

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The TNM system of the American Joint Committee on Cancer/International Union Against Cancer Classification (AJCC/UICC) has been revised every few years. The 7th system was introduced in 2010, and there were some changes from 6th system: 1) T2a (tumor invades muscularis propria), T2b (tumor penetrates subserosal connective tissue without invasion of visceral peritoneum or adjacent structures), T3 (tumor invades serosa), and T4 (tumor invades adjacent structures) in the 6th system were redefined as T2, T3, T4a, and T4b in the 7th system, respectively; 2) N1 (metastasis in 1–6 regional nodes) in the 6th system had been divided into N1 (metastasis in 1–2 regional nodes) and N2 (metastasis in 3–6 nodes); 3) N2 (metastasis in 7–15 regional nodes) and N3 (metastasis in more than 15 regional nodes) in the 6th system had been redefined as N3a and N3b in the 7th system, respectively; and 4) positive peritoneal lavage cytology is classified as M1 (distant metastasis) [12].
In the 6th system, gastric cancer patients with lymph node metastasis more than 15 (LNM>15) were classified as stage IV, which had been reclassified as localized disease (stage IIb, IIIa, IIIb, or IIIc) in the 7th system [12]. Meanwhile, even though N3 was sub-classified into N3a (LNM 7–15) and N3b (LNM>15), these sub-classifications of N3 were not adapted in the final 7th system [1]. Hence, there was much debate on the prognosis of patients with N3a and N3b cancer, who were classified to the same stages [3456]. However, in the 8th system, which has been applied since 2018, the sub-classifications of N3 were finally adapted in the final staging system [7]. There is a tendency that N3b patients are prone to be classified into more advanced TNM stages, especially stage IIIc. However, N3b patients were still regarded as the localized disease. Meanwhile, the peritoneal washing cytology-only positive (CY1-only) patients had better overall survival than those with either overt distant metastasis-only or both overt distant metastasis and cytology-positive disease [8910].
Patients with localized disease have been considered for targets of neoadjuvant or adjuvant chemotherapy regimens, which are relatively limited comparing to those of palliative regimens. Results of previous studies showing that some stage IIIc gastric cancer patients with N3b showed comparable survival rates to those of patients with stage IV remained controversial [111213], which should be taken into account when treating patients with N3b.
In this study, we compared the overall survival (OS), 5-year survival rate (5YSR), and recurrence-free survival (RFS) of patients with 1) stage IIb, IIIa, IIIb, IIIc, and IV based on the 7th and 8th systems, as well as those of 2) “pure N3b” patients who underwent radical gastrectomy, CY1-only stage IV cancer patients, and grossly stage IV patients. We aimed to determine whether the survival of N3b patients who underwent radical gastrectomy is comparable to that of CY1-only patients who are literally stage IV by definition. Furthermore, we aimed to propose a new TNM staging system interpreting N3b as an eligibility criterion for classifying together with CY1-only stage IV. Moreover, we aimed to suggest the usability of more intensive chemotherapy regimens as an adjuvant therapy for N3b patients as if they are palliative disease.
MATERIALS AND METHODS
Patients
A total of 4,809 patients who underwent gastric cancer surgery at the Department of Surgery, Seoul National University Hospital (SNUH) from January 2007 to December 2012 were included in the study. Patients inclusion criteria were as follows: 1) patients with pathologically confirmed gastric adenocarcinoma, 2) patients whose stage IIb–IIIc cancer was confirmed after surgery based on the 7th system, and 3) patients with stage IV who underwent non-resection surgery. Patients exclusion criteria were as follows: 1) patients who were aged less than 18 years, 2) patients who underwent gastrectomy with 15 or fewer retrieved lymph nodes (LNs), and 3) patients who received preoperative neoadjuvant chemotherapy. After retrospectively reviewing the electronic medical records (EMRs) of 4,809 patients, 3,379 patients were excluded and only 1,430 were included in the study.
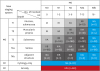
The 6th, 7th, and 8th staging systems are shown in Fig. 1. Besides the AJCC staging system, we defined a new categorization system to evaluate the genuine effect of LNM on survival irrespective of the T stage. Based only on the N classification, we re-classified the patients into N0-2 (LNM<7), N3a (LNM 7–15), and N3b (LNM>15).
 | Fig. 1AJCC staging systems. Shown are the 6th (top), 7th (middle), and 8th (bottom) AJCC staging system.AJCC = American Joint Committee on Cancer; LN = lymph node.
|
The variables included in the data were age, sex, types of operation (distal, total, proximal, pylorus-preserving, non-resection, or others), pathological characteristics (differentiation, Lauren classification, presence of residual disease, lymphatic invasion, venous invasion, perineural invasion, T classifications, and N classification), and peritoneal washing cytology [1415]. The T classification, N classification, and staging of cancer were classified according to the 7th and 8th systems [17].
Treatment methods
Curative resections of the primary tumor were performed after the evaluation, which confirmed to be the absence of distant metastases. The resection and lymphatic dissection were performed in accordance with the standard guidelines, which mainly includes D1+ dissection for clinically early gastric cancer (EGC) and D2 dissection for clinically advanced gastric cancer (AGC) [1617].
Among the stage IV patients (n=371), 171 underwent palliative resection. Lymphatic dissection for palliative resections primarily includes D2 dissection (n=131, 76.6%) followed by D1+ (n=23, 13.5%) and D1 dissection (n=17, 9.9%). The remaining 200 patients underwent non-resection surgery (gastrojejunostomy, biopsy, and jejunostomy) without lymphatic dissection.
Postoperative adjuvant chemotherapy was administered based on the adjuvant chemotherapy trial of TS-1 for gastric cancer (ACTS-GC) [18] and adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC) trial [19]. Before these trials, fluorouracil-based combinations were widely used [20].
The follow-up surveillance after surgery for involved patients were as follows: 1) the patients were required to visit the outpatient clinic every 3–4 months during the first 2-year period, and every 6 months for 2 years thereafter; 2) tumor markers (carcinoembryonic antigen; CEA and carbohydrate antigen 19-9; CA 19-9) were checked every follow-up examination; 3) computed tomography (CT) and/or ultrasonography was performed every 6 months; and 4) endoscopy was performed every year [16]. Follow-up was continued for at least 5 years (mean follow-up, 46.62±36.48 months) after which the patients were recommended to undergo surveillance by general physicians or health care programs [16].
The survival status was checked through the EMR by confirming the date of last follow-up or death before and after 5 years for every patient one by one until June 2018. Some uncertain survival status due to follow-up loss was supplemented with the data from the Ministry of the Interior and Safety.
Intraoperative peritoneal washing cytology
After accessing the peritoneal cavity, either through open or laparoscopic surgery, exploration was performed to confirm the operability of the tumor. If any peritoneal fluid was found, it was aspirated and sent to experienced pathologists for evaluation. If only a scanty amount of peritoneal fluid was found, which was not enough for cytology evaluation, 200 mL of normal saline was used to rinse the pelvic cavity (100 mL) and the left subphrenic cavity (100 mL) [21].
While positive peritoneal washing cytology is included in the 7th system as M1 disease [1], we performed peritoneal washing cytology selectively in patients who were highly suspected of having overt peritoneal metastasis. This procedure has become a part of the routine evaluation in clinically AGC patients since 2016.
New TNM staging system
To compare the OS of the “pure N3b” group with that of the CY1-only group, we separated the N3b patients from other stages, and only T4bN3a patients (n=4) were left in the stage IIIc (Fig. 1). We evaluated the OS of patients with IIb–IIIc, N3b, CY1-only stage IV, and grossly stage IV and the RFS of those with IIb–IIIc and N3b in order to suggest a new TNM staging besides the 8th staging system.
Statistical analyses
OS was defined as the period between the date of surgery and the date of death, or the date of last follow up. If the patients did not visit the outpatient department before confirming that they had no evidence of disease (NED) for 5 years, we defined them as “follow up loss.”
RFS was defined as the period between the date of surgery and the date of first-documented disease recurrence by any modality (e.g., ultrasonography, computed tomography, positron emission tomography, or esophagogastroduodenoscopy). Data of patients who had been originally diagnosed as stage IV were censored. The 3-year RFS and the mean RFS were evaluated.
The SPSS software 23.0 was used for the analysis. The OS, 5YSR, and RFS were analyzed based on the 7th and 8th systems, as well as the new categorization using the Kaplan-Meier method. Heterogeneity in the OS and RFS of each group was compared using the log-rank test. A P-value of less than 0.05 was considered to be statistically significant.
Ethical approval
The data collection and analysis of this study were approved by the Institutional Review Board (IRB) of the Seoul National University Hospital. The written informed consent of patients was not required in accordance with IRB regulation because of the retrospective design of the study (IRB No.: H-1709-018-882).
RESULTS
Patient features
We evaluated 1,430 out of 4,809 patients who underwent gastric cancer surgery from January 2007 to December 2012. The flow diagram of patient extraction is shown in Fig. 2.
 | Fig. 2Patients extraction.TNM = tumor, node, metastasis.
*The patient count number can be duplicated when extracted; †Ten of 32 patients had cytology-only positive (CY1-only) disease.
|
The clinicopathological characteristics of these patients are summarized in Table 1. The mean age of the patients was 60.21±12.34 years, and the male to female ratio was 949/481. Peritoneal washing cytology was performed in 161 patients. Among them, the number of patients in stage IIb, IIIa, IIIb, IIIc, and IV was 23, 8, 29, 13, and 88 respectively. A total of 32 patients had cytology-positive (CY1) stage IV, while 10 out of 32 patients had CY1-only stage IV.
Table 1
Patient baseline characteristics

Values are expressed as mean±standard deviation or number (%).
*Gastrojejunostomy, biopsy, or feeding jejunostomy; †Papillary adenocarcinoma, well-differentiated tubular adenocarcinoma, and moderately-differentiated tubular adenocarcinoma; ‡Poorly differentiated adenocarcinoma, mucinous adenocarcinoma, and signet ring cell carcinoma; §Indeterminate, undifferentiated carcinoma, adenosquamous carcinoma, or mixed type; ∥Indeterminate; ¶There were 10 cytology-only positive (CY1-only) patients out of 32 patients.
![]()
Table 2 summarizes the recurrence patterns in 1,059 patients with localized disease, except stage IV patients. A total of 404 patients developed disease recurrence, while 655 had absence of disease recurrence.
OS
According to the 7th system, the 5YSR was 76.4% for stage IIb (n=306), 63.5% for stage IIIa (n=266), 50.1% for stage IIIb (n=259), 29.6% for stage IIIc (n=228), and 8.3% for stage IV (n=371). Significant differences were observed in the OS curves of each group (Fig. 3A).
 | Fig. 3OS curves. Shown are the OS curves of the (A) 7th and (B) 8th systems, as well as the new categorization based on (C) the N classification; N3b patients separated from (D) other stages and (E) T1–T4bN3b.OS = overall survival.
|
According to the 8th system, the 5YSR was 76.4% for stage IIb (n=302), 60.3% for stage IIIa (n=349), 48.5% for stage IIIb (n=263), 22.3% for stage IIIc (n=145), and 8.3% for stage IV (n=371). The OS curves of each group were significantly different (Fig. 3B).
Fig. 3C shows the evaluation process according to the new categorization based on the N classification. The 5YSR was 67.5% for N0-2 (n=604), 51.4% for N3a (n=304), 24.1% for N3b (n=151), 40% for CY1-only stage IV (n=10), and 7.4% for grossly stage IV (n=361). The log rank test showed the p values of 1) OS between N3a and CY1-only stage IV (P=0.052) and those between 2) N3b and CY1-only stage IV (P=0.671). There was a more similar survival tendency between N3b and CY1-only stage IV rather than between N3a and CY1-only stage IV. The OS curve of N3b is significantly different from that of grossly stage IV (P<0.001)
We analyzed the OS of IIb–IIIc, N3b, CY1-only stage IV, and grossly stage IV (Fig. 3D). The 5YSR was 48.3% for stage IIIb (n=253), 25.0% for stage IIIc (n=4), 24.1% for N3b (n=151), 40.0% for CY1-only stage IV (n=10), and 7.4% for grossly stage IV (n=361). The OS curve of the remaining patients with stage IIIc (T4bN3a) was comparable to that of the patients with N3b and CY1-only stage IV. OS curves of these 3 groups were distinct from those with grossly stage IV.
We analyzed the OS of T1–T4bN3b, CY1-only stage IV, and grossly stage IV (Fig. 3E). The 5YSR was 60.0% for T1N3b (n=5), 37.5% for stage T2N3b (n=5), 29.7% for T3N3b (n=38), 19.3% for T4aN3b (n=98), 20.0% for T4bN3b (n=5), 40.0% for CY1-only stage IV (n =10), and 7.4% for grossly stage IV (n=361). The log rank test showed that the differences of OS curves among T1–T4b are insignificant. They showed similar trends to CY1-only stage IV but showed distinct trends from grossly stage IV.
RFS
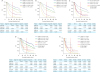
The 3-year RFS and the mean RFS were analyzed. According to the 7th system, the 3-year RFS was 89.3% for stage IIb (n=306), 78.4% for stage IIIa (n=266), 65.8% for stage IIIb (n=259), and 49.6% for stage IIIc (n=228). The mean RFS was 114.9 months for stage IIb (95% confidence interval [CI], 109.2–120.6), 95.2 months for stage IIIa (95% CI, 88.6–101.8), 81.3 months for stage IIIb (95% CI, 74.3–88.3), and 56.2 months for stage IIIc (95% CI, 49.4–62.9). The RFS curves of each group were significantly different (Fig. 4A).
 | Fig. 4RFS curves. Shown are the RFS curves reported in the (A) 7th and (B) 8th systems, as well as the new categorization based on (C) the N classification; N3b patients separated from (D) other stages and (E) T1–T4bN3b.RFS = recurrence-free survival.
|
According to the 8th system, the 3-year RFS was 89.9% for stage IIb (n=302), 75.4% for stage IIIa (n=349), 64.2% for stage IIIb (n=263), and 42.3% for stage IIIc (n=145). The mean RFS was 115.5 months for stage IIb (95% CI, 109.7–121.2), 91.2 months for stage IIIa (95% CI, 85.3–97.0), 78.1 months for stage IIIb (95% CI, 71.2–85.0), and 47.8 months for stage IIIc (95% CI, 87.0–94.4). The RFS curves of each group were significantly different (Fig. 4B).
We also evaluated the RFS based on the N classification. The 3-year RFS was 81.7% for stage N0-2 (n=604), 67.4% for N3a (n=304), and 44.5% for N3b (n=151). The mean RFS was 104.0 months for N0-2 (95% CI, 99.4–108.6), 82.0 months for N3a (95% CI, 75.6–88.5), and 49.1 months for N3b (95% CI, 41.4–56.8). The RFS curves of each group showed significant differences (Fig. 4C).
We analyzed the RFS of IIb–IIIc and N3b. The 3-year RFS were 89.9% for stage IIb (n=302), 75.4% for stage IIIa (n=349), 63.8% for stage IIIb (n=253), 33.3% for stage IIIc (n=4), and 44.5% for N3b (n=151). The mean RFS was 115.5 months for stage IIb (95% CI, 109.7–121.2), 91.2 months for stage IIIa (95% CI, 85.3–97.0), 78.0 months for stage IIIb (95% CI, 71.0–85.0), 51.3 months for stage IIIc (95% CI, 16.0–86.6), and 49.1 months for N3b (95% CI, 41.4–56.8). The RFS curve of N3b was significantly different from that of stage IIb, IIIa, and IIIb, but was similar to that of the remaining IIIc (Fig. 4D).
We analyzed the RFS of T1–T4bN3b. The 3-year RFS were 60.0% for T1N3b (n=5), 0.0% for stage T2N3b (n=5), 43.8% for T3N3b (n=38), 42.0% for T4aN3b (n=98), and 40.0% for T4bN3b (n=5). The mean RFS was 62.0 months for stage T1N3b (95% CI, 33.7–90.2), 54.8 months for T2N3b (95% CI, 46.2–63.4), 56.0 months for T3N3b (95% CI, 40.2–71.6), 43.1 months for T4aN3b (95% CI, 34.5–51.7), and 33.9 months for T4bN3b (95% CI, 7.9–60.0). No significant differences were observed among the RFS curves of T1–T4bN3b (Fig. 4E).
Proposal of a new TNM staging system
We have found out some trends after performing the evaluations: 1) OS of N3b was comparable to that of CY1-only stage IV, but distinct from that of grossly stage IV; 2) after separating patients with pure N3b other stages, OS of the remaining patients in stage IIIc (T4bN3a, n=4) was comparable to that of patients with N3b and CY1-only stage IV; 3) the differences in OS and RFS curves among T1–T4bN3b are insignificant, and OS curves of T1–T4bN3b were similar trends to that of CY1-only stage IV, but distinct from that of grossly stage IV; and 4) most of the N3b patients had significantly shorter 3-year RFS and mean RFS than those with IIb–IIIc, as if N3b itself was a higher TNM stage.
Based on these findings, we have proposed a new staging system; that is, the remaining stage IIIc (T4bN3a), N3b, and CY1-only stage IV were unified as an individual stage, which is stage IVa. Grossly stage IV was consequently categorized as stage IVb (Fig. 5).
DISCUSSION
In the 6th edition of AJCC TNM staging system, gastric cancer with lymph node metastasis more than 15 (which means the number of lymph node metastasis is 16 or more) were defined as stage IV irrespective of the T stage [2]. In the 7th system, which was introduced in 2010, it was reclassified as stage IIb–IIIc [1], and this concept has been retained in the 8th system as well [7]. This means that the patients with LNM more than 15 were no longer eligible for palliative therapy.
The survival curves for all stages according to the 7th and 8th systems were significantly different. Interestingly, despite these significant differences in statistics, the survival trends for stage IIIc and stage IV were more similar in the 8th system than in the 7th system. This was probably due to the reclassification of N3b gastric cancer patients more purely into the stage IIIc group; the proportion of N3b patients in stage IIIc was 103 out of 228 (45.18%) in the 7th system and 141 out of 145 (97.24%) in the 8th system.
Considering this assumption, we defined a new categorization based on N classification to evaluate the genuine effect of lymph node metastasis. We compared the survival of patients with N0-2, N3a, N3b, CY1-only stage IV, and grossly stage IV. The survival trend of pure N3b patients were very similar to that of CY1-only stage IV patients, but were different from that of grossly stage IV.
We analyzed the survival of patients with IIb–IIIc, N3b, CY1-only stage IV, and grossly stage IV. After separating the N3b patients from other stages, only four patients, whose staging were T4bN3a, were left in the stage IIIc group. We found that the survival of T4bN3a patients was comparable to that of patients with N3b and CY1-only stage IV. Survival trends of these three groups were distinct from that of the grossly stage IV group.
Survival analysis was performed in patients with T1–T4bN3b, CY1-only stage IV, and grossly stage IV. OS of patients with T1–T4bN3b was homogeneous irrespective of T stage according to log rank test and comparable to that of CY1-only stage IV, but was distinct from that of patients with grossly stage IV. Even if the number of patients with T1N3b, T2N3b, and T4bN3b was quite small, T1–T4bN3b were homogeneous according to log rank test and eventually showed dismal prognosis based on the statistic evaluation. Hence, it was appropriate to group them in the same stage.
Most of the 3-year RFS and the mean RFS showed high likelihood of inverse relation with TNM stage. After separately classifying the N3b patients from other stages, results showed that N3b patients had significantly shorter 3-year RFS and mean RFS, as if N3b itself was a higher TNM stage.
We have finally proposed a new staging system with the aforementioned findings: 1) OS of N3b was comparable to that of CY1-only stage IV, but was distinct from that of grossly stage IV; 2) OS of the remaining stage IIIc patients (T4bN3a) was comparable to that of patients with N3b and CY1-only stage IV; 3) N3b patients showed homogeneous survival and RFS irrespective of T stage (T1–T4b), and were appropriate to be grouped in the same stage; and 4) N3b patients showed significantly shorter RFS than those with IIb–IIIc, as if N3b itself was a higher TNM stage.
In the aspect of survival difference between CY1-only stage IV and grossly stage IV, we divided stage IV into two subcategories, IVa and IVb. The remaining stage IIIc (T4bN3a), N3b, and CY1-only stage IV were unified as stage IVa, while grossly stage IV was consequently defined as stage IVb. The classification of subdivisions of each stage is simplified intuitively: Ia, Ib, IIa, IIb, IIIa, IIb, IVa, and IVb.
This study had a few limitations. First, the study was retrospective in nature and was based on the data from the EMRs. Second, because the concept of cytology was applied in the final staging system only since the introduction of the 7th system in 2010 and peritoneal washing cytology was previously performed in limited cases only (e.g., advanced cancer suspected of overt peritoneal seeding), the number of CY1-only stage IV patients was small. Due to the small sample size, there were unexpected outlying values of 5YSR, 3-year RFS, and mean RFS. Hence, a multicenter study is necessary to overcome this drawback. Third, separation of patients with pure N3b from other stages resulted in a dramatic decrease in the number of patients with stage IIIc, leaving only four patients whose TNM staging was T4bN3a, which also resulted in outlying values. This problem can also be handled by multicenter cooperation. Fourth, any underlying diseases of patients were not considered during the evaluation. Finally, all survival data were based on all-cause mortality, not disease-specific mortality.
To date, patients with localized disease have been considered for neoadjuvant or adjuvant chemotherapy with limited regimens, while those with positive peritoneal washing cytology and/or distant metastases have been considered for relatively wide variety of more intensive chemotherapy regimens. Some trials, of which subjects are the patients with unresectable advanced gastric cancer or unresectable recurrence, suggested the usability of various intensive chemotherapy regimens [22232425].
Our analysis showed that the survival of pure N3b patients who underwent radical gastrectomy is comparable to that of CY1-only stage IV patients, which is literally stage IV by definition.
In conclusion, we proposed a new TNM staging system interpreting N3b as an eligibility criterion for classifying together with CY1-only stage IV; hence, we suggest the usability of more intensive chemotherapy regimens as an adjuvant therapy for N3b patients as if they are palliative disease. We did not aim to insist that N3b patients were not targets for surgery, but we focused on the manner of administering chemotherapy with this dismal disease.
 XML Download
XML Download