

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) is one of the oldest diseases known to mankind, and it is the leading cause of mortality worldwide. Although the incidence of TB has decreased, the TB incidence and mortality rates in Korea remain the highest among member countries of the Organisation for Economic Co-operation and Development, with an incidence of 70 cases/100,000 persons and a mortality rate of 4.9 cases/100,000 persons in 2017.1
Pulmonary TB (PTB) is a communicable infectious disease transmitted almost exclusively via aerosols produced when coughing.2 Treatment with anti-mycobacterial drugs greatly reduces the infectivity of PTB, whereas delays in diagnosis and treatment increase the risk of transmitting TB.3 However, diagnosis and isolation of patients with PTB are often delayed because the symptoms of TB are diverse and non-specific.
Historically, diagnosis of TB has been based on sputum smear microscopy to detect the presence of acid-fast bacilli (AFB) and, subsequently, TB has been diagnosed using cultures, based on the isolation of Mycobacterium tuberculosis (M. tuberculosis). However, AFB smears have a low sensitivity and specificity for diagnosing PTB, and culture results take several weeks.4 The recent introduction of Xpert MTB/RIF (Cepheid, Sunnyvale, CA, USA), a semi-automated nucleic acid amplification test, has improved the accuracy of TB diagnosis, and has resulted in shorter time to treatment initiation and isolation of patients with active TB.5
Delays in isolating patients admitted to hospital with active PTB can contribute to nosocomial transmission. However, in Korea, patients with clinically diagnosed PTB are not routinely isolated while awaiting microbiological confirmation of the diagnosis. This study aimed to assess the extent of delayed isolation of patients admitted with PTB, and the factors related to delays in isolating these patients.
METHODS
Study design and patients
This was a retrospective study of patients aged ≥ 18 years who had been admitted to two university-affiliated hospitals in Korea with active PTB between January 2008 and December 2017. The two hospitals were Seoul National University Bundang Hospital (1,300 beds), a tertiary referral hospital and Boramae Medical Center (800 beds), a secondary hospital. Inclusion criteria comprised patients with a diagnosis of active PTB, and microbiological confirmation of M. tuberculosis through culture test. Respiratory specimens used for diagnosis included sputum, endotracheal aspirates, and bronchoalveolar lavage.
Data collection and outcome measures
We retrospectively reviewed the patients' electronic medical records to identify factors associated with delays in isolating patients admitted with PTB. We extracted information on patients' age, gender, comorbidities, smoking history, symptoms, and the hospital department to which patients had been admitted. We also extracted information on radiological findings of PTB, such as apical infiltrates, cavitation, and tree-in-bud opacities.6 Delayed isolation was defined as a delay of one or more calendar days from the time of admission to isolation. We compared the characteristics of the patients with delayed isolation to those of patients who had been isolated on the day of admission to identify factors associated with a delay in isolation.
Statistical analysis
Chi-squared or Fisher's exact tests were used to test for statistical significance of comparisons between categorical variables, and the Mann-Whitney U-test was used to test for statistical significance of comparisons between continuous variables. Multivariable logistic regression analyses were used to identify factors associated with delays in isolating patients after admission. All factors associated significantly (P < 0.05) with delayed isolation on univariable analysis were included in the multivariable regression model. Statistical analyses were performed using SPSS for Windows (version 18 software package; SPSS, Inc., Chicago, IL, USA). In addition, we adopted a segmented regression method using open-source statistical software R, version 3.4.2 (http://www.R-project.org) to assess changes in the delay from admission to isolation over the study period.
RESULTS
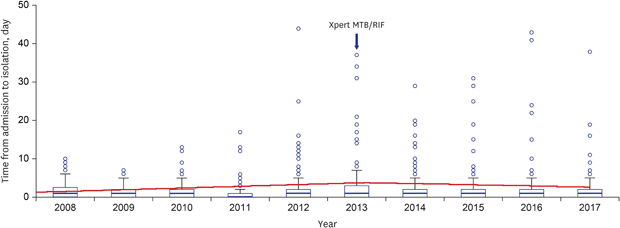
Of 1,062 patients diagnosed with PTB over the study period, 612 (57.6%) were not isolated on the day of admission. All patients had an AFB smear test, and 314 (29.6%) patients were tested with Xpert MTB/RIF. The median time from admission to isolation was 1 day (interquartile range, 0–2 days). The time from admission to isolation did not change significantly over the 10-year period (P = 0.361) (Fig. 1). However, there was a statistically significant decrease in the time from admission to isolation after 2013 when the Xpert MTB/RIF test was introduced in Korea (P = 0.007) (Fig. 1). Nonetheless, the Xpert MTB/RIF did not have a significant effect on the delays in isolation.
Fig. 1
Changes in the time from admission to isolation among patients with pulmonary tuberculosis over a 10-year period and in the period post-introduction of the Xpert MTB/RIF test in 2013.

The demographic and clinical characteristics of patients with immediate versus delayed isolation are compared in Table 1. Admission to a department other than a pulmonology or infectious diseases department was most strongly associated with delayed isolation. The chief complaints of patients admitted to the pulmonology and infectious diseases departments were symptoms suggestive of PTB, including cough, dyspnea and fever. On the other hand, the chief complaints of patients admitted to other departments were varied, and included general weakness, abdominal pain, surgical conditions, and trauma. Compared to patients with immediate isolation on admission, patients with delayed isolation had a higher median age (67 years) and a higher number of comorbidities including cardiovascular disease, chronic kidney disease, and malignancies. They were also less likely to have a history of previous TB, cigarette smoking, symptoms of active TB (including cough, sputum production, hemoptysis, night sweats, and weight loss), or to have signs of PTB (including apical infiltrates and cavities) on chest radiographs.
Table 1
Demographic and clinical characteristics of patients with delayed isolation compared to patients with immediate isolation

Data are presented as number (%) or median (interquartile range).
IQR = interquartile range, HIV = human immunodeficiency virus, TB = tuberculosis, CT = computed tomography, AFB = acid-fast bacilli.
aNumber of patients with chest CT: immediate isolation 391, delayed isolation 544; bNumber of patients with Xpert MTB/RIF: immediate isolation 121, delayed isolation 193.
Multivariable logistic regression analysis showed that the independent risk factor most strongly associated with delayed isolation was admission to departments other than those for pulmonology or infectious diseases (adjusted odds ratio [aOR], 5.302; 95% confidence interval [CI], 3.177–8.847; P < 0.001), and that the risk of delayed isolation increased with age (aOR, 1.016; 95% CI, 1.008–1.023; P < 0.001) (Table 2). Those with a past TB history (aOR, 0.669; 95% CI, 0.494–0.906; P = 0.009), night sweats (aOR, 0.530; 95% CI, 0.330–0.851; P = 0.009), and apical infiltrates on chest radiographs (aOR, 0.452; 95% CI, 0.276–0.740; P = 0.002) were more likely to be isolated on the day of admission.
Table 2
Results of univariable and multivariable logistic regression analyses of risk factors associated with delayed isolation among patients with pulmonary tuberculosis
DISCUSSION
Immediate isolation of patients with suspected PTB on admission is necessary to prevent nosocomial transmission of PTB.7 In this study, we found that > 50% of the patients subsequently diagnosed with active PTB had delayed isolation. Similar to the results of previous studies,89 admission to departments other than those for pulmonology or infectious diseases was associated with delayed isolation, and factors associated with isolation on the day of admission included the presence of a past history of TB, night sweats, and apical infiltrates on chest radiographs.
The incidence of TB in Korea remains the highest among high-income countries. The demographic shift towards an older population, many of whom have latent TB, affects TB control efforts in Korea.10 Preemptive isolation of patients with suspected PTB has been possible since 2007, due to the support of national health insurance. However, the isolation of patients admitted to hospital with active TB may be delayed in clinical practice because of factors associated with health care system, including the limited availability of single-occupancy rooms. Although it is desirable to preemptively isolate patients with pneumonia of unknown cause, it is difficult to implement preemptive isolation in the real world unless there is clear evidence of PTB. Many cases of nosocomial transmission of PTB have been reported in Korea.1112 Early diagnosis, isolation, and treatment are essential for an effective TB control program. The main factors associated with diagnostic delays have been reported to below levels of awareness regarding TB, poor access to healthcare, older age, human immunodeficiency virus (HIV) infection, extrapulmonary TB, and the coexistence of chronic cough and/or other lung diseases.1314 Okur et al.15 reported that the most common reasons for delays in diagnosis were a low index of suspicion for TB among physicians and the healthcare system, resulting in delays in referral. Similar to Rajagopalan's report,8 we found that delays in isolating patients with PTB increased with age. In Korea, 45.5% of newly diagnosed patients with TB in 2018 were aged 65 years or older, compared 10 years ago (27.5%).16 Many elderly patients with PTB may not exhibit the classic features, such as cough, night sweats, and weight loss. Atypical clinical manifestations of TB in elderly patients can result in delayed diagnosis and isolation.8 Therefore, a cautious approach is necessary, especially in elderly patients, even though their clinical manifestations seem to be non-specific for active PTB.
As in our study, previous studies have shown that among patients with PTB, changes in chest radiographs that are typical of PTB, such as apical infiltrates or cavitation on chest radiographs, are associated with a shorter time to isolation.1718 However, clinicians should be aware that, in immunocompromised hosts such as HIV-infected patients, it is difficult to distinguish between M. tuberculosis and other multiple pulmonary pathogens based on the patterns of radiographic infiltrates.19 Our study found a high proportion of patients with malignancies in the delayed isolation group. According to a 5-year national population-based study in Korea,20 in individuals with malignancies, the incidence of TB increased after diagnosis of the malignancy, and their risk of developing TB remained elevated 24 months after the cancer diagnosis. Their radiologic findings overlapped with those of patients with PTB or immunosuppression due to the malignancy itself or treatment such as chemotherapy might contribute to delays in isolation. As clinical differentiation may not be accurate, immediate isolation of patients suspected of having TB, without waiting for laboratory confirmation, is important for TB control. Recently, Han et al.21 reported that older age, malignancy, and hospitalization to a department other than a infectious diseases or pulmonology department was a risk factor for delayed isolation of PTB, and that radiologic diagnosis of active PTB was associated with early isolation. Conversely, a past TB history, night sweats, and apical infiltrates on chest radiographs were associated with early isolation. The elderly population in Korea has steadily increased, and the prevalence of PTB has also increased in this population. It is advisable to consider the possibility of PTB in elderly patients who have a past TB history, night sweats, or apical infiltrates on chest radiographs.
The Xpert MTB/RIF assay is a rapid and accurate nucleic acid amplification test for the diagnosis of PTB, and provides substantial clinical and economic benefits.45 Chaisson et al.22 have proposed that new guidelines that incorporate the use of Xpert MTB/RIF be developed to guide TB diagnostic evaluation and discontinuation of respiratory isolation. Although the use of Xpert MTB/RIF can reduce the time to isolation of patients with PTB as it reduces delays in microbiological confirmation, the Xpert MTB/RIF did not have a significant effect on the early isolation of patients with PTB in our study. Therefore, all patients with suspected PTB should be placed in airborne isolation immediately on admission, and then tested for PTB with AFB smear microscopy and Xpert MTB/RIF.
Our study had some limitations. As the study data were collected retrospectively, other important clinical variables that contribute towards delays in isolation may have been missed. In addition, our study may not be generalizable to all patients hospitalized with PTB in Korea because it only included TB patients admitted to two university-affiliated hospitals. However, hospitals in Korea do not routinely isolate patients with suspected TB on admission, and the study hospitals included both a secondary hospital and a tertiary referral hospital, making our results broadly applicable to other hospitals in Korea.
We found that > 50% of the patients subsequently diagnosed with active PTB were not isolated immediately upon admission to hospital. To minimize delays in isolation, clinicians should be vigilant against the elderly patients who have a past TB history, complaints of night sweats, or apical infiltration on chest radiographs. We suggest that all patients with clinically suspected PTB be presumptively isolated on admission until the possibility of PTB is excluded, based on microbiological test results.
 XML Download
XML Download