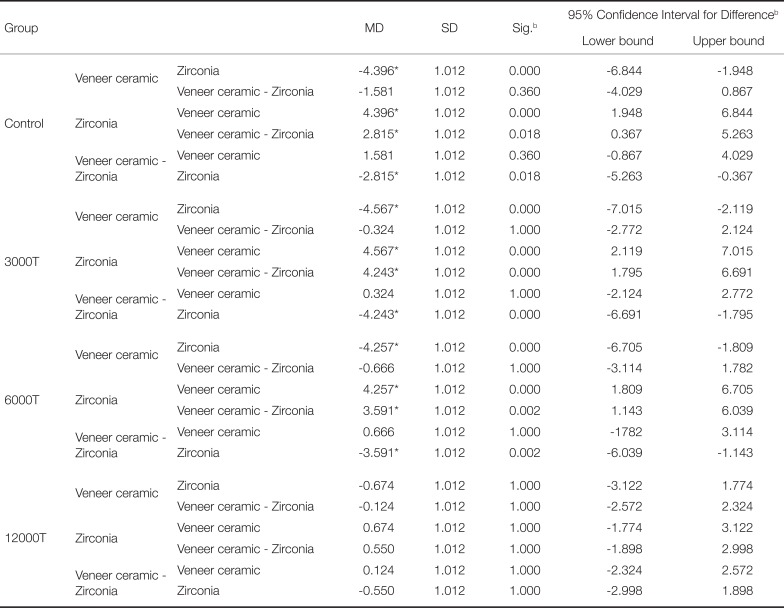
Data were analyzed using IBM SPSS Version 22 (IBM, Armonk, NY, USA). Levene test was applied to determine homogeneity of variances. Two-way ANOVA test was done to determine whether there is a statistical difference between the effect of different ceramic surfaces and different thermal cycling applications on bond strength (Table 2). Bonferroni test was used for multiple comparisons. Results were evaluated with confidence interval (95%) and level of significance (P < .05) (Table 3).
RESULTS
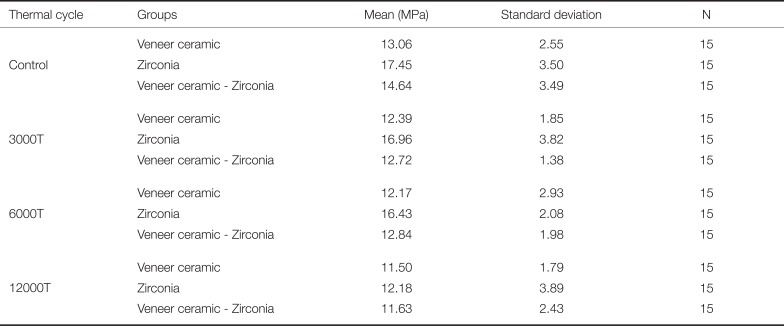
Table 4 shows the means and standard deviations values of all groups. The highest and lowest RBS were obtained in control zirconia and 12000 T veneer ceramic groups, respectively. When we examined the effect of thermal cycling on the RBS between veneer ceramic specimens and repair composite, the highest value was obtained in control group and the lowest value was taken in 12000 T group. Although the RBS values of control group were higher than the RBS of 3000 T and 6000 T groups, no statistically significant difference was found among control, 3000 T, 6000 T, and 12000 T groups (P > .05).
Among zirconia specimens, the highest value was observed in control group and the lowest value was found in 12000 T group. The RBS values of control group were higher than the RBS values of 3000 T and 6000 T groups, but there was no significant difference among these groups. 12000 T group had significantly lower binding values than control, 3000 T, and 6000 T groups.
Within the veneer ceramic-zirconia specimens, the highest RBS value was obtained in control group. The lowest value was found in 12000 T group and the difference was statistically significant. Although the RBS values of control group were higher than the RBS values of 3000 T and 6000 T groups, no significant difference was observed among these groups. There was also no significant difference among 3000 T, 6000 T, and 12000 T groups.
When the RBS with the repair composite is examined within control, 3000 T, and 6000 T groups, there was no statistically significant difference between veneer ceramic and veneer ceramic-zirconia specimens, whereas zirconia specimens showed significantly higher values.
In 12000 T group, the highest RBS value was found in zirconia specimens and the lowest value was in veneer ceramic specimens. However, there was no significant difference among veneer ceramic, zirconia, and veneer ceramic-zirconia specimens.
Veneer ceramic specimens had only cohesive failures and zirconia specimens exhibited only adhesive failures. In veneer ceramic-zirconia specimens, adhesive and higher mixed type failures were observed (Fig. 4).
DISCUSSION
In the repair process made with composite resin, the hypothesis that the lowest RBS values will be seen in fractures where the veneer ceramic is separated and only the zirconia remains is rejected, in line with the findings of our study. The hypothesis that RBS values between composite resins and ceramics will decrease as the number of thermal cycles increases is partially accepted. Applying 12000 thermal cycles significantly reduced bond strength in veneer ceramic-zirconia and zirconia specimens, but the decrease in veneer ceramic specimens did not make a statistically significant difference.
Many studies have been conducted on the bond strength between zirconia and veneer ceramic. However, fracture of the veneer ceramic remains as a frequently reported complication.4202122 Adding new veneer ceramic to the broken restoration is almost impossible in the mouth due to the structure of veneer ceramic. Therefore veneer ceramic fracture is a difficult situation for both the patient and the dentist.23 When the fracture area is small, repair can be performed in the mouth by using composite resins. This method is often preferred because of its ease of application, ability to be performed in one session, having different colour options, valid aesthetic appearance, and being economical. Recent developments in adhesive systems provide successful results.2425
The repair process was based on the macro mechanical bond between the repair material and fracture surface in previous years.26 It is built on chemical and micro-mechanical connections as well as the connection strength of surface treatment in recent years.2728 Hydrofluoric acid (HF) roughening process is one of the most commonly used methods to increase the bond strength between ceramic surface and resin.2930 It dissolves the glassy and crystalline content of ceramics and increases micro retention. HF acid process is effective in silica-based ceramics. Since zirconia and alumina ceramics are not silica-based, they are resistant to acid application.14 Shiu et al.31 applied various surface treatments on feldspathic ceramic in order to evaluate the RBS of resin cement to feldspathic ceramic. They obtained the highest bond strength values in specimens with 10% HF acid applied. Similarly, Akyıl et al.32 got the highest bond strength between feldspatic ceramic and repair composite resin in HF acid applied specimens. Contrary to these studies, it has been reported that application of HF acid to veneer ceramic surface may cause premature failure when it is not used in ideal proportions and time. A porous structure on ceramic surface may be formed.6 In addition, it should be applied carefully because it has harmful effects on skin, soft tissues, and lungs by inhalation.33 In some repair sets, 35 - 40% phosphoric acid (H3PO4 acid) is added as an alternative to HF acid.17 Leibrock et al.34 analyzed RBS between veneer ceramic and repair composite after thermal cycling and mechanical loading and found no significant difference between systems using H3PO4 acid or HF acid. Because of its chemically aggressive nature, HF should be avoided and replaced with H3PO4 acid, which is not harmful to tissues and produces the same effects when used with silane agent. In this study, K-etchant gel with 40% H3PO4 acid was applied to the specimen surfaces according to the usage advices of the company.
When the fracture site of the restoration is to be repaired with composite resin, the surface roughening process is performed with diamond burs, which is a widely used method to increase mechanical retention and to remove veneer ceramic structure and contaminated area.1535 Şen et al.36 worked on the surface roughening treatments that are applied with sandblasting, acid, and diamond bur. They examined the effect of veneer ceramic repair materials on the bond strength. The highest bond values were obtained in the acid applied groups. However, they did not find a significant difference in the bonding forces obtained after acid applying and diamond bur roughening, and reported that roughening of the veneer ceramic with diamond bur is a more practical method. Kirmali et al.35 found high bond strength of composite resins after roughening of zirconia ceramics with diamond burs. In this study, surface roughening process with a diamond bur was applied to the specimens as described in the instructions of the repair kit.
The chemical bond between metal or ceramic surfaces and the resin is formed by silanes or phosphate monomers.37 Silane application is the main factor for bonding the composite resin onto the ceramic surface.38 Silane increases the wetness of the surface, allowing the low viscosity resin to flow more easily and increasing micromechanical retention.3940 After the surface treatments, surface should be wetted with 10-methacryloxidecyl dihydrogen phosphate (MDP) monomer to increase the bond strength between zirconia surface and the repair composite.4142 Since MDP monomer is water resistant, it provides stable adhesion by showing resistance to hydrolysis during different aging methods.43 Therefore, in our study, Clearfil Repair kit was used, which includes silane and MDP based adhesive.
Many studies have reported that the durability of dental materials decreases when they are used in mouth for a certain period of time. There are aging methods applied to the materials to mimic the oral environment.1819 Long-term storage in water with constant temperature and thermal cycling are clinical aging parameters and they are often used when measuring the bond strength of resins.194445 Passia et al.46 reported a significant decrease in tensile bond strength values between zirconia and adhesive systems after thermal cycling. Özcan and Vallittu14 evaluated the effect of acid, sandblasting, and silica coating on bond strength of BIS-GMA-based resin with six different ceramics and stated that the application of thermal cycle significantly reduced bond strength in all groups. D'Amario et al.18 reported that the application of thermal cycling significantly reduced the bond strength between zirconia and resin cement. Similarly, in this study, statistically significant lower values were obtained for the bonding forces between zirconia specimens and composite resin in 12000 T group than the control group. Özcan et al.15 compared the durability of repair bond strength of a resin composite with reinforced ceramic. They applied 12000 thermal cycles to some of the specimens after 150 days of water storage. Compared to other repair kits in their study, Clearfil repair kit showed significantly lower bond strength in thermal cycled specimens. The use of micro tensile test, various specimen sizes, and prolonged storage of specimens can be the reasons of differences in results. We obtained higher bond strength from the veneer ceramic specimens in control group than the veneer ceramic specimens in 12000T group, but the difference was not statistically significant.
Kamada et al.47 evaluated the effect of different surface treatments on the bond strength between ceramic (Cerec 2) and resin luting agents. They showed that there was no significant difference between water storage (37℃, 24 hours) and 20000 thermal cycle applications for the values of RBS of H3PO4 acid-silane applied specimens. Matsumura et al.48 roughened the feldspatic veneer ceramic surface with 50 µm Al2O3 powder and applied resin cement. They reported that the bond strength values decreased after thermal cycling in samples treated with Clapearl DC resin cement and Clearfil Porcelain Bond Activator, but the difference from the specimens without thermal cycling was not significant. Appeldoorn et al.7 evaluated the relationship between veneer ceramic and composite resin. Half of the specimens were kept in water at 37℃ for 24 hours, the other half stayed in water for 3 months and then were applied 2500 thermal cycles (5 - 55℃). Considering different veneer ceramic repair sets, there was no statistically significant difference for bond strengths after the aging process in three different repair sets. In our study, RBS values of veneer ceramic specimens with composite resin decreased after thermal cycling, but no significant difference was observed compared to control group.
In the studies, fracture surfaces were classified as adhesive, cohesive, and mixed types.495051 Uludamar52 and Akyıl et al.53 studied about the effects of different surface treatments on the connection between resin cement and zirconia and reported that the fractures were adhesive type in all specimens in their work. In this study, we observed that adhesive type fractures exist between zirconia specimens and composite resin.
Cohesive type fractures have been reported in several studies investigating the veneer ceramic-composite resin connection.2834 Külünk et al.54 observed that there were only cohesive type failures in their repair process with Clearfil repair kit on IPS Empress Esthetic. All cohesive fractures were within the substructure material. Ozdemir et al.55 showed the effect of different surface treatments on veneer ceramic-composite resin bonding and reported that all specimens that used the Clearfil Repair set had cohesive fractures. In this study, we observed cohesive type fractures among the all veneer ceramic specimens. The fractured parts were formed as a result of separations on veneer ceramic surface. As a result of applying the materials in the repair kit, the bond strength between the composite resin and veneer ceramic may have exceeded the strength limit of the veneer ceramic.
If there is a large amount of cracks on the surface of the remaining veneer ceramic after the fracture, fracture formation may be seen again after the repairs due to the weakness of the integrity of the structure.56 Fractures that occur after intraoral repair using composites are reported to occur due to chewing forces, trauma, or incorrect bonding procedures.30 Before starting the repair process, the cause of the breakage must be determined and eliminated in order to avoid failure.
The limitations of this study can be stated as follows. Only the RBS test was applied among bond strength tests. Different surface treatments were not applied. Also, the size and shape of specimens were not similar to the clinical crown anatomy. More accurate results can be achieved by applying a mechanical cycle in addition to the thermal cycle. The use of different materials, application of different working methods, and changes in the interface surface area may change the results of the bond strength test.
CONCLUSION
Considering the composite resin and specimens in all groups, RBS values decreased after the thermal cycle application. This decrease did not create a statistically significant difference in veneer ceramic specimens. However, a significant difference was observed after the application of 12000 thermal cycles in zirconia and veneer ceramic-zirconia specimens. The highest RBS values between the specimens and composite resin were obtained in zirconia specimens and the lowest bond strength values were obtained from veneer ceramic specimens in all control and thermal cycling groups.


 XML Download
XML Download