

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Ehlers-Danlos Syndromes (EDSs) are a group of heritable connective tissue disorders characterized by defects in the structure and synthesis of connective tissue. Defective connective tissue can lead to a myriad of clinical problems such as frequent joint dislocations, early-onset osteoarthritis, extensive bruising, abnormal scarring, delayed wound healing, periodontal disease, arterial dissections and aneurysms, hernias, bladder and bowel dysfunction, dysautonomia, sleep disorders, fatigue, headaches, paresthesia, numbness, Chiari malformation, and scoliosis [12345]. Pain is a common co-morbidity in these disorders [4678].
Small case series [91011] suggest that people with EDS may experience local anesthetic (LA) resistance, defined as the failure of LA to provide pain prevention using typical dental practice methods, more often than the general population. However, large surveys are lacking, limiting the estimates of the magnitude of this issue. The primary goal of this hypothesis-generating study was to determine the recalled adequacy of LA administered during dental procedures in a large cohort of people with and without EDS. A secondary exploratory aim asked people with EDS to recall the relative efficacy of local anesthetics used in their dental procedures.
At a two day meeting funded by the Patient Centered Outcomes Research Institute (PCORI), local anesthetic resistance was among the top priorities chosen by the Ehlers-Danlos Co-morbidity Coalition [12]. The charge of the meeting was to follow PCORI patient engagement methodology standards in generating research priorities [13].
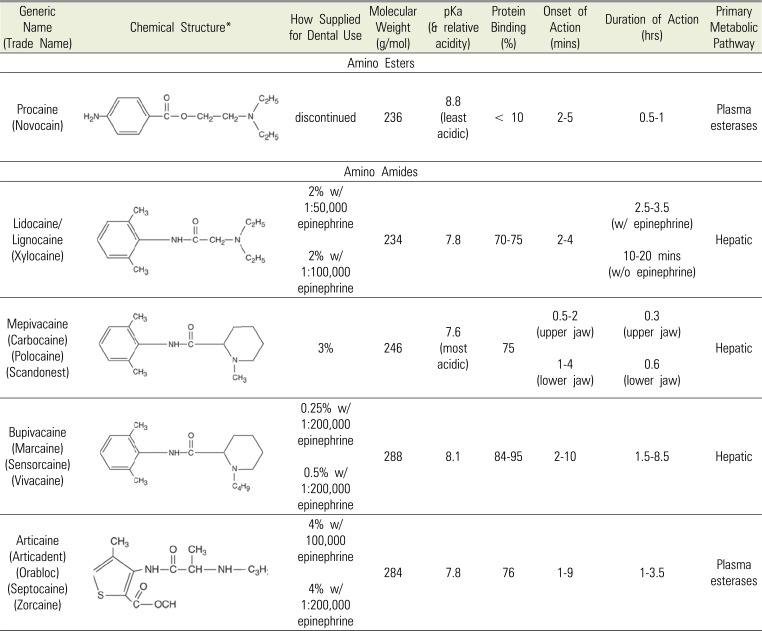
Experiencing pain during dental procedures can be traumatic and painful. LAs, such as lidocaine, mepivacaine, bupivacaine, or articaine are routinely used to prevent procedure-associated pain. The common factors that can influence analgesic effectiveness of the LA procedures include the physicochemical properties of the specific LA being used, the target nerve that is being blocked, and the addition of adjuncts or vasoconstrictor that is co-administered, among many other factors. For example, several studies have pointed out that the anesthetic success depends on the specific tooth involved [141516], and that it is easier to achieve in the upper jaw (maxillary region) compared to the lower jaw (mandibular region). The other patient related factors also include the rate of drug absorption, dispersion and metabolism, genetic variation in anesthetic target site structure or function or in rates of nociceptive pain transmission, the presence or absence of local inflammation, and anatomic variations in peripheral nerve locations. The mechanisms of local anesthetic resistance in EDS are not known.
Go to : 
METHODS
We administered an online survey focused on the recalled adequacy of pain prevention with LA administered during dental procedures using Research Electronic Data Capture (REDCap) [17], a secure, browser-based application for managing online surveys and research databases housed at Vanderbilt University. This study was approved by the Institutional Review Board of Vanderbilt University (IRB# 180954). Participants gave their informed consent electronically.
The REDCap survey was distributed in the English language world-wide by the Ehlers-Danlos Society through various social media platforms (Facebook, Instagram, Twitter, weekly newsletters, and their message board on Inspire). The pushes of the survey occurred across these platforms three times in 2018 (June, September, and November). In addition, the Ehlers-Danlos Society Comorbidity Coalition [12] member organizations distributed the survey to their members. Individuals with EDS and their friends who did not have EDS were asked to complete the survey.
The primary objective of the survey was to compare self-reported rates of subjective LA resistance among individuals with and without EDS. The secondary objective was to compare subjective LA effectiveness (among various LA from the same drug class) in the subset of individuals with EDS who reported experiencing past LA problems.
Survey respondents were stratified into the EDS cohort and non-EDS cohort by their responses to survey questions which listed EDS and 9 other comorbid disorders. Responses could be selected from among the following: “Yes,” “No,” “Not sure,” and “Don't Want to Say.” Those who answered “Not sure” and “Don't Want to Say” were excluded from further analysis. Respondents who indicated a problem with LAs were asked additional questions related to the effectiveness of specific agents and any alternative pain control methods they have used to augment the lack of LA efficacy.
For statistical analysis, we focused on respondents who had ever received a LA ( > 98% of the sample). A chi-squared test was used to compare groups (EDS and non-EDS respondents) for responses to the question “Have you ever had a problem with a local anesthetic not working adequately or properly?”
For respondents with EDS who had received LA, we calculated the percentage who reported adequate pain control separately for each specific agent received (lidocaine, procaine, bupivacaine, mepivacaine, and articaine). To evaluate whether EDS respondents indicated anesthetic failure to all LA or whether some of them worked better than others, we focused on respondents who received ≥ 2 specific agents. For each selected combination of agents, we calculated the percentage of respondents in which both agents, neither agent, and only 1 agent provided adequate pain control. Excluded from this analysis were respondents that selected “Not sure” or “Don't want to say” to the question about adequate pain control for either agent in the combination. EDS respondents who received 3 or more of the selected agents were included in the analyses for all respective combinations.
Go to :
RESULTS
The demographic characteristics of those included in the analysis are provided in Table 1. A total of 1,691 individuals responded to the survey; however, 448 of those were excluded as a result of either not answering the question related to consent (n = 49), not providing consent for the study (n = 6), not completing the survey in its entirety (n = 296), or having answered “Don't Want to Say” or “Not sure” for the question regarding a diagnosis of EDS (n = 97). These exclusions left 1243 responses: 988 in the EDS group and 255 in the non-EDS group. The overwhelming majority of the respondents were female (92%), white (91%), non-Hispanic (94%), and from the United States (73%).
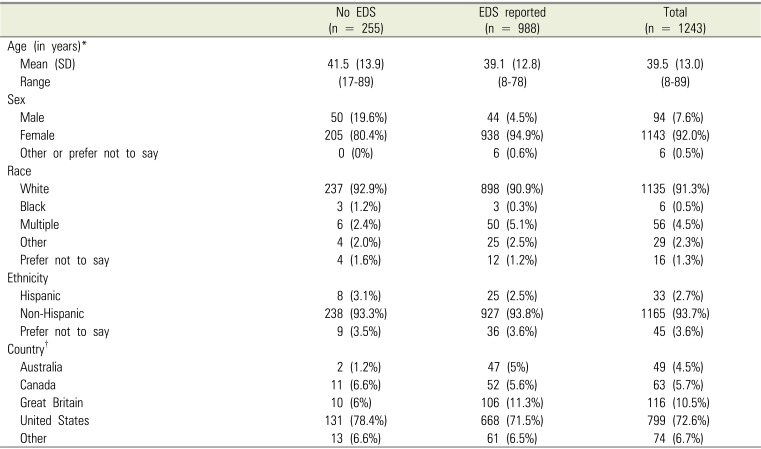
Table 1
Demographic characteristics of survey responders, stratified by EDS status
![]()
Among EDS respondents, 980 (99%) indicated they had been given a dental procedure-associated LA in the past, with nearly 88% (n = 860) of those indicating it did not provide adequate anesthesia at some point in time. Among non-EDS respondents, 249 (98%) indicated they had been given a dental procedure-associated LA in the past, with 33% (n = 83) of those indicating it was not effective at some point in time (P < 0.001 compared to EDS respondents) (Table 2).

Table 2
Use of local anesthetics, stratified by EDS status
![]()
Table 3 summarizes data among respondents with EDS who indicated that they had received at least one local anesthetic (n = 980). As respondents could select more than one, the drug categories are not mutually exclusive. The two most common agents that EDS respondents reported having received were lidocaine (69%, n = 676) and procaine (64%, n = 623). Bupivacaine (18%, n = 169), mepivacaine (5%, n = 50), and articaine (4%, n = 40) were less common. Of those that reported having ever received lidocaine, only 8% indicated that it provided adequate pain relief during the procedure, and only 7% of those who reported having ever received procaine indicated it was effective. The agent with the highest respondent-reported success rate was articaine (30%), followed by bupivacaine (25%), and mepivacaine (22%).

Table 3
Survey responses for the EDS cohort who reported ever having received a local anesthetic injection (n = 980)
![]()
Table 4 focuses on EDS respondents who received at least 2 of the 4 most common agents. For most combinations, if a survey responder indicated that one sodium channel blocker did not provide adequate pain control, another sodium channel blocker they reported as receiving at some point was also reported as unsuccessful (see the “Neither provided adequate pain control” category for each pair), ranging in frequency from 69–86%. This was true regardless of whether the sodium channel blocker was an amino ester (procaine) or an amino amide (lidocaine, mepivacaine, bupivacaine). Approximately 71% (n = 608) of EDS respondents who reported having a problem with a local anesthetic in the past also reported having tried at least one other agent in the same drug class.
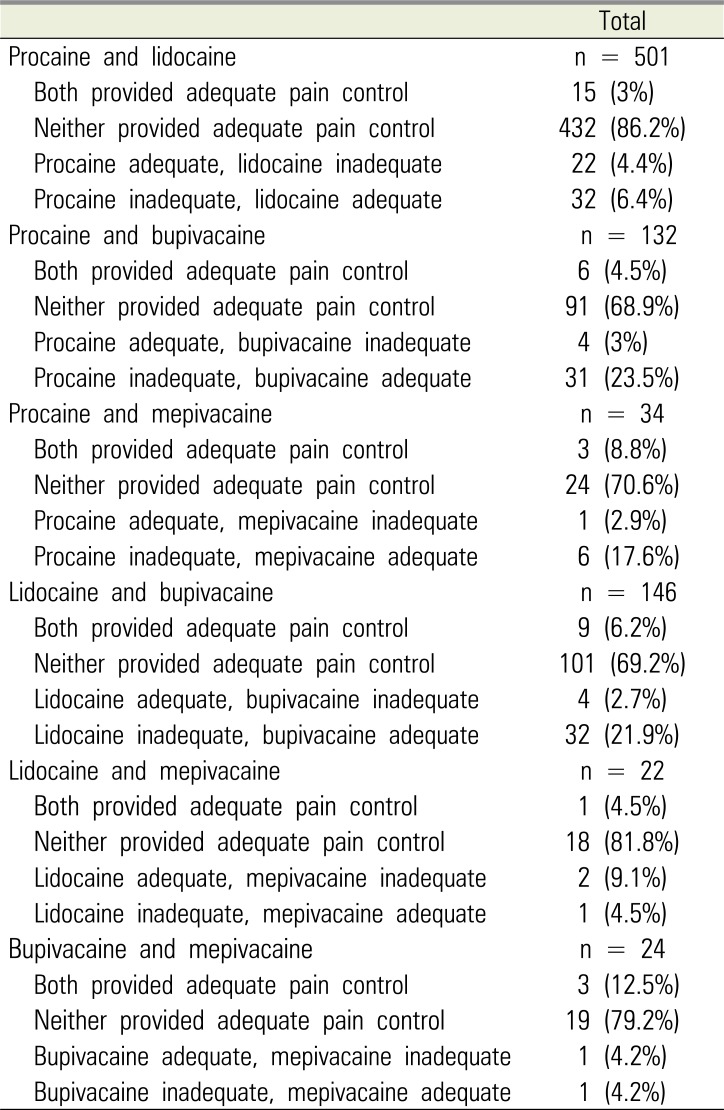
Table 4
Survey responses for the EDS cohort who reported ever having received a local anesthetic injection (n = 980)*
![]()
We also analyzed the types of alternative pain control strategies utilized among EDS respondents who indicated they had encountered a problem with the use of a local anesthetic (n = 860): 45% (n = 383) indicated use of alternative strategies prior to the procedure to help manage pain during the procedure, and 73% (n = 630) indicated use of alternative strategies post-procedure. The most common drug therapies used among EDS respondents in both pre- and post-procedural pain management were non-steroidal anti-inflammatory drugs (NSAIDs) (74% pre-procedure and 81% post-procedure) followed by acetaminophen/paracetamol (71% pre-procedure and 79% post-procedure), and opioids (56% pre-procedure and 66% post-procedure). Cryotherapy (use of ice packs) was the most commonly utilized method reported of all post-procedural strategies (84%). Mindfulness and other similar types of relaxation techniques were commonly reported in both pre- procedural (67%) and post-procedural settings (71%).
Go to :
DISCUSSION
These retrospective survey data indicate that people with EDS report a dental local anesthetic injection that “did not work” at nearly three times the rate of those without EDS (88% vs. 33%). This suggests that local anesthetics are less effective in preventing or reducing pain during routine dental procedures, a phenomenon that has been called “local anesthetic resistance.” Marhofer et al. (2014), in a small study, pre-specified a meaningful clinical difference as 30% for failure of dental anesthesia [18]. The Cochrane Systematic Review of Injectable Local Anesthetic Agents for Dental Anesthesia reported a success range of 31% to 83% [19].
Our second aim sought evidence of differences in effectiveness between dental local anesthetic agents. This suggests that the most effective local anesthetic agents among EDS respondents are articaine, bupivacaine, and mepivacaine, with lidocaine and procaine reported as effective far less often. The most effective agent (articaine) was effective in only 30% of people with EDS.
Strengths of our study include the large sample obtained by leveraging the Ehlers-Danlos Society's access to large numbers of people with these heritable disorders. The higher response by people with selfidentified EDS (n = 988) compared to people without identified EDS (255) is likely because the survey was distributed through social media platforms used by people with EDS. Acknowledging the limits of recall data and the hypothesis generating intent of this work, the EDS community is highly attuned to their medical history and in the authors' clinical experience typically provide accurate details of their past care. The primary limitation of this survey is that it is a non-random convenience sampling of people with self-identified EDS and people without identified EDS. The results of the convenience sampling cannot be generalized to all people with EDS because of the potential, unmeasurable, bias of the sampling technique. Additional difficulties inherent to survey research include respondents' variable interpretation of questions, accuracy of recall, and lack of confirmatory measures or data sources. We did not ask about specific locations of the dental procedures and associated site of anesthesia.
The results of our study, performed on a relatively large cohort of people with EDS, are in agreement with previously published observations in a smaller number of patients [91011]. A 2003 single site survey, focused on women with symptomatic joint hypermobility syndrome (JHS), asked the question “If you have ever had a local anaesthetic injection (dentist/minor surgery/epidural), did you think that it was as effective as it should have been?” Among those with symptomatic JHS, 58% recalled poor pain control efficacy. Among the two matched control groups (women without joint hypermobility and women with non-symptomatic JHS), poor pain control efficacy was 21% and 14%, respectively [11]. JHS is a historic rheumatologic classification for people with symptomatic generalized joint hypermobility.
Small studies investigated analgesic effects in people with EDS using controlled sensory testing. Arendt-Nielsen and colleagues [9] compared the analgesic effect of intradermal lidocaine infiltration in 8 people with EDS type III (now termed the hypermobile type) and 8 controls. Pain (assessed by thresholds to short argon laser stimulation) was prevented in both groups when assessed 5 minutes after lidocaine cutaneous infusion. However, an hour later the analgesic effect was no longer present for those with EDS, but did persist in the controls. A subsequent study evaluated cutaneous analgesia using a weighted needle pinprick sensory threshold in 7 people with EDS, 10 people with non-EDS hypermobility and 15 controls. A local anesthetic cream applied up to 2 hours did not achieve full analgesia in the people with EDS, but did so in the people with non-EDS hypermobile and also in the controls. The people with EDS had lower thresholds to pain stimulation [10].
Seeking to understand local anesthetic resistance in a large patient sample, (not characterized with respect to EDS), Trescot interviewed 1,198 pain center patients; 250 reported difficulty getting numb from injections and subsequently were tested for LA resistance. Ninety, representing 7.5% (90/1198) of the total were found to be hypoesthetic only to mepivicaine, and an additional 3.6% (43/1198) only to lidocaine. The rest were hypoesthetic to all or bupivacaine [20], suggesting that drug specific factors may influence anesthetic effectiveness.
A 2018 review summarized a decade of research on the efficacy of dentistry-associated LA use in general population [21]. Of 30 studies reviewed, 11 found that articaine provided better analgesia versus lidocaine; 3 found articaine superior to bupivacaine; and 2 found articaine superior to mepivacaine; 3 found mepivacaine to lidocaine to be similar, while 2 found mepivacaine to be superior to lidocaine; and 2 found bupivacaine superior to lidocaine. A 2018 Cochrane review by George et al. presented similar findings [19].
Differences in pharmacokinetic or pharmacodynamic responses to LA could contribute to variability. Inherited differences in the structure or function of VGSC could lower LA efficacy by altering the drug binding sites or downstream signaling. There are many examples of so-called channelopathies caused by point mutations in VGSC genes in which the channels are less responsive to LA [22].
Human cytochrome P450 3A4 is the most abundant isoform of P450 enzyme (CYP) in the liver. It plays an important role in the metabolism of wide variety of xenobiotic and endogenous substrates. Genetic polymorphism of CYP3A4 can greatly influence the rate of elimination of lidocaine, thereby may result in adverse effects or therapeutic failures [23]. It is possible the EDS patients as a group may display higher variant allele frequencies which result in alteration of hepatic metabolism of other LA (e.g., mepivacaine metabolized by CYP1A2//3A4 and bupivacaine metabolized by CYP3A4), however this has not been tested.
Tissue factors possibly related to abnormal connective tissue (e.g., skin laxity) may be involved, but are not understood at present. Prior studies have concluded the dispersion rates of LA through the tissues after deep dermal injections were identical for EDS and control subjects [24]. If lack of local anesthetic effectiveness is not due to differential, rapid dispersal of solution, then increasing the amount of drug will not compensate for lack of effectiveness. Tissue factors could also affect pain perception or transmission. Research studies in animals indicate that genetic mutations frequently seen in some types of matrix proteins could affect pain transmission of peripheral nociceptive neurons [2526].
The presence or absence of inflammation may alter the efficacy of a local anesthetic [27282930]. Vasodilation will hasten the diffusion of local anesthetic drugs away from the area, thus reducing their efficacy. People with EDS often have chronic, wide-spread mast-cell activation [31] (with increased inflammation), which may explain why some LAs can work differently than other in people with EDS [32].
Another host factor relates to the accumulated impact of repeated painful experiences. Many people with EDS live with chronic pain and high anxiety [33] and often experience a phenomenon known as “wind-up pain”, with prolonged, persistent release of neurotransmitters involved in pain pathways. This results in the up-regulation of physiologic pathways that ultimately cause people to experience pain from otherwise non-painful stimuli (allodynia) and an exaggerated amount of pain during painful episodes (hyperalgesia). This phenomenon may make achieving adequate anesthesia difficult for people who deal with chronic pain, and may be the cause for increased failure of local anesthetics in people with EDS. Prior failure of LA may contribute to central sensitization, thus exacerbate the pain experience in subsequent procedures [34].
In summary, our patient survey suggests that people with EDS suffer from LA resistance at a rate much higher than people without EDS. The increasing attention to this research question reflects the success of the PCORI patient engagement methodology through which patients are at the table during the generation of research priorities. Patients attending the EDS Co-Morbidity Coalition meeting identified dental procedure pain as a traumatic, routine event that was part of their lived experience. While human resistance to LAs has been documented, and sometimes explained [3435], the basis for LA resistance in people with EDS is unknown. Prospective, double-blind studies are needed to verify if LA resistance in people with EDS can be objectively documented, and if this varies by specific types of LA, and by EDS subtypes. The sheer magnitude of this phenomenon among people with EDS compels additional research into the cause, and a search for practical pain prevention strategies.
Go to :
 XML Download
XML Download