

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The elderly population has increased globally, and the incidence of patients with geriatric cancer has also significantly increased [1]. In Korea, the number of elderly patients with gastric cancer aged ≥70 years has been steadily increasing, from 9.1% in 1995 to 25.3%, in 2014 [2]. The number of elderly patients with gastric cancer undergoing gastrectomy has also increased because surgical resection is the only curative treatment method for gastric cancer [2].
Many studies have investigated risk factors for complications after gastrectomy, and old age is a risk factor for postoperative morbidity and mortality [3]. The prevalence of malnutrition has been ranging from 35% to 65% in hospitalized geriatric patients [4], and the malnourished state has a negative impact on the body's defensive system and is associated with adverse clinical manifestations such as a prolonged hospital stay, higher postoperative complications, delayed recovery of bowel function, higher readmission rate, and lower survival rate [56].
To detect malnutrition in patients with cancer, a variety of screening tools are used. Commonly used tools are Nutritional Risk Screening (2002), Mini Nutritional Assessment, Subjective Global Assessment, Nutritional Risk Index, serum albumin, and body mass index (BMI). However, these nutritional assessment methods have disadvantages in that they are based on subjective items, such as the amount of food consumed based on patient's description, or they may be influenced by confounding variables. Thus, there is no golden standard method to date.
Bioelectrical impedance analysis (BIA) is an objective, quick, safe, reproducible, and noninvasive method to evaluate body composition. BIA measures body component resistance and reactance by recording a voltage drop in the applied current [7]. Resistance is the restriction to the flow of an electric current, primarily related to the amount of water present in tissues. Cell membranes produce capacitance (reactance) by storing parts of the charge as a capacitor [8]. This storage of the current creates a phase shift, which is quantified geometrically as the angular transformation of the ratio of reactance to resistance, or the phase angle [9]. Geometrical relationships among impedance, reactance, resistance, and phase angle are illustrated in Fig. 1 [7].
 | Fig. 1Geometrical relationship between impedance (Z), reactance (Xc), resistance (R), and phase angle (PA).
|
Phase angle reflects the relative contributions of fluid (resistance) and cellular membranes (reactance) of the human body, and is positively associated with reactance and negatively associated with resistance [9]. Phase angle can be interpreted as an indicator of water distribution between the extra- and intra-cellular spaces, one of the most sensitive indicators of malnutrition [10]. Low phase angle suggests cell death or decreased cell integrity, while high phase angle suggests large quantities of intact cell membranes and body cell mass [11]. Phase angle has been used as a nutritional indicator in different patient groups [121314], and has been associated with malnutritional risk, morbidity, and mortality in patients with various cancer [151617].
In this study, we evaluated the relationship between complications after gastrectomy and various risk factors for postoperative complications, including phase angle in elderly patients with gastric cancer.
MATERIALS AND METHODS
Patients
We retrospectively reviewed data from 210 patients aged ≥65 years who had undergone total or distal gastrectomy for primary gastric cancer at Kyungpook National University Chilgok Hospital from August 2016 to August 2017. Patients who did not undergo preoperative BIA were excluded. Moreover, patients who completed total gastrectomy, Whipple's procedure, palliative gastrectomy, or neoadjuvant chemotherapy were excluded from the study. The study was approved by the Institutional Review Board of Kyungpook National University Chilgok Hospital (approval number: 201807016).
Clinical analysis
Clinicopathological data including age, sex, BMI (calculated as body weight/height2), American Society of Anesthesiology (ASA) classification, comorbidity, hemoglobin level (<13 g/dL for males and <12 g/dL for females was defined as anemia), serum albumin level (<3.5 g/dL was defined as hypoalbuminemia), prognostic nutritional index (PNI: 10×serum albumin [g/dL]+0.05×total lymphocyte count [103/µL]) score, neutrophil/lymphocyte ratio (NLR), and the phase angle were obtained from our medical database records.
All patients scheduled for gastric cancer surgery in our hospital undergo BIA using InBody720 (Biospace, Seoul, Korea) to assess preoperative body composition. With InBody720, we can only acquire the value of reactance (Xc) and resistance (R). Therefore, we calculated the whole body phase angle using the following formula:
InBody720 measures impedance by using 6 different frequencies, but in most previous studies for several clinical conditions, including cancer, the phase angle at 50 kHz has been shown to be predictive for prognosis; thus, we used the phase angle at the frequency of 50 kHz in this study [1819].
Morbidity and mortality within 30 days after the procedure were evaluated. Postoperative complications were defined as any deviation from the standard postoperative clinical pathway in our department requiring conservative or surgical treatment and graded according to the Clavien-Dindo (CD) classification [20]. All patients who underwent grade I complications did not require additional medication or treatment, hence grade I complications were excluded in this analysis. CD grade II or higher was considered as overall complication and CD grade III or higher were considered as severe complication. Clinical and pathologic cancer staging was based on the 7th American Joint Committee on Cancer staging system.
Statistical analysis
Statistical analysis was performed using SPSS® version 23.0 (SPSS Inc., Chicago, IL, USA). The χ2 test and Fisher's exact test were used to compare categorical variables, and the Student t-test was used to compare continuous variables. Receiver operating characteristic (ROC) curve analysis was used to obtain the cut-off value of nutritional indices, which did not determine standard reference values. A logistic regression model was used for multivariate analysis. P<0.05 was considered statistically significant. Significant risk factors identified with univariate analysis were further assessed using multivariate analysis with backward elimination.
RESULTS
Clinicopathological characteristics of the 210 patients are shown in Table 1. Patient mean age was 72.9 years, and 73 patients were ≥75 years. There were 143 men (68.1%) and 67 women (31.9%). The mean BMI was 23.9 kg/m2. Twenty-seven patients (12.9%) had an ASA score of 3, and 81 patients (38.6%) had two or more comorbidities. Eighty-five patients (40.5%) had preoperative anemia (reference value: 11.0–17.0 g/dL), and hypoalbuminemia (reference value: 3.5–5.2 g/dL) was noted in 16 patients (7.6%). A comparison between the high- and low-phase angle groups showed statistically significant differences in BMI, albumin, PNI score, and NLR, which are nutritional indices, between the groups (Table 2). All nutritional indices were similar to the phase angles; thus, the phase angle was considered to reflect the nutritional status of patients (Table 2).
Table 1
Clinical and surgical characteristics of patients

Values are presented as mean ± standard deviation or number (%).
BMI = body mass index; ASA = American Society of Anesthesiologists; PNI = prognostic nutritional index; NLR = neutrophil/lymphocyte ratio; JP = Jackson-Pratt.
![]()
Table 2
Nutritional status between the high- and low phase angle groups

| Variable | High phase angle | Low phase angle | P-value |
|---|---|---|---|
| BMI | 24.82±2.97 | 22.89±3.50 | <0.001 |
| Albumin (g/dL) | 4.07±0.22 | 3.84±0.40 | <0.001 |
| PNI score | 50.21±4.14 | 46.63±5.44 | 0.004 |
| NLR | 2.18±1.88 | 2.87±1.43 | <0.001 |
Values are presented as mean ± standard deviation. High phase angle, phase angle ≥4.19° for females and ≥4.87° for males; low phase angle, phase angle <4.19° for females and <4.87° for males.
BMI = body mass index; PNI = prognostic nutritional index; NLR = neutrophil/lymphocyte ratio.
![]()
All nutritional indices showed significant differences between patients with and without complications (Table 3). There is no standard cutoff value for these indices, thus ROC curve analysis was used to compare the prognostic ability of these variables for each complication according to the area under the curve (AUC) based on the maximum of the Youden index (sensitivity+specificity−1) (Fig. 2). The AUC of the PNI score, NLR, phase angle for males, and phase angle for females were 0.634 (95% confidence interval [CI], 0.544–0.724; P=0.002), 0.614 (95% CI, 0.525–0.702; P=0.010), 0.713 (95% CI, 0.615–0.810; P<0.001), and 0.639 (95% CI, 0.490–0.789; P=0.075), respectively. The cut-off values of PNI score, NLR, phase angle for males, and phase angle for females were 48.2, 2.15, 4.87°, and 4.19° respectively. Low PNI score, low NLR, and low phase angle were noted in 93 (44.3%), 113 (53.8%), and 92 (43.8%) patients, respectively. The percentage of clinical early gastric cancer (EGC) was 64.2%.
Table 3
Nutritional status between the complication- and non-complication groups

Values are presented as mean ± standard deviation.
BMI = body mass index; PNI = prognostic nutritional index; NLR = neutrophil/lymphocyte ratio.
![]()
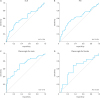 | Fig. 2Receiver operating characteristics curve showing the sensitivity and specificity of the nutritional indices for predicting postoperative complications: (A) NLR, (B) PNI, and phase angle for male (C) and female (D) individuals.AUC = area under the curve; NLR = neutrophil/lymphocyte ratio; PNI = prognostic nutritional index.
|
Postoperative complications are shown in Table 4. A total of 61 patients had complications. The most common complication was intra-abdominal or pulmonary infection requiring antibiotic therapy. Seven patients had tachyarrhythmia requiring medical treatment and four patients had postoperative ileus or obstruction requiring fasting and total parenteral nutrition. Fifteen patients were managed with radiological or endoscopic intervention and five patients underwent surgery under general anesthesia.
Table 4
Postoperative complications according to the Clavien-Dindo classification

![]()
In univariate analysis, age ≥75 years (P=0.005), high ASA score (P<0.001), presence of 2 or more comorbidities (P=0.001), anemia (P=0.004), hypoalbuminemia (P=0.001), low PNI score (P=0.002), low NLR (P=0.017), low phase angle (P<0.001), total gastrectomy (P=0.002), combined resection of other organs (P=0.022), long operation time (P<0.001), and JP drain insertion (P=0.015) were significant risk factors for overall complications (Table 5). Age ≥75 years (P=0.046), female sex (P=0.020), low phase angle (P=0.004), total gastrectomy (P=0.009), and long operation time (P=0.032) were significant risk factors for severe complications.
Table 5
Univariate analysis of risk factors for postoperative complications

Values are presented as number (%).
BMI = body mass index; ASA = American Society of Anesthesiologists; PNI = prognostic nutritional index; NLR = neutrophil/lymphocyte ratio; JP = Jackson-Pratt.
![]()
In multivariate analysis, two or more comorbidities (odds ratio [OR], 3.675; 95% CI, 1.1781–7.584; P<0.001) and hypoalbuminemia (OR, 4.059; 95% CI, 1.171–14.068; P=0.027) were independent risk factors for overall complications (Table 6). Female sex (OR, 2.993; 95% CI, 1.120–7.994; P=0.029) was an independent risk factor for severe complications. Low phase angle (OR, 2.901; 95% CI, 1.431–5.880; P=0.003 for overall complications; OR, 4.348; 95% CI, 1.478–12.791; P=0.008 for severe complications) and total gastrectomy (OR, 4.718; 95% CI, 2.098–10.607; P<0.001 for overall complications; OR, 3.473; 95% CI, 1.268–9.512; P=0.015 for severe complications) were independent risk factors for overall and severe complications.
Table 6
Multivariate analysis of risk factors for postoperative complications

Low hypoalbuminemia, serum albumin level <3.5 g/dL; low phase angle, phase angle <4.19° for females and <4.87° for males.
OR = odds ratio; CI = confidence interval.
![]()
DISCUSSION
Previous studies have shown that various clinical and surgical factors are associated with complications after gastrectomy. Although studies have shown variable results, risk factors for postoperative complications after gastrectomy are advanced age, high BMI, malnutrition, total gastrectomy, multiple comorbidities, extended lymphadenectomy, and advanced cancer stages [212223]. In this study, multiple comorbidities, hypoalbuminemia, female sex, total gastrectomy, and low phase angle were found to be independent risk factors for postoperative complications after gastrectomy in elderly patients with gastric cancer.
A standard definition for elderly or old age has not been established, and old age is determined by social, physical, and other factors. The age of patients undergoing surgical treatment has increased, but most developed countries have accepted the age of 65 years as the definition of “elderly” persons; therefore, in this study, elderly patients were defined as those aged ≥65 years.
Elderly patients are more likely to have many comorbidities, including cardiovascular, endocrine, and pulmonary comorbidities. In the present study, 38.6% of the patients had 2 or more comorbidities. These comorbidities are associated with postoperative complications [24], and multivariate analysis in this study also showed that comorbidities were independently associated with a higher complication rate and that patients with comorbidities tended to have a low phase angle.
BIA is a safe, noninvasive, and objective method to evaluate body composition. Phase angle is derived from the ratio of R and Xc, and these values are obtained with BIA. A low phase angle is a result of a decrease in Xc and an increase in R. Therefore, phase angle is considered as an indicator of cellular health, where higher values reflect stronger cell membranes and better cell function [20]. Phase angle is widely used to evaluate the nutritional status of various groups of patients [142526272829].
Several studies have reported that there is a strong association between malnutrition and postoperative complications. Sungurtekin et al. [30] reported that malnutrition is an indicator of postoperative complications in patients undergoing major abdominal surgery. Schiesser et al. [31] found that complication rates after gastrointestinal surgery were significantly higher in patients at nutritional risk: 40% of patients at nutritional risk versus 15% of patients not at nutritional risk. In our study, many nutritional indicators, including the phase angle, were associated with overall postoperative complications, but only the phase angle was an independent risk factor for overall and severe complications among all nutritional indicators.
Many previous studies have shown that the phase angle is an independent prognostic indicator in various clinical conditions such as liver cirrhosis, hemodialysis, human immunodeficiency virus infection, and several advanced cancers [1415161726], and these findings are consistent with our results. Postoperative complications adversely affect survival with advanced gastric cancer [32]; however, in this study, the relatively short follow-up period did not allow for the long-term evaluation of survival after gastrectomy. In our hospital, the phase angle has been calculated since August 2016. Based on the results of this study, we plan to evaluate the impact of the phase angle on long-term survival after curative gastrectomy for elderly patients with gastric cancer.
Phase angle is affected by age, sex, and BMI, and data is scarce regarding the reference value of phase angle in Asian populations [3334]. In this study, we restricted participants to elderly patients and the mean BMI of patients was not different between patients with and without complications, thus we divided the reference value of phase angle according to sex. The reference value of phase angle for Asian elderly patients requires investigation based on large clinical trials.
Unlike the results from other studies on postoperative complications after gastrectomy, female sex was identified as a risk factor for severe complications. Among the known risk factors, mean age and BMI were higher in women than in men, but the difference was not statistically significant. Other known risk factors were not significantly different between the sexes. The only variable that was statistically significant was the degree of obesity obtained using BIA, with female sex having a higher value. Moreover, the low incidence of severe complications (9.5%) is thought to have affected this result.
The strength of this study is that it is the first study to confirm the significance of the phase angle as a predictor of postoperative complications after gastrectomy for gastric cancer, especially in elderly patients. Moreover, most studies for phase angle determination have been conducted in the Western population; however, in this study, we analyzed the clinical impact of the phase angle in the Asian populations. In addition, we analyzed risk factors for postoperative complications using various nutritional indicators as well as the phase angle.
Our study had a few important limitations. First, it was retrospective, thus confounding, and bias might have affected the results. Second, a relatively small number of patients were analyzed, and the occurrence of severe complications was relatively low, which may have resulted in bias during the analysis. Thus, we plan to analyze a large number of patients to evaluate the relationship between the phase angle and postoperative complications. Third, body composition measured using BIA can be influenced by various factors such as patient fasting status and posture. Therefore, in our hospital, patients underwent the test after at least 8 hours of fasting and at least 15 minutes of resting and performed the same posture (holding the hand electrode loosely with both hands while standing upright on the foot electrode). In addition, the same examiner managed the examination process to obtain reliable results.
In conclusion, a preoperative low phase angle is an effective predictor of complications following gastrectomy for elderly patients with gastric cancer. We recommend that surgeons should perform BIA for elderly patients to obtain the phase angle before gastric cancer surgery, especially before total gastrectomy. Further studies are required to determine the cutoff value of the phase angles for the Asian populations and the prognostic impact of the phase angle on gastric cancer.
 XML Download
XML Download