

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
The mandible is the most significant and most durable bone of the skull. Its position is at the lowest point of the human face, beneath the maxilla. Aside from the ossicles of the middle ear, the mandible is the second movable bone of the skull1. The mandible is essential to the formation and function of the oral cavity. Its primary function is to form the lower jaw and hold the lower teeth in place. It also provides the support and foundation for tongue positioning and elevation of the larynx during swallowing2. Mandibular continuity defects that result from trauma, congenital deformity, or tumor resection have an impact on patients' physical function and aesthetics2. For functional rehabilitation of affected patients, the continuity defect must be restored immediately or as soon as possible3.
Through the course of history, many options for reconstruction after mandibular defect have been introduced, such as free bone grafts, vascularized rib, or alloplasts; however, these often did not result in optimal outcomes as expected45. In the mid-1970s, vascularized mandibular reconstruction was introduced and, since then, has become the standard protocol for the treatment of significant defects of the jaw6. The fibular free flap has become the most popular flap for mandible reconstruction because it can provide excellent bone stock with reliable anatomy, and the flap can be harvested using a two-team approach7. However, the morbidity of the donor site, a lengthy operation, and suboptimal aesthetics results are possible disadvantages of using this type of flap89. Another factor that should be considered is that in situations where the mandibular defect is due to the recession of a tumor, caution when choosing to perform vascularized free flap as the primary reconstruction protocol is warranted because of a high recurrence rate10. This approach should only be performed when no recurrence of the lesion is confirmed through oral and radiographic examinations.
The introduction of the metallic reconstruction plate (RP) in the 1980s provided an alternative treatment protocol for primary reconstruction of a mandibular defect. Such could be used to achieve stable fixation of free bone grafts and soft tissue reconstruction11. Another purpose of the RP is to bridge and maintain the position of the two free bone segments of a resected mandible, providing an adequate condition for subsequent reconstruction using a vascularized free flap if there is no recurrence of the lesion12. Although this technique has become popular in conjunction with vascularized free flap, a variety of complications including plate fracture, plate exposure, screw loosening, and infection through the mucosa or skin have been observed1314. A key reason for the failure of the RP system is most likely the high force created during masticatory movement of the patient15. Moreover, in cases with significant mandibular defects or when the defect is adjacent to/involves the condyle, placement of a long RP with limited to no space for screw fixation could prove to be inadequate for primary reconstruction. Consequently, a proposal for a new reconstruction option must be suggested.
Cone-beam computed tomography (CBCT), in combination with computer-aided design (CAD)/computer-aided manufacturing (CAM), has been previously used by clinicians to set up thorough and precise treatment plans for reconstruction surgeries. Throughout this process, a plastic model of the patient is made from the CBCT data. A surgical guide is then fabricated by CAD/CAM for assisting the clinician during the osteotomy procedure16. On the other hand, CAD/CAM technology has the advantages of creating a digital reconstruction of unilateral mandibular defects based on the anatomy characteristics of the unaffected side17. This idea involves the use of CAD/CAM to produce a customized implant (CI) for reconstruction of the mandibular defect of a specific patient. However, CIs for mandibular defects are difficult to design and produce because of the requirement to withstand high mechanical stress. Recently, there was a case report published that described a successful reconstruction of a mandibular defect using a CI produced by the combination of CAD/CAM technology and three-dimensional (3D) printing by electron-beam melting18. Although this could prove to be a promising treatment method for the reconstruction of mandibular defects, comparative studies between this new protocol and conventional protocols, especially in an animal model, are needed before it can be widely approved for use in humans.
In this study, mandibular defects were created surgically in a rabbit model. Because of the relatively small size of the rabbit's mandible as compared with the human's, five-hole titanium mini-plates without any bone graft were used as a RP system to reconstruct the defects in the control group, and CI by 3D printing was used to restore the deficiencies in the experimental groups. The aims of this study were to compare the efficiency of CI and RP in the reconstruction of mandibular defect in an animal model in regard to recovery indicated by daily food intake amount (DFIA) and screw status.
II. Materials and Methods
1. Implant fabrication
Pure titanium grade 1 spherical powder (average particle size, 35 mm) was used as a base material for 3D printing using the selective laser melting (SLM) method with the Realizer SLM300i system (Realizer, Borchen, Germany). Purified argon gas was then pumped into the chamber to prevent oxidation of the material. The CI was printed in a layer-to-layer pattern, with each layer being 25 mm thick. In terms of the processing parameters, a laser power of 200 W and a scan speed of 500 mm/s were applied. After the CI was printed, residual titanium powder was removed by using an ultrasonic cleaner.
2. Animal experiment
This experiment was approved by the Institutional Animal Care and Use Committee of Gangneung-Wonju National University, Gangneung, Republic of Korea (GWNU-2016-25). Fifteen New Zealand white rabbits were used for this study and were randomly assigned to one of two groups. The RP group (control group, n=5) received a five-hole mini-plate without any bone graft for reconstruction of the mandibular defect, while the CI group (experimental group, n=10) had their defect reconstructed by use of a CI instead. The CI group was then divided into two subgroups, a six-week CI (6WCI) group and a one-week CI (1WCI) group. The difference between these two subgroups was the amount of time from CI fabrication to the reconstruction surgery (six weeks vs one week). The 6WCI group used the CBCT data taken at six weeks before surgery for the manufacturing of the CI, while the CBCT data for the 1WCI group was taken at one week before the surgery.(Fig. 1)
In consideration of the mandibular defect, a bony segment measuring 5 mm in the right side of the mandibular body, between the molar and incisor, was chosen to be removed surgically to create the defect. A CBCT scan was performed on each rabbit, and surgical guides for the osteotomy procedure were manufactured using CAD/CAM technology. The CIs were then designed based on the individual CBCT data of each rabbit in the CI group. The printing process for the CI was already described in the previous section. The internal structure of the implant was designed to be as similar to the porous structure of original bone as possible, and the pore size was 800 mm.(Fig. 2)
The operation was performed with the rabbits under druginduced general anesthesia by an intramuscular injection of a combination of Zoletil 50 (15 mg/kg; Vibac Korea, Seoul, Korea) and Rompun (0.2 mL/kg; Bayer Korea, Seoul, Korea). Each rabbit was then injected with gentamicin (0.1 mL/kg; Samu Median, Seoul, Korea) and tolfenamic acid (0.1 mL/kg; Samyang Anipharm, Seoul, Korea) intramuscularly as preoperation medication.
After the hair had been shaved, the right mandibular area was disinfected with iodine solution and local anesthesia was administered. A submandibular incision on the right side of the mandible was performed and the skin and platysma muscle were incised while ensuring hemostasis. After exposure of the mandibular periosteum, a periosteal incision and subperiosteal dissection were performed. The right side of the mandibular body was exposed, and a surgical guide was used to mark the recession margin before vertical osteotomy. The defect was then created by the use of a reciprocating saw. Each mandibular defect was then reconstructed using the appropriate protocol depending on the group. For the RP group, a five-hole titanium mini-plate (MN/P SB 14MM 1.0T G3; OsteoMed, Dallas, TX, USA) and four mini-screws (20-MN-006 and 20-MN-008, diameter: 2.0 mm and length: 6.0 mm; Jeil Medical Corporation, Seoul, Korea) were used for fixation and reconstruction of the mandibular defect.(Fig. 3) Each rabbit of the CI group received their specific indicated CI for reconstruction, and micro-screws were used for the fixation of each implant.(Fig. 4) After review of the final positioning of the plates or CIs, closure by layer was performed using 4-0 Vicryl sutures (Johnson & Johnson, New Brunswick, NJ, USA). Gentamicin and tolfenamic acid were then injected intramuscularly after the operation.
Each rabbit was individually caged and received Purina Rabbit Chow (Purina Mills, Gray Summit, MO, USA) as food as well as water without any shortage. The functional recovery rate was assessed by measuring the daily food intake amount19, as calculated by the ratio between DFIA for each day postoperation and preoperative average DFIA (Equation 1). Individually, DFIA was measured for four days before the surgery and for 76 days postoperation.

Plain radiographic images (parallel technique) were obtained for each rabbit immediately postoperation and at monthly intervals thereafter using the X-ray generator HEL-S (Shinhung, Seoul, Korea) with 0.10 seconds of exposure time. The radiographic results were used to evaluated screw quantity between each time interval. All rabbits were then sacrificed humanely at the end of the observation period. During the sacrifice procedure, screw status and the presence of new bony ingrowth into the CI pores were evaluated. CBCT scans of each rabbit head were then taken post sacrifice for further evaluation of screw loosening based on changes in the positioning of the screw thread as compared with the appearance on the immediate postoperative plain radiographs. Screws that were entirely lost during the observation period were also be classified as being loosened for the purpose of this study. The screw status between groups was compared based on the percentage of screws that were intact versus loosened.
For the histologic analysis, the middle of the CI between the edges of the bony defect in each rabbit was cross-sectioned. Sectioned specimens were embedded in light-curing resin after a gradual dehydration process. Polymerized specimens were ground and polished20. The final thickness of the sliced specimens was 2 mm. Sections were stained with Goldner trichrome stain and examined under a light microscope.
3. Statistical analysis
The one-way ANOVA test was used to compare DFIA values between the RP, 6WCI, and 1WCI groups. If statistical significance was found, a post-hoc test was performed to compare each group to the other two groups. Tukey's test was chosen to be the post-hoc test and the statistical significance was set at P<0.05. The statistical analysis was performed using the IBM SPSS Statistics software program (ver. 25; IBM Corp., Armonk, NY, USA).
III. Results
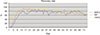
The average recovery rates of all groups are shown in Fig. 5. A similar pattern was observed in all groups. After reaching the peak average recovery rate after approximately three weeks, the rabbits maintained stable values for two months and then started to decline gradually until the end of the observation period. In terms of both the peak average recovery rate and the fastest average recovery rate, the 1WCI group showed the highest values out of all of the groups. The average time periods required to achieve 50% and 80% recovery for each rabbit in each group are presented in Fig. 6. The 1WCI group required 2.6±1.3 days and 8.2±3.3 days to reach 50% and 80% recovery, respectively. The 6WCI group required 7.8±2.3 days and 10.8±1.8 days to reach 50% and 80% recovery, respectively. Finally, the RP group required 4.6±1.5 days and 7.8±2.2 days to reach 50% and 80% recovery, respectively.
The one-way ANOVA test showed statistically significant differences between the average days required for 50% recovery of the 6WCI, 1WCI, and RP groups (P=0.002). However, there were no statistically significant differences between the average days required for 80% recovery among the groups. More specifically, there was a statistical difference between the 6WCI group and RP group at 50% recovery (P=0.035), while the difference between the 6WCI group and 1WCI group was also statistically different at 50% recovery (P=0.001). However, there was no statistical difference between the 1WCI group and RP group at 50% recovery. During the observation period, all of the rabbits achieved a recovery rate of more than 90%.
The numbers of screws (35 and 20, respectively) in the 1WCI group and RP group did not change during the observation time. In the 6WCI group, at both the one-month and two-month intervals, the remaining screws numbered 28 (84.9%), while, at the point of sacrifice, there were 26 screws present in the 6WCI group (78.8%), for a total of seven screws lost during the observation time in this group. Of all groups, the 1WCI group maintained the highest percentage of intact screws (94.3%). The percentages of intact screws in the 6WCI group and RP group were 75.8% and 85.0%, respectively.(Table 1)
During the observation time, there was one rabbit in the 6WCI group that showed a complication of wound infection with CI exposure at one month postoperation, while another rabbit in the same group presented a similar condition at two months postoperation. Both were treated with the same medication as was given immediately postoperation for three days and daily dressing using iodine solution. At the end of the observation period, both showed complete healing of their secondary wounds. The other rabbits showed no sign of postoperative complications. At sacrifice, only one rabbit in the 6WCI group demonstrated instability of the CI, and no evidence of new bone generation was found in this rabbit. All other CIs and plates were stable at the time of sacrifice.(Fig. 7) In general, the rates of CI exposure and unstable CI in the 6WCI group were 40% and 20%, respectively.
According to the CBCT data after the sacrifice, there was confirmation of successful new bone generation in the rabbits of the CI group with no loosened screws.(Fig. 8. A) In the case of a rabbit that had one loosened screw at sacrifice, a lower level of bony regeneration was still observed in the margin area around the CI.(Fig. 8. B) Histologic examination of the rabbits with no loosened screws showed evidence of bony ingrowth into the pores structure of the titanium CI structure.(Fig. 9. A) In the case of the rabbit with plate exposure and unstable CI, bony ingrowth into the CI was not observed.(Fig. 9. B)
IV. Discussion
In this study, DFIA was used as a primary indicator to demonstrate the recovery rate of each rabbit2122. As shown in Fig. 5, the 1WCI group achieved the highest value in terms of peak average recovery rate and fastest average recovery rate. With respect to reaching a 50% recovery rate, the 1WCI group also required the least mean average number of days of all three groups (2.6±1.3 days). Although the difference between 1WCI group and RP group was not statistically significant, we could infer that the use of CI as a treatment protocol for reconstruction of a mandibular defect could accelerate the speed of rehabilitation better than the RP system. This finding could be explained by the fact that the CIs were created with the same anatomical characteristics as the mandibular defect through the combination of CBCT and CAD/CAM technology. Moreover, the advantage of 3D printing enables the possibility of creating porous structures from a metallic material to mimic original bone23. The result is an ideal CI designed with an almost identical external shape to that of the mandibular defect and containing a porous internal structure to enhance bone ingrowth.
The 1WCI group required 2.6±1.3 days to reach 50% recovery, while the 6WCI group required 7.8±2.3 days. There was a statistically significant difference between these two groups (P=0.001). As mentioned above, the difference between these subgroups was that the 6WCI group used the CBCT data taken six weeks before surgery for the manufacturing of the CIs, while the CBCT data used for the same in the 1WCI group were taken at one week before the surgery. It should also be noticed that the 6WCI group was the only group that had missing screws according to plain radiography review at monthly intervals and at sacrifice. Coincidentally, two rabbits in the 6WCI groups, which had missing screws, also showed signs of infection and plate exposure. At sacrifice, one of them even showed instability of the CI. However, no signs of complication were observed in the 1WCI group. It could be suggested from this finding that the CBCT data used for the manufacturing of CI could have an essential role in treatment protocols using CIs as means of reconstruction. The time factor could affect the outcome of this treatment procedure. More recent CBCT data will provide a better foundation for more accurate CIs. In this study, 6WCI groups used the CBCT data collected at six weeks before the operation. The length of time, in conjunction with the fast-growing rate of rabbits, made these CBCT data inappropriate for the manufacturing of CIs in this group. This factor should be considered when using CIs for reconstruction surgery in a human. In cases of mandibular defects related to tumors, the growth rate of the tumor or the recurrence of a tumor could affect the size of the defect24, leading to a mismatch of the designed CI and the defect. The timing of CBCT data collection should be selected carefully to ensure a more precise evaluation of the defects is completed so as to increase the accuracy of CIs for reconstruction of the particular defect.
The screw-loosening rate of the 1WCI group was the lowest among all of the groups. In a related fashion, when comparing the intact screw rate, the 1WCI group showed a higher percentage of such than the RP group. It is possible that the mandibular morphogenesis was influenced by a series of stress factors induced masticatory muscle forces25. The shape of the mandible is suitable for the distribution of occlusal forces in different horizontal mandibular positions. The appearance of a mandibular defect may decrease the masticatory efficiency of a patient because of discontinuation of the mandible26. Another factor able to contribute to stress distribution is the degree of surface contact between the reconstruction replacements and the bony segments of the mandible. A higher degree of surface contact will reduce stress concentrated on the reconstruction replacements and improve their stability, which has been reported in a previous comparison study between carbon plates and RPs27. In mandibular reconstruction using the RP system, the interface between the plate and screws is usually put under stress created by masticatory movement28. Continuous stress on the plate and screws could be one of the reasons for screw loosening, which has already been reported in prior research29. To avoid stress concentration, the screw alignment should be designed in a non-linear formation, which is hardly possible in an RP system30. In the present study, the CIs were designed with a mesh structure connected by a titanium plate. The CI ultimately fulfilled three factors that could reduce stress concentration: (1) The shape of the CI mimicked the original defect to recreate the continuous span of the mandible; (2) the CI had a wider contact area with the bony segments compared with an RP; and (3) the screw formation in the CI was designed to appear in a zig-zag formation, which enabled equal stress distribution between screws.
Despite the advantages of CIs compared with RPs as mentioned above, screw loosening was still observed in the CI groups at a relatively low rate, suggesting a slight degree of mismatch between the CIs and the mandibular defect, even in the 1WCI group. There could be an explanation for this finding. Incorrect positioning or design of the surgical guide could lead to incorrect osteotomy31. These errors could occur during planning procedures or the surgery itself. Examples of errors in planning procedures could be the use of inappropriate CBCT data or overlapping the CBCT data and 3D images. Errors during surgery can happen if the guide is not placed accurately or the guide is moved due to unwanted forces during the osteotomy. There have been many studies emphasizing the importance of using a precise surgical guide in the conduct of surgery based on CAD/CAM technology16. To prevent such errors, the CBCT data should be evaluated carefully for better fabrication of both the surgical guide and CI, as mentioned above. The surgical guide could also be designed with landmark indicators such as the host's teeth for precise placement or could include fixation holes for better stability during osteotomy.
In this study, some but not all CIs allowed bony ingrowth into the porous structures. To allow for bony ingrowth, initial stability of the CI must be achieved immediately following CI fixation, which is similar to the case of dental implant osseointegration32. Intermaxillary fixation could be an additional procedure performed during the initial stage of recovery to enhance the stability of CI by avoiding masticatory movement. However, this procedure may be impossible to complete in an animal experiment. A soft diet could also be recommended during the recovery stage to reduce high masticatory forces. However, a prescribed change of diet could affect the DFIA pre- and postoperation, which eventually may lead to errors in calculating the recovery rate.
The 1WCI group showed better efficiency in terms of the recovery rate compared with the RP group. However, the difference was not statistically significant, which could be because the use of DFIA as the only indicator of recovery rate affected the statistical analysis. Another indicator such as average body weight should also be considered to more accurately determine the difference among groups.
Achieving dental rehabilitation was not the main aim of this research. Future designs for CIs should consider the inclusion of dental implants as an additional goal before being applied in fully rehabilitating patients.
V. Conclusion
In conclusion, rabbits with mandibular defects treated using CIs for reconstruction showed higher and faster recovery rates of their DFIA than those treated with five-hole mini-plates without bone grafts. However, this could only be achieved with precise utilization and careful evaluation based on more recent CBCT data. The screw status showed favorable results in the CI group, which showed higher screw intact and lower screw loosening rates compared with the RP group. The CI group showed bony ingrowth into the porous structure; however, precise fabrication and placement of the surgical guide for the planned position were required for accurate osteotomy in the CI group. Future design of CIs should require consideration of dental implants in fully rehabilitating patients.









 XML Download
XML Download