

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cobalt-chromium (Co-Cr) alloys have been commonly used as the main structure of fixed dental prostheses as an alternative to Ni-Cr alloys for patients with an allergy to Ni.1 The alloy exhibits good mechanical properties with a high modulus of elasticity that increases the stress distribution of the framework, thereby reducing frequency of fracture of the framework.2 Conventionally, the Co-Cr alloys have been applied to dental prosthesis using the casting technique.1 The casting technique is based on melting of the alloy ingots and subsequent cooling for making the shape of the framework.3 The process is not only a time- and labor-intensive task but also inevitably involves shrinkage phenomenon during the cooling period of the liquefied alloy.4 When shrinkage is not completely controlled, misfit of the prosthesis to abutment occurs. This inherent feature of the casting technique facilitated alternative methods for the fabrication of prostheses using Co-Cr alloys.
Over the last decade, manufacturing processes using computer-aided design/computer-aided manufacturing (CAD/CAM) technology have become increasingly important in the production of dental prostheses.56 With the introduction of CAD/CAM in the field of dental prosthodontics, the milling method became the technique of choice in the fabrication of dental prostheses.7 The milling method is more efficient and streamlines the fabrication workflow, and provides high predictability of the resultant prostheses as opposed to conventional method.8 In the milling method, the formation of internal flaws and porosities can be minimized using homogeneous alloy blocks produced under standardized industrial conditions.9
Fully sintered Co-Cr hard alloy blocks were initially used for milling prostheses.10 Hard machining showed a high precision because the alloy block was trimmed to the actual size of the prosthesis without contraction.11 However, the fully sintered alloy blocks were not widely used because of the excessive abrasions inflicted onto the cutting burs and costly processing machines.12 To overcome these limitations, presintered alloy blocks that contain organic binders, which function as adhesive agents between alloy powders, were developed.13 The presintered blocks are processed by dry milling in the pre-state and subsequent sintering (Milling-sintering method).13 During the sintering, the binders are burned off, and alloy powders are sintered.14 Relatively lower hardness of presintered blocks in comparison with the hardness of fully sintered blocks contributes toward a more time- and cost-effective milling process.15
The prognosis of fixed dental prostheses essentially relates to the fit accuracy of the prostheses to abutments.16 The fit accuracy is evaluated at the marginal, axial, and occlusal regions of the prostheses by measuring the gap between the inner surface of the prosthesis and abutment surface.17 Among the measurement regions, marginal area is considered the most important in terms of the longevity of prosthesis because an ill-fitting margin increases the risk of critical biological or technical failures.18 Common complications are gingival irritation, alveolar crestal bone loss, dental caries, and cement dissolution.1819 Marginal discrepancy can be evaluated by measuring the distance between the most extended point of the prosthesis margin and the marginal line of the prepared abutment.16 As for measurement methods of marginal discrepancy, direct detection by dental explorer and indirect silicone replica technique has commonly been implemented in the clinic.20 Currently, with the advent of digital technologies in dentistry, the space between the prosthesis and abutment can be three-dimensionally visualized, and diverse quantitative geometric analyses can be performed.11
Although several in vitro studies were recently conducted for investigating the fit accuracy of prostheses fabricated by using the presintered metals and the milling-sintering method, the actual fit of the prostheses has not been fully verified in a clinical study. Therefore, the purpose of this study was to examine the geometric marginal discrepancies of the metal-ceramic prostheses made by the milling-sintering method in comparison with results by the casting method.
MATERIALS AND METHODS
The overall workflow of this clinical study is described in Fig. 1. Twelve consecutive patients (5 men, 7 women; age range, 40 – 78 years; mean age, 64.6 ± 12.0 years) requiring an implant-supported single fixed dental metal-ceramic prosthesis were included in this study (3 cases for the maxilla, 9 cases for the mandible). All patients were treated at the identical prosthodontics department of a university hospital. Following the design of this study, two metal-ceramic crowns were fabricated for each patient, using the millingsintering method by employing a presintered Co-Cr alloy and the casting method by employing a casting alloy. The study protocol was approved by the Institutional Review Board of Kyungpook National University Hospital (2019-02-01-00).
The identical clinical process was conducted for each patient by a single clinician. A preliminary impression was taken with a stock tray using irreversible hydrocolloid (Aroma fine plus normal set, GC, Tokyo, Japan) and a diagnostic cast was made. To provide the space for the impression material, a 2.0-mm-thick relief base plate wax was laid on the cast and a customized impression tray was fabricated with an autopolymerized acrylic resin (Ostron 100, GC, Tokyo, Japan). Then, an intraoral silicone impression was taken with light- and regular-body and polyvinyl siloxane (Aquasil Ultra XLV and Aquasil Ultra LV, Dentsply Sinora, Philadelphia, PA, USA) for the implant using the open tray technique with a pick-up type impression coping. Afterwards, a definitive cast was made with type IV dental stone (Fujirock EP, GC, GC, Leuven, Belgium) according to the ratio provided by the manufacturer. To make the first prosthesis using the milling-sintering method, the master cast was digitized using a laboratory scanner (IDC S1, Amann Girrbach, Koblach, Austria), and the scan image was transferred to dental CAD software (IDC D1, Amann Girrbach, Koblach, Austria) where a custom abutment and a prosthetic coping were designed in optimal shapes (Fig. 2). The design of prosthetic coping was converted to a non-precious metal coping by milling a presintered Co-Cr alloy block (Soft Metal, LHK, Chilgok, Korea) using a 5-axis milling machine (Ceramill Motion 2, Amann Girrbach, Koblach, Austria). The milled coping was subsequently sintered to full density in the corresponding sintering furnaces (Well-Burn, Denstar, LHK, Chilgok, Korea) (Fig. 3). To compensate the sintering shrinkage, the copings were formed larger than the final size when milled in presintered alloy blocks. All procedures were performed following the manufacturers' instructions. The second casting copings were made with traditional lost wax technique. A 12 micron die spacer (SPACE-IT, Taub Products, Jersey City, NJ, USA) was applied to the implant custom abutment starting 1.0 mm above the finish line with one coating. After the full contour framework wax-up procedure, 1.5-mm cutback was done to provide the space for porcelain veneering at the buccal side. The wax pattern was then invested in a phosphate-bonded investment (Bellavest SH, Bego, Bremen, Germany) according to the manufacturer's instruction, and vacuum mixed to remove air bubbles. The casting ring was filled completely with the investment mixture into the rim and left for 20 minutes for setting. Then the wax was burned out of the mold and the ring was placed in an induction-heated centrifugal casting machine (Sejin dental, Seoul, Korea) and cast using a casting alloy (4-all, Ivoclar Vivadent, Schaan, Liechtenstein). The cast specimen was treated with airborneparticle abrasion using 110 micron aluminum oxide (Al2O3) particles at 4 bar and sprue was cut. After that, finishing and polishing with tungsten carbide instruments was done. The die spacer layer was then removed from the abutment by using a steam cleaner. Porcelain veneering (VITA VMK Master, Vita Zahnfabrik, Bad Säckingen, Germany) was conducted manually in both prostheses. Information on the materials used is presented in Table 1. The fabrication of both prostheses was carried out by a single dental technician.
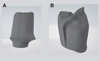
Marginal gap of the prosthesis was evaluated using clinical techniques and the triple-scan technique on the day of prosthesis delivery. The custom abutment was first connected to the implant, and the metal-ceramic prostheses were tried in to the abutment (Fig. 4). Clinical marginal adaptation of the prostheses was examined using an explorer (Trudent, New Delhi, India), relying on the visual and tactile sense of single examiner. Four circumferential recordings were made at the middle of the buccal, lingual, mesial, and distal surfaces of each prosthesis. The clinical misfit was defined as over-extended margin, under-extended margin, and incomplete seating. Same explorer was used to investigate all prostheses and one examiner performed the clinical evaluations for the methodological standardization. As per the protocol for Triple-scan technique,11 three digital scans were taken using an intraoral optical scanner (CS3600, Carestream, Rochester, NY, USA). The first scan was of the fabricated custom abutment alone, the second was of the custom abutment inside the oral cavity, and the third was of the metal-ceramic prosthesis on the custom abutment inside the oral cavity. The data of the three scans were exported to image analysis software (Geomagic DesignX, 3D Systems, Rock Hill, SC, USA). In the software, the first and the second scan images were merged with the third scan image using an area-designated best-fit algorithm (Fig. 5A).11 The cross-sectional line images were bucco-lingually and mesiodistally obtained at the position of custom abutment (Fig. 5B). Absolute marginal discrepancy was measured at the margins of the buccal, lingual, mesial, and distal areas.16
Statistical analysis was conducted using the IBM SPSS Statistics v25.0 statistical software package (IBM Corp., Armonk, NY, USA). Marginal discrepancy for each region was expressed as mean ± standard deviation. The difference of marginal discrepancy between prostheses made by the milling-sintering and casting methods was visualized for each treatment case using a line plot. Mann-Whitney U test was used to compare the efficacy of the fabrication method between the two prostheses. Statistical significance was set at a P value of < .05.
RESULTS
The two metal-ceramic prostheses fabricated by the milling-sintering method and the casting method were completely seated to the abutment. No specific over- or under-extended margins were noted when visual and tactile inspection was carried out using an explorer. The patients could not recognize the difference between the two prostheses with regard to their fabrication methods based on the tactile sense of their tongue. The absolute marginal discrepancy of prostheses made by different methods in each patient is exhibited in Fig. 6. Eight patients (66.7%) showed a lower marginal discrepancy of the protheses made using the milling-sintering method than that of the prosthesis made by the casting method. The specific values of marginal discrepancy of prostheses at measurement points and comparative evaluation are presented in Table 2. The misfit of the milling- sintering method showed no significant difference from that of the casting method (P = .782). There was no relationship between the amount of marginal gap and the measurement point.
DISCUSSION
The objective of this study was to investigate the marginal discrepancy of a fixed dental prosthesis made by the milling-sintering method using a presintered Co-Cr alloy in clinical cases. The metal-ceramic prosthesis made by implementing the milling-sintering method demonstrated marginal adaptations similar to that produced by the casting technique. The results of the present study are in close agreement with those of recent in vitro studies.112122 Kocaağaoğlu et al.21 showed that the milling-sintering method had an outcome equivalent to the hard-milling method and was superior to the casting or 3D printing methods. Pasali et al.22 reported the application of milling-sintering method to single implant-supported metal-ceramic crowns. The results of the study revealed that the marginal fit of crowns prepared by the milling-sintering method produced acceptable values (< 120 µm). The accuracy of the milling-sintering method in a full-arch framework design on an edentulous implant model was verified in the study conducted by Woo et al.11 The marginal discrepancy in the milling-sintering group was comparable with that in the hard-milling group and better than that in the conventional casting group.
Since the introduction of presintered Co-Cr alloys to dentistry, fundamental characteristics of the material have been investigated. Biological response from the material itself is important to avoid harmful effects such as metal allergies and cell toxicity because dental prosthetic material has the potential to function in the oral cavity for a long-time period in close contact with the tissues. It was reported that the presintered Co-Cr soft alloys do not induce harmful biologic responses compared with those induced by conventional casting alloys.23 Inductively coupled plasma-mass spectroscopy showed higher fibroblast viability with smaller release of Co ions in the specimens made by a presintered Co-Cr alloy.23 With regard to mechanical property, it has been known that the products made by presintered alloys have high ductility, which could facilitate effective burnishing of prosthesis in a clinical setting.24 In another study that compared the mechanical properties of Co-Cr alloys using a tensile test, specimens produced by presintered alloys showed greater elongation, whereas specimens produced by 3D printing powders showed higher proof strength.25 Sintering after the milling process is inevitable for a presintered alloy to be in the fully sintered state. The effect of sintering temperatures on the mechanical properties of a presintered Co-Cr alloy was examined, and the result indicated that over-sintering, about 1350℃, is better than under-sintering in terms of strength. It also showed that the number and size of the pores in the microstructure were largely related to the sintering temperature.26
To the best of our knowledge, our study is the first to provide clinical data on the marginal fit of fixed dental prosthesis fabricated using a presintered Co-Cr alloy and comparative results for the misfit of prosthesis fabricated using the conventional casting method in the same subject. Even though this article showed the clinical accuracy of the milling-sintering method, large-scale randomized controlled clinical studies are necessary for confirming the results of this study. Moreover, various types of prosthesis design, such as multi-unit or tooth-supported, need to be included in further studies to extend the application of this fabrication method.
CONCLUSION
Within the limitations of this study, the marginal fit of a fixed dental prosthesis made by the milling-sintering method with a presintered Co-Cr alloy was equivalent to that of the casting method in clinical use. Presintered soft alloys could be an alternative to casting alloys and fully sintered hard alloys in dental prostheses.







 XML Download
XML Download