

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus and periodontal disease are two common diseases that are in close relation to one another.1 Diabetes mellitus alters glucose tolerance or impairs metabolism of lipids and carbohydrates.2 It is considered as a manifestation of a persistent chronic low-grade inflammation.3 Periodontal disease is a chronic inflammatory condition that causes an imbalance in anabolic and catabolic processes, ultimately resulting in resorption of alveolar bone or tooth-supporting tissues.4
Previous clinical studies56 provided evidence on a mutual relationship between diabetes mellitus and periodontal disease. In diabetes, hyperglycemia is a potential risk factor for periodontitis.789 In periodontitis, a systematic review by Borgnakke et al.10 suggested that severe periodontitis was related to significantly elevated serum levels of HbA1c.
Previous research1 has given effort to clarify the underlying mechanisms between diabetes mellitus and periodontal disease. Gingival crevicular fluid is a serum transudate originating from the gingival plexus of blood vessels.11 It has been shown that elevated serum levels of inflammatory mediators and cytokines such as tumor necrosis factor-alpha (TNF-a) in diabetic patients correlated with increased levels of these mediators and cytokines in gingival crevicular fluid.12 Systemic infection of gram negative organisms such as Porphyromonas gingivalis, Tannerella forsythensis, Prevotella intermedia or their products may promote an elevated inflammatory state and increased levels of serum inflammatory markers.13 Serum markers of inflammation such as C-reactive protein (CRP), IL-6, and fibrinogen are significantly higher in patients with periodontitis, than in patients without periodontitis.141516 Gram-negative infections in periodontal disease may also engender insulin resistance and exacerbate metabolic control in patients with diabetes.17
In view of these relations between diabetes mellitus and periodontal disease, it has been speculated that treatment of periodontal diseases can improve metabolic control of diabetes. 18 According to previous studies,1920 the magnitude of the reduction in HbA1c ranged from 0.27% to 0.48% 3 – 4 months after periodontal treatment. Despite periodontal treatment seeming to ameliorate metabolic control, evidence was not sufficient to significant associate periodontal treatment and metabolic control in patients with diabetes.21 According to a consensus report, there is a lack of data to manifest that this effect is maintained over 6 months following periodontal treatment.22
Prosthodontic therapy, such as restoration, implant prosthesis, and removable partial denture, have been reported to cause dental problems on abutment teeth.23 Plaques can be accumulated on teeth used as abutment, thus becoming a risk for infection and deteriorate metabolic control for patients with diabetes. However, there was not enough evidence to conclude whether these changes on abutment teeth could be mitigated when periodontal therapy was combined.
Therefore, in this retrospective study, we sought to compare the changes in glycemic control between patients receiving periodontal and prosthodontic therapy and patients not receiving the therapy over 6 month period.
Go to : 
MATERIALS AND METHODS
70 diabetic patients who visited the Kyungpook National University Hospital to monitor their HbA1c levels between January 2016 and May 2018 were analyzed in this study. Among the 70 patients, 35 patients who also visited Kyungpook National University Dental Hospital to receive periodontal and prosthodontic therapy during the same period was designated as the treatment group, and the other 35 patients who did not received such therapy was designated as the control group.
The treatment group was further divided to subgroups according to the type of periodontal therapy: active periodontal therapy and supportive periodontal therapy. The treatment group was also classified based on whether prosthodontic therapy was carried out or not (with or without prosthodontic therapy). Active periodontal therapy encompassed oral hygiene instruction, full mouth scaling, subgingival curettage, extraction and flap operation performed under local anesthesia. Supportive periodontal therapy consisted of oral hygiene instructions, full mouth scaling, and root plaining. The mean interval between visits for supportive periodontal therapy was 3.5 months. Prosthodontic therapy consisted of implant prosthodontics, single and bridge restorations, occlusal adjustment, and removable partial denture. Patients in the treatment group received at least one of these therapies.
In the treatment group, data such as the type of periodontal therapy, the presence or absence of prosthodontic therapy, and the number of teeth lost, were collected. The number of teeth lost was calculated by subtracting the number of remaining teeth from 32 teeth.
A statistical analysis was performed using a SPSS software (IBM SPSS Statistics for Windows, Version 23.0. IBM, Armonk, NY, USA). Comparison of HbA1c levels before and after therapy within groups, and difference in extent of HbA1c reduction between groups were performed using independent t-test. Correlation between level of HbA1c before therapy and the number of teeth lost was investigated through simple linear regression analysis. It was considered to be statistically significant when P value is below 0.05.
Go to :
RESULTS
Clinical characteristics are summarized in Table 1. At baseline, the two groups had similar mean values for age, gender distribution, and the time interval between the initial and final HbA1c levels.
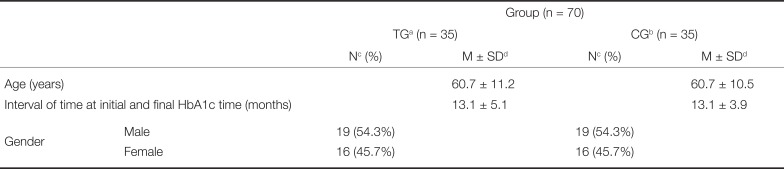
Table 1
Clinical characteristics of patients of treatment and control groups
![]()
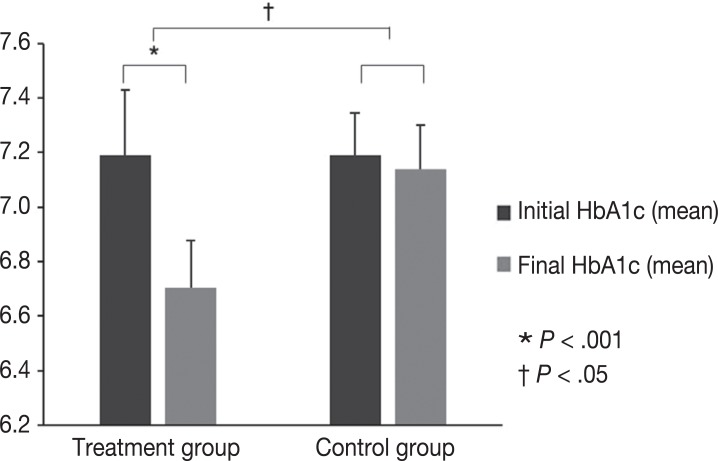
The HbA1c levels in the treatment group decreased from 7.2 to 6.7 (P= .001) following periodontal and prosthodontic therapy, and this change was statistically significant (Fig. 1). During the similar time frame, the HbA1c levels in the control group also decreased from 7.2 to 7.1 (P= .580) but this change was not statistically significant. Furthermore, the difference in changes between the two groups was statistically significant (P= .011, Fig. 1).
Clinical characteristics of two subcategories of the treatment group according to the type of periodontal therapy are summarized in Table 2. The two groups were well matched for age, gender distribution, and the time interval between the initial and final HbA1c levels. The only statistical difference between the two groups was the mean interval of therapy; the mean interval of active periodontal therapy group was 1.6 ± 0.7 months, whereas that of supportive periodontal therapy group was 3.5 ± 0.5 months.
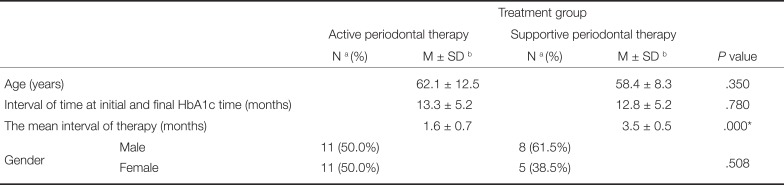
Table 2
Clinical characteristics of two subcategories of the treatment group according to the type of periodontal therapy
![]()
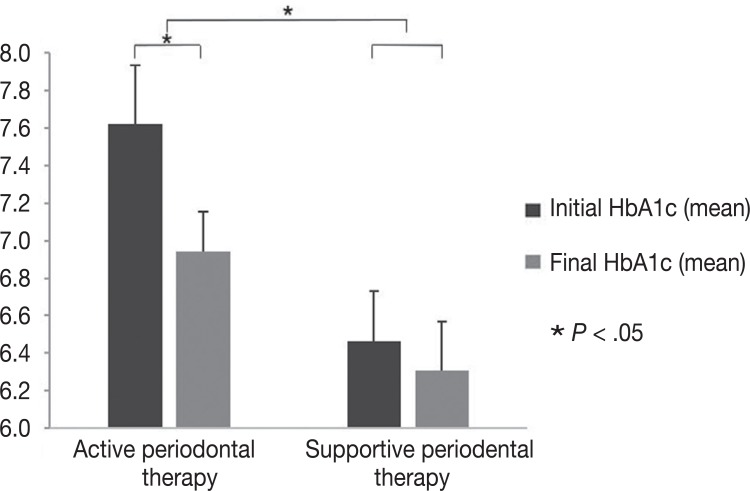
The HbA1c levels in the active periodontal therapy group decreased from 7.6 to 6.9 (P= .003), and this change was statistically significant (Fig. 2). During a similar time frame, the HbA1c levels in the supportive periodontal therapy group also decreased from 6.5 to 6.3 (P= .194), but this change was not statistically significant. Furthermore, the difference in changes between the two groups was statistically significant (P= .029, Fig. 2). The initial HbA1c level of the active periodontal therapy group and supportive periodontal therapy group was 7.6 and 6.5, respectively, and this difference was statistically significant (P= .016).
Clinical characteristics of two subcategories of the treatment group based on whether or not prosthodontic therapy was carried (with or without prosthodontic therapy) were summarized in Table 3. The two groups differed in age, gender distribution, and the time interval between the initial and final HbA1c levels, but this difference was not statistically significant.
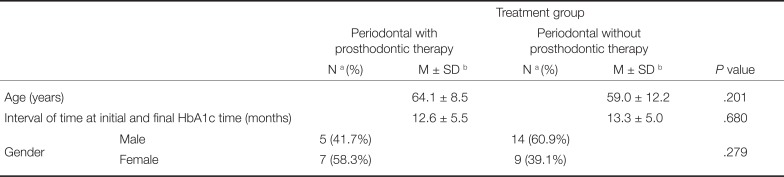
Table 3
Clinical characteristics of two subcategories of the treatment group based on whether prosthodontic therapy was carried out or not (with or without prosthodontic therapy)
![]()
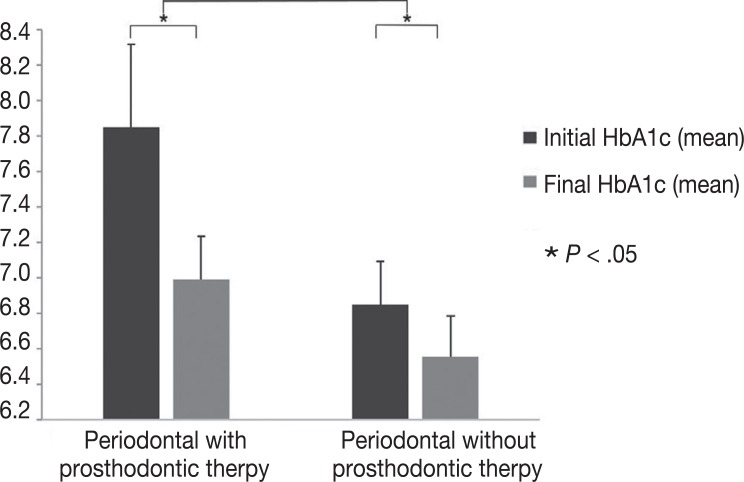
The HbA1c levels in the periodontal with prosthodontic therapy group decreased from 7.9 to 7.0 (P= .025), and this change was statistically significant (Fig. 3). During a similar time frame, the HbA1c levels in the periodontal without prosthodontic therapy group also decreased from 6.8 to 6.6 (P= .014), and this change was statistically significant (Fig. 3). However, the difference in changes between the two groups was not statistically significant.
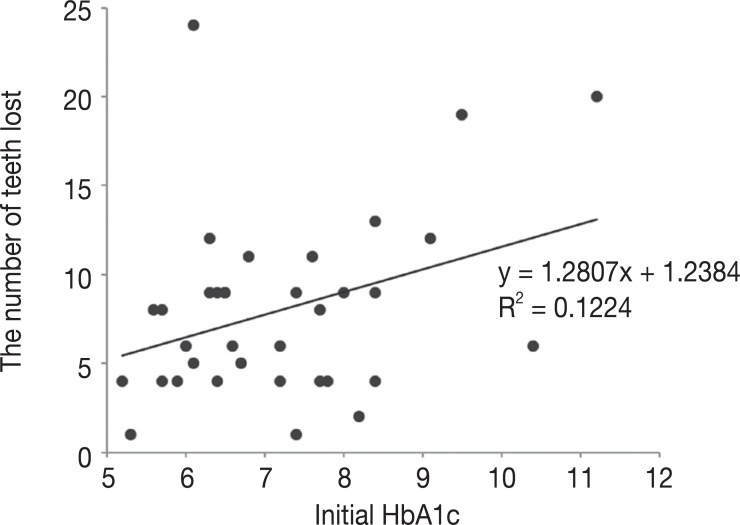
The simple linear regression model showed that there was a positive correlation between initial HbA1c and the number of teeth loss in the treatment group, which was statistically significant (P= .039, Fig. 4).
Go to :
DISCUSSION
There were previously published studies242526 investigating the relationship between periodontal therapy and HbA1c levels. Moeintaghavi et al.27 noted a significant reduction of HbA1c level (0.74%) in the treatment group after 3 months. Sun et al.28 also observed a reduction of HbA1c level (0.5%) in the treatment group after 3 months. Our results supported those of previous studies, showing a reduction of HbA1c level from 7.2 to 6.7 (0.5%) after periodontal and prosthodontic therapy.
The mechanism by which HbA1c decreases after periodontal and prosthodontic therapy can be explained by the regulation of TNF-alpha (Tumor Necrosis Factor-alpha) levels. In diabetic patients, elevated levels of TNF-alpha can engender insulin resistance and worsen glycemic control2. Therefore, in diabetic patients, decreasing TNF-alpha levels through periodontal and prosthetic therapy can restore insulin sensitivity and improve glycemic control. In a study29 of 13 type 2 diabetic subjects with periodontitis, periodontal therapy decreased TNF-alpha levels. In another study30 using rat model, the expression of interleukin-1beta, cyclooxygenase 2, and TNF-alpha tended to be elevated by trauma from occlusion, and thereby occlusal stabilization through prosthodontic therapy was expected to decrease TNF-alpha levels.
Recent randomized clinical trial27 examined the effect of periodontal treatment on the glycemic control and showed a reduction in HbA1c after 3 to 4 months of follow-up. There are insufficient data to show that this effect is maintained after 6 months or more.5 Within the limitation of retrospective study, we found a significant reduction in the HbA1c level (0.5%) in the treatment group after 13.1 months in average.
We noticed that active periodontal therapy was more effective in reducing HbA1c level than supportive periodontal therapy. This result could be due to the difference in mean interval of therapy. Active periodontal therapy had much shorter time interval than supportive periodontal therapy. We also noticed that the initial HbA1c level of supportive periodontal therapy group was much lower than that of active periodontal therapy group. Supportive periodontal therapy group had already been treated with active periodontal therapy before the initiation of supportive periodontal therapy, thus having lower initial HbA1c level from the beginning.
Prosthodontic therapy such as implant prosthesis, restoration, and removable partial denture could change the ecological system of the oral cavity possibly raising plaque accumulation at teeth.31 This could lead to bacteremia in the oral cavity and could exacerbate metabolic in diabetic patients. However, our results showed that periodontal and prosthodontic therapy group showed significant reduction in the HbA1c level, even more than periodontal therapy alone. This indicated that when periodontal therapy was performed together, prosthodontic therapy did not worsen glycemic control in patients with diabetes.
Polak and Shapira32 suggested a biological pathway that the elevated pro-inflammatory factors in the gingiva of patients with poorly controlled serum glucose may aggravate periodontitis. In this study, we examined the relationship between initial HbA1c and teeth loss rates in treatment group. Our study showed positive correlation between initial HbA1c and teeth loss rates and this result was statistically significant. This indicates that the severity of diabetes may affect the progression of periodontitis.
The retrospective design of this study presents inherent limitations. Not all HbA1c levels of patients were measured at the same time after periodontal and prosthodontic therapy. Another limitation is the inability to examine TNF-alpha levels after periodontal and prosthodontic treatment. Further studies are needed to examine TNF-alpha and C-Reactive Protein levels after periodontal and prosthetic treatment through randomized controlled design.
Go to :
 XML Download
XML Download