

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Epithelial ovarian cancer (EOC) is the second most common gynecologic cancer worldwide, and most cases (75–80%) are found in the advanced stage at the time of diagnosis. Even with the therapeutic advances of maximal debulking surgery and platinum-based chemotherapy, the survival rate in EOC remains poor. The overall 5-year survival rate was only approximately 40% following surgical and systemic chemotherapy treatments [1]. Recently, poly (ADP-ribose) polymerase inhibitors (PARPi) have been widely used in EOC patients carrying BRCA mutation, and information regarding BRCA1/2 mutations tends to be more important in the treatment of EOC.
BRCA1 and BRCA2 have significant roles in DNA repair mechanisms, and proteins encoded by the BRCA genes are necessary for homologous recombination-mediated DNA repair of double-strand breaks, which subsequently maintains DNA stability and prevents uncontrolled cell growth [2]. Interestingly, improved survival outcomes were reported in EOC patients with BRCA1/2 mutation compared to those with wild-type BRCA. Chemotherapy containing platinum, which is a cytotoxic agent causing DNA damage, shows a high response rate with improved survival in germline BRCA1/2 mutation carriers compared to sporadic ovarian cancers [34].
Although the status of BRCA1/2 mutations is important in clinical decision making and prognostication of EOC, there have been only a few studies with small sample sizes conducted in Asian populations including Korean patients. Some ovarian cancer studies with germline BRCA1/2 mutation have been analyzed in Korea, and 33% of patients with BRCA1/2 mutation had a family history of EOC. Patients with BRCA1/2 mutation had a longer overall survival (OS) than those with BRCA1/2 wild-type in Korea [567]. Another study showed that in advanced-stage high-grade serous ovarian cancer, patients with BRCA1/2 mutation had a longer progression-free survival (PFS) than those with BRCA wild-type [8].
In addition, the clinical characteristics or prognosis of EOC patients who have BRCA1/2 variant of unknown significance (VUS) have not been analyzed extensively, especially in Asian patients. A VUS is an identified DNA alteration not known to be deleterious and with unknown effects on protein function [9]. Patients diagnosed with BRCA1/2 VUS typically receive simple counselling and observation [710].
Therefore, the purpose of this study is to analyze the prevalence of and survival outcomes according to BRCA1/2 mutation status, including BRCA VUS, in Korean patients with EOC.
Materials and methods
1. Patients and study design
This was a retrospective cohort study performed in a single institution in Korea. Patients newly diagnosed with EOC between January 2007 and January 2017 were analyzed. Eligible patients included women who were newly diagnosed with EOC, either fallopian tube or primary peritoneal carcinoma; were rated as International Federation of Gynecology and Obstetrics (FIGO) stage I to IV; and underwent genetic BRCA testing. Women with high-grade serous carcinoma and those with mucinous, clear cell, low-grade serous or endometrioid, mixed epithelial adenocarcinoma, or undifferentiated carcinoma were included. The study was approved by Samsung Medical Center Institutional Review Board (IRB No. 2019-05-080-001).
2. BRCA1/2 mutation analysis
Genomic DNA was extracted from ethylenediaminetetraacetic acid-anticoagulated whole blood using the Wizard® Genomic DNA Purification Kit according to the manufacturer's instructions (Promega, Madison, WI, USA). Full sequencing of all coding exons and all adjacent exon/intron boundaries of BRCA1/2 was achieved using the Ion AmpliSeq™ BRCA1 and BRCA2 Panel (Life Technologies, Carlsbad, CA, USA) containing 167 primer pairs, and Ion AmpliSeq kit 2.0. The amplicons were clonally amplified through emulsion PCR using the IT OneTouch Template Kit 2.0 on an IT OneTouch system (Life Technologies) following the manufacturer's instructions. Targeted sequencing was performed using the Ion PGM platform with the Ion PGM sequencing 200 kit, following the manufacturer's instructions.
3. Treatment and follow-up
Patients underwent primary surgery followed by platinum-based combination chemotherapy or were treated with neoadjuvant chemotherapy followed by interval debulking surgery. After treatment, patients were followed up every 3 months for the first 2 years and then every 6 months for up to 5 years. Patients were monitored on the basis of clinical, biochemical, and imaging examinations. All clinical and pathologic data were collected through electronic chart review, including age at diagnosis, cancer antigen (CA)-125 level, residual disease status after primary cytoreductive surgery, histologic type, tumor grade, and FIGO stage. Surgical outcomes were categorized as either optimal if residual tumor size was less than 1 centimeter or suboptimal if it was the same or greater than 1 centimeter. PFS was defined as the period from the date of initial diagnosis to the date of progression or last follow-up. OS was defined as the length of time from either the date of diagnosis or the start of treatment for EOC in patients alive at the last follow up. BRCA testing results were categorized as BRCA mutation, wild-type, or VUS.
4. Statistical analysis
Categorical variables were compared between groups using the χ2 test. The Kaplan-Meier method with log-rank test was used to compare PFS and OS of wild-type vs. mutant groups. Statistical analysis was performed using R software (https://www.r-project.org/) version 3.2. A 2-sided P-value less than 0.05 was considered to be statistically significant.
Results
1. Prevalence of BRCA1/2 mutation
A total of 3,726 patients were treated at Samsung Medical Center between January 1, 2007 and January 1, 2017, and 313 patients (8.4%) who underwent the BRCA test were eligible for the current study. Of the 313 patients, 88 (28.1%) had a BRCA mutation. Fifty-seven patients (18.2%) had a BRCA1 mutation, while 31 patients (9.9%) had a BRCA2 mutation. In addition, 48 patients (15.3%) were identified with BRCA1/2 VUS. Among them, 27 patients (8.6%) had BRCA1 VUS, while 21 patients (6.7%) had BRCA2 VUS.
2. Patient characteristics
Patient characteristics were compared according to BRCA1/2 mutation and VUS, as shown in Tables 1 and 2. The median age at diagnosis was 49 years for BRCA1 mutation (range, 45–57 years) and 53 years for BRCA2 mutation (ranging from 48–58.5 years). Most patients showed serous type disease on histology. A larger proportion of patients with high-grade serous disease was observed in the BRCA1 mutation group (93.1%) than in the BRCA1 wild-type (81.1%) or BRCA1 VUS (65.5%) groups, but no significant difference based on BRCA status was observed. Similar patterns of histologic distribution were observed in BRCA2 mutations. The proportion of advanced stages (FIGO stage III/IV) did not differ among BRCA1 wild-type, BRCA1 mutation, and BRCA1 VUS groups (69.8% for BRCA1 wild-type, 73.2% for BRCA1 mutation, and 74.1% for BRCA1 VUS). In contrast, BRCA2 VUS patients showed a significantly larger proportion of FIGO stage IV than did the BRCA2 mutation and BRCA2 wild-type patients (14.9% in BRCA2 wild-type vs. 3.3% in BRCA2 mutation vs. 45% in BRCA2 VUS, P=0.002). Over 90% of the total patients had high-grade (grade 2 or 3) pathology, and no meaningful difference based on BRCA status was observed. There was no significant association between BRCA1 mutation and optimal primary debulking rate (73.4% for BRCA1 wild-type, 64.9% for BRCA1 mutation, 85.2% for BRCA1 VUS), and a similar pattern was observed for BRCA2 mutations.
Table 1
Patient characteristics by BRCA1 status
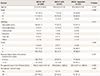
Values are expressed as median (range) or number (%).
WT, wild-type; VUS, variant of unknown significance; CA, cancer antigen.
![]()
Table 2
Patient characteristics by BRCA2 status
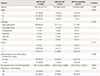
Values are expressed as median (range) or number (%).
WT, wild-type; VUS, variant of unknown significance; CA, cancer antigen.
![]()
CA-125 level before primary debulking surgery was not significantly different according to BRCA status.
Twenty-nine (9.2%) patients were treated with neoadjuvant chemotherapy followed by interval debulking surgery. The response rate of primary platinum-based chemotherapy in our study population was 89.1% (279/313). Among 88 patients who had a BRCA mutation, 26 (29.5%) were treated with PARPi.
Brief review of patient's characteristics between BRCA1 VUS and BRCA2 VUS were shown in Supplementary Table 1.
3. Survival outcomes
With a median follow-up duration of 19.8 months (ranging from 2–120 months), 193 patients showed disease progression, and 19 patients died due to EOC. Median PFS for BRCA1 wild-type, BRCA1 mutation, and BRCA1 VUS was 18.9, 23.0, and 19.1 months, respectively, and 19.4, 31.2, and 18.2 months for BRCA2 wild-type, BRCA2 mutation, and BRCA2 VUS, respectively. No significant difference was detected in terms of PFS between patients with BRCA1 mutation and BRCA1 wild-type or VUS (P=0.10, P=0.49, respectively) (Fig. 1A-C).
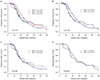 | Fig. 1Kaplan-Meier curves of progression-free survival (PFS) by BRCA1.
VUS, variant of unknown significance; wt, wild type; mut, mutation.
|
BRCA1 VUS did not show meaningful difference in PFS compared to BRCA1 mutation (P=0.87) (Fig. 1D). Regardless of BRCA1 mutation, there was no significant difference in OS (Supplementary Fig. 1A). In contrast, the presence of BRCA2 mutation was associated with longer PFS compared to BRCA2 wild-type (P=0.04) (Fig. 2A and B). The PFS curve of BRCA2 VUS showed no meaningful difference from that of BRCA2 wild-type (P=0.41) (Fig. 2C). The BRCA2 mutation group showed significantly higher PFS compared to BRCA2 VUS (P=0.02) (Fig. 2D). In contrast to PFS rates, there was no difference in OS between BRCA2 mutation (including VUS status) and BRCA2 wild-type (Supplementary Fig. 1B).
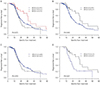 | Fig. 2Kaplan-Meier curves of progression-free survival (PFS) by BRCA2.
VUS, variant of unknown significance; wt, wild type; mut, mutation.
|
Brief review of clinical outcomes between BRCA1 VUS and BRCA2 VUS were shown in Supplementary Table 1.
Discussion
A number of previous studies have shown improved clinical outcomes in patients with BRCA1 or BRCA2 mutation compared to patients with wild-type BRCA in EOC [1112]. Those patients received platinum-based chemotherapy as a first-line standard therapy for ovarian cancer and showed improved outcomes with BRCA1 or BRCA2 mutation related to impairment in homologous recombination-mediated DNA repair. Other studies have shown that patients with BRCA2 mutation had improved OS and PFS compared to those with BRCA1 mutation [34]. However, such studies excluded BRCA VUS results and only focused on patients with BRCA1/2 mutation. Only a few reports have analyzed VUS prevalence in Asian patients. According to such studies, only about 7% of EOC patients had BRCA VUS [1314]. Until recently, there has been a paucity of evidence regarding the pathogenicity of BRCA VUS in EOC [15]. Some studies revealed that BRCA VUS should be treated as BRCA wild-type based solely on patient history, but clinical outcomes were not analyzed [1617]. Regarding BRCA mutation, the SOLO-2 study reported that platinum-sensitive, recurrent EOC patients have better PFS when treated with PARPi [18]. However, that study did not include patients with BRCA VUS, and further research is needed to determine the benefit of PARPi application in such patients.
This retrospective case-control study investigated baseline characteristics and clinical outcomes of EOC patients with BRCA1/2 mutation or VUS. The BRCA mutation rate was 28% in our study population, which is consistent with previously reported results ranging from 5% to 29% [51920212223242526]. The BRCA1/2 VUS rate was 15% (48/313). Favorable results regarding BRCA VUS were identified in this study, in that such patients did not show significant difference in PFS or OS compared to those with BRCA1 mutation or BRCA1 wild-type. Patients with BRCA2 VUS were significantly associated with lower median PFS compared to those with BRCA2 mutation. The strength of this study is inclusion of a large number of patients who underwent BRCA gene mutation testing. The present study is also valuable in that it is the first study comparing clinical outcomes of BRCA mutation to BRCA VUS according to subtype of EOC histology in the Korean population. This study provides clinical characteristics and survival outcomes of BRCA1/2 VUS in EOC patients and offers a good starting point for further research.
This study has several limitations. One of the limitations of this study is its retrospective nature. In patients with recurrent EOC, survival outcomes were not separated by chemotherapy duration. Due to a low death rate (19/313, 6.0%), the median OS of our study showed no meaningful difference in BRCA1/2 mutations or VUS. This is because many of the patients were diagnosed recently and had only a short follow-up time. When follow-up time is prolonged, there might be a significant difference in survival outcomes. In addition, only a small number of patients with BRCA1/2 mutation or VUS were enrolled, which can limit the significance of this study. Multi-center studies focusing on BRCA1/2 mutation and VUS are needed and may reveal differences in OS due to BRCA mutation or BRCA VUS.
In conclusion, our study shows similar patient demographics in BRCA mutation, wild-type, and VUS groups. When comparing survival outcomes, BRCA2 mutation showed improved PFS compared to BRCA2 wild-type or BRCA2 VUS. BRCA1 mutation did not produce significant difference in OS or PFS compared to BRCA wild-type.
 XML Download
XML Download